You might also like
- Immunization RecordDocument4 pagesImmunization RecordVin BitzNo ratings yet
- NeonatologiDocument19 pagesNeonatologiariandhitaNo ratings yet
- Recording Forms (Masterlist) School Forms - Kinder To Grade 7Document16 pagesRecording Forms (Masterlist) School Forms - Kinder To Grade 7lourdes estopaciaNo ratings yet
- 2017 Access To Vaccines IndexDocument102 pages2017 Access To Vaccines IndexMohamedRefaatMohamedNo ratings yet
- Universalimmunisationprogram 171120044520Document22 pagesUniversalimmunisationprogram 171120044520Gagan GargNo ratings yet
- Expanded Program On ImmunizationDocument9 pagesExpanded Program On Immunizationnichiichaii100% (1)
- Immunisation History Statement 3Document2 pagesImmunisation History Statement 3Fordham JessNo ratings yet
- Recording Form 1: Masterlist of Grade 1 Students: School-Based ImmunizationDocument1 pageRecording Form 1: Masterlist of Grade 1 Students: School-Based ImmunizationJesse100% (1)
- Recording Forms Masterlist School Forms Kinder To Grade 7 2Document16 pagesRecording Forms Masterlist School Forms Kinder To Grade 7 2Nimfa AsuqueNo ratings yet
- SBI MASTERLIST Grade 7Document2 pagesSBI MASTERLIST Grade 7Eden Jane CaparasNo ratings yet
- VaccineDocument4 pagesVaccineFe marikitNo ratings yet
- RECORDING Form 1: MR-TD (6-7 Years Old) : Community-Based Immunization ActivityDocument4 pagesRECORDING Form 1: MR-TD (6-7 Years Old) : Community-Based Immunization ActivityMay John Delos SantosNo ratings yet
- Sbi FormsDocument70 pagesSbi Formsdiomedescolar.13No ratings yet
- No. Name (1) (Surname, First Name, MI) Complete Address (2) Age Sex 1 Date of Birth Mm/Dd/YyDocument6 pagesNo. Name (1) (Surname, First Name, MI) Complete Address (2) Age Sex 1 Date of Birth Mm/Dd/YyMADELYN U.ULITANo ratings yet
- School - BAsed Immunization Recording FormDocument14 pagesSchool - BAsed Immunization Recording FormErnest Jerome Malamion100% (4)
- To Be Filled Up by The Teacher/Adviser To Be Filled Up by The Vaccination TeamDocument8 pagesTo Be Filled Up by The Teacher/Adviser To Be Filled Up by The Vaccination TeamGlenn L. Ravanilla100% (1)
- School Based Immunization Form Grade 1Document1 pageSchool Based Immunization Form Grade 1maristellaNo ratings yet
- Recording Form 1: MR TD Lot No: Lot No: Batch No: Batch NoDocument1 pageRecording Form 1: MR TD Lot No: Lot No: Batch No: Batch NoJean Francis ReyesNo ratings yet
- Final Draft - Community-Based Immunization (CBI) Recording Form-1 MR - TD 6-7 Years OldDocument101 pagesFinal Draft - Community-Based Immunization (CBI) Recording Form-1 MR - TD 6-7 Years OldDOMINADOR PANOLINNo ratings yet
- SBI Recording Form 1Document12 pagesSBI Recording Form 1Maybel Din0% (1)
- Form 3 - HPV Masterlistingv Form - UECSDocument6 pagesForm 3 - HPV Masterlistingv Form - UECSJEROMENo ratings yet
- SBI Recording and Consolidation Form LatestDocument46 pagesSBI Recording and Consolidation Form LatestMannielle MeNo ratings yet
- SBI Recording and Consolidation FormDocument46 pagesSBI Recording and Consolidation FormLee-Ann ZerimarNo ratings yet
- RECORDING Form 1: MR-TD (6-7 Years Old) : Community-Based Immunization ActivityDocument2 pagesRECORDING Form 1: MR-TD (6-7 Years Old) : Community-Based Immunization ActivityLiza Domingo100% (2)
- Recording Form1 DohDocument1 pageRecording Form1 DohReyno D. Paca-anasNo ratings yet
- RECORDING Form 1: Masterlist of Students Masterlist of Kinder 1 To Grade 7 (Except Grade 4)Document2 pagesRECORDING Form 1: Masterlist of Students Masterlist of Kinder 1 To Grade 7 (Except Grade 4)Mary Luz ManaliliNo ratings yet
- RECORDING Form 1: Masterlist of Kinder - Grade 6 Students: School-Based ImmunizationDocument2 pagesRECORDING Form 1: Masterlist of Kinder - Grade 6 Students: School-Based ImmunizationRhealyn Eje TorresNo ratings yet
- Application Form For AdmissionDocument2 pagesApplication Form For AdmissionApr CelestialNo ratings yet
- Recording Form1 Masterlist of Grade 1 StudentsDocument1 pageRecording Form1 Masterlist of Grade 1 StudentsSandra Nicole TorresNo ratings yet
- Vi Virgo Masterlist MeaslesDocument57 pagesVi Virgo Masterlist Measlesbess0910No ratings yet
- RECORDING Form 1: Masterlist of Grade 1 Students: School-Based ImmunizationDocument3 pagesRECORDING Form 1: Masterlist of Grade 1 Students: School-Based ImmunizationChaterine Joy MasayonNo ratings yet
- CatchUp Form TemplateDocument7 pagesCatchUp Form TemplateGinalyn Gine- GarduqueNo ratings yet
- Community Base ImmunizationDocument3 pagesCommunity Base ImmunizationZhaine MendozaNo ratings yet
- RECORDING FORM 1: Masterlist of Grade 1 Students: Galas Elementary School Zn/Dipolog City Dipolog City Division City WestDocument1 pageRECORDING FORM 1: Masterlist of Grade 1 Students: Galas Elementary School Zn/Dipolog City Dipolog City Division City Westadonis_abellanosaNo ratings yet
- Master List Measles Grade 6 TWODocument8 pagesMaster List Measles Grade 6 TWOjoemer mabagosNo ratings yet
- Immunization 2019 SJES BlankDocument14 pagesImmunization 2019 SJES BlankBeaJanelleMacalaladNo ratings yet
- RECORDING Form 1: Masterlist of Grade 1 Students: School-Based ImmunizationDocument19 pagesRECORDING Form 1: Masterlist of Grade 1 Students: School-Based ImmunizationnorhataNo ratings yet
- School-Based ImmunizationDocument1 pageSchool-Based ImmunizationJenevieve Odtojan BajanNo ratings yet
- Form-1-3-MR-TdHPV-Masterlisting-Form-1 HESTIADocument3 pagesForm-1-3-MR-TdHPV-Masterlisting-Form-1 HESTIAMay John Delos SantosNo ratings yet
- Necropsy Sample Submission Form SWDocument2 pagesNecropsy Sample Submission Form SWAlberto UribelyNo ratings yet
- Adverse Events Following Immunization: Philippine Integrated DiseaseDocument2 pagesAdverse Events Following Immunization: Philippine Integrated DiseaseRex DoctoNo ratings yet
- To Be Filled Up by The School Nurse/ Class Adviser To Be Filled Up by The Vaccination TeamDocument13 pagesTo Be Filled Up by The School Nurse/ Class Adviser To Be Filled Up by The Vaccination TeamShinSan 77No ratings yet
- Aefi Case Reporting Form (CRF)Document2 pagesAefi Case Reporting Form (CRF)Saumyasankar Sarangi86% (22)
- RECORDING Form 1: Masterlist of Grade 1 Students: School-Based ImmunizationDocument9 pagesRECORDING Form 1: Masterlist of Grade 1 Students: School-Based ImmunizationShiela Isip SaliNo ratings yet
- RECORDING Form 3: HPV Masterlist of FEMALE 9-14 Years Old: Community-Based Immunization ActivityDocument1 pageRECORDING Form 3: HPV Masterlist of FEMALE 9-14 Years Old: Community-Based Immunization ActivityLiza Domingo0% (1)
- School-Based Immunization Masterlist of Learners GradeDocument9 pagesSchool-Based Immunization Masterlist of Learners GradeRamuel Edrian Tugade PelayoNo ratings yet
- Community-Based Immunization Activity RECORDING Form 2:MR-Td (12 - 13 Years Old)Document1 pageCommunity-Based Immunization Activity RECORDING Form 2:MR-Td (12 - 13 Years Old)MERRIAN SIBOLINAONo ratings yet
- 7 M None X R-11/1/21 Religion: RECORDING FORM 1. MR-TD (6-7 Years Old)Document3 pages7 M None X R-11/1/21 Religion: RECORDING FORM 1. MR-TD (6-7 Years Old)Jasmin Kerre Villarin100% (1)
- Tirumala Tirupati Devasthanams: TirupatiDocument2 pagesTirumala Tirupati Devasthanams: TirupatiChintha RamuNo ratings yet
- Summary List of BeneficiariesDocument3 pagesSummary List of BeneficiariesMetal WeebNo ratings yet
- Form 3 - HPV Masterlistingv FormDocument1 pageForm 3 - HPV Masterlistingv Formeloisa mae malitaoNo ratings yet
- Namakkal District Co-Operative Milk Producers' Union Limited, Namakkal Application FormDocument16 pagesNamakkal District Co-Operative Milk Producers' Union Limited, Namakkal Application FormarulmuruguNo ratings yet
- Application Format 2019 MODocument1 pageApplication Format 2019 MOUtkarsh AnandNo ratings yet
- FEMALE HPV 9 14 Years OldDocument1 pageFEMALE HPV 9 14 Years OldMA CARLA DIANNE PARABA. ESPINOSANo ratings yet
- Discharge Planning TBDocument2 pagesDischarge Planning TBNurida LatipahNo ratings yet
- Namakkal Aavin - Recruitment - Application - Final. - CORRECTED PDFDocument18 pagesNamakkal Aavin - Recruitment - Application - Final. - CORRECTED PDFSreekumarNarayanNo ratings yet
- Immunization Form For Visiting StudentsDocument1 pageImmunization Form For Visiting StudentsAnonymous tS0WWCCNo ratings yet
- School Based Immunization: Recording Form 1: Masterlist of Grade 1 StudentsDocument10 pagesSchool Based Immunization: Recording Form 1: Masterlist of Grade 1 StudentsScholar WinterflameNo ratings yet
- Cif AfpDocument2 pagesCif Afpninzah wanzahNo ratings yet
- SBI 2019: Masterlisting Form For Kinder To Grade 7 LearnersDocument1 pageSBI 2019: Masterlisting Form For Kinder To Grade 7 LearnersJhun Bel PadrillanNo ratings yet
- PFIZER 5 17 All in 1 FormDocument3 pagesPFIZER 5 17 All in 1 Formrenz jNo ratings yet
- Enclosure 3 - SDO Pre Registration Form - LearnCon PH 2023 - 20230310Document2 pagesEnclosure 3 - SDO Pre Registration Form - LearnCon PH 2023 - 20230310Mari BsnNo ratings yet
- Directorate of Nursing Services: Data Collection Tool PhotoDocument6 pagesDirectorate of Nursing Services: Data Collection Tool PhotoArif IslamNo ratings yet
- Bloorview SchoolDocument10 pagesBloorview SchoolAbdul KarimNo ratings yet
- PediatricDocument4 pagesPediatricIrma Nur Rizka HanifahNo ratings yet
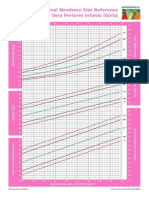
- Intergrowth21 Newborn Size Reference Charts (Girls)Document2 pagesIntergrowth21 Newborn Size Reference Charts (Girls)Anonymous MWd5UOUuiyNo ratings yet
- EwqrfDocument22 pagesEwqrfEmilio ApodacaNo ratings yet
- CVX CodesDocument16 pagesCVX CodesansarNo ratings yet
- For Vaccine Micro PlansDocument7 pagesFor Vaccine Micro PlansPrabir Kumar ChatterjeeNo ratings yet
- Vaccina1365tion FAQDocument2 pagesVaccina1365tion FAQAtharvaNo ratings yet
- Reaching Every Purok FormsDocument26 pagesReaching Every Purok FormsRich ArocenaNo ratings yet
- 0 18yrs Child Combined ScheduleDocument15 pages0 18yrs Child Combined ScheduleBONDADA GIRI SIVA NAGUNo ratings yet
- Vi Virgo Masterlist MeaslesDocument57 pagesVi Virgo Masterlist Measlesbess0910No ratings yet
- Pusponegoro HD. Standar Pelayanan Medis Kesehatan Anak Edisi 1. Jakarta: Badan Penerbit IDAI, 2004. Hal 149-153Document2 pagesPusponegoro HD. Standar Pelayanan Medis Kesehatan Anak Edisi 1. Jakarta: Badan Penerbit IDAI, 2004. Hal 149-153Nurrahmadani RambeNo ratings yet
- EPI To SendDocument13 pagesEPI To SendMarylle Joy SullanoNo ratings yet
- Pentingnya Pemberian Imunisasi DPT Pada Anak Difteri Dan PertusisDocument30 pagesPentingnya Pemberian Imunisasi DPT Pada Anak Difteri Dan Pertusisrevi rillianiNo ratings yet
- UKHSA 12155 Routine Childhood Immunisation Schedule - Feb2022Document1 pageUKHSA 12155 Routine Childhood Immunisation Schedule - Feb2022cicitNo ratings yet
- Vaccine - A Scientific Analysis (Malayalam) DR K P AravindanDocument3 pagesVaccine - A Scientific Analysis (Malayalam) DR K P AravindanMas ThulanNo ratings yet
- Routine Immunization Schedule For InfantsDocument2 pagesRoutine Immunization Schedule For InfantsknotstmNo ratings yet
- NICHQ Vanderbilt Assessment Scale-TEACHER-Informant PDFDocument3 pagesNICHQ Vanderbilt Assessment Scale-TEACHER-Informant PDFGloria oluchiNo ratings yet
- Laporan Vaksin Februari 2022Document32 pagesLaporan Vaksin Februari 2022Dewa Sigit SaPutraNo ratings yet
- Suspected Neonatal Sepsis: Tenth Clinical Consensus of The Ibero-American Society of Neonatology (SIBEN)Document32 pagesSuspected Neonatal Sepsis: Tenth Clinical Consensus of The Ibero-American Society of Neonatology (SIBEN)Anais SánchezNo ratings yet
- ImmunizationDocument1 pageImmunizationALYSSA DENISE CORPUZNo ratings yet
- Vaccination For NewbornsDocument5 pagesVaccination For NewbornsJannah Marie A. DimaporoNo ratings yet
- NID Report January 2013 Day 1 - 2 - 3Document10 pagesNID Report January 2013 Day 1 - 2 - 3Prabir Kumar ChatterjeeNo ratings yet
- BCG Hepatitisb Hexa1 Hexa2 Penta: Baby Immunization Schedule - QatarDocument3 pagesBCG Hepatitisb Hexa1 Hexa2 Penta: Baby Immunization Schedule - QatarKiran Kumar AkulaNo ratings yet
- Overview of Post Traumatic Stress Disorder (PTSD) Symptoms of Post-Road Traffic Accident PatientsDocument9 pagesOverview of Post Traumatic Stress Disorder (PTSD) Symptoms of Post-Road Traffic Accident PatientsAsniar RNo ratings yet