You might also like
- Nursing Study Guide: Your Nursing Assistant To Do Well In SchoolFrom EverandNursing Study Guide: Your Nursing Assistant To Do Well In SchoolRating: 3 out of 5 stars3/5 (2)
- Hospital Accreditation QuestionsDocument5 pagesHospital Accreditation Questionsshoumyaosu100% (21)
- Robotic Surgery Technical ManualDocument10 pagesRobotic Surgery Technical Manualapi-346387336No ratings yet
- Final Project Attrition & RetentionDocument91 pagesFinal Project Attrition & RetentionDilpreet KalerNo ratings yet
- Head Nursing Tool ChecklistDocument9 pagesHead Nursing Tool ChecklistManager HR Hijaz HospitalNo ratings yet
- J CNC 2014 10 007Document16 pagesJ CNC 2014 10 007martina.penatoNo ratings yet
- Luscombe 2010Document5 pagesLuscombe 2010Daniel Meyer CoraciniNo ratings yet
- Remifentanilo EleveldDocument14 pagesRemifentanilo EleveldAleNo ratings yet
- Evaluation of Three Paediatric Weight Estimation Methods in SingaporeDocument6 pagesEvaluation of Three Paediatric Weight Estimation Methods in SingaporeDewanggaWahyuPrajaNo ratings yet
- Reliability of Routine Anthropometric Measurements To Estimate Body Composition in Term InfantsDocument5 pagesReliability of Routine Anthropometric Measurements To Estimate Body Composition in Term InfantsLuana BarrosNo ratings yet
- Mac in Adult and ChildreanDocument6 pagesMac in Adult and ChildreanJorianditha RamadhanNo ratings yet
- The Apparent Breastfeeding Paradox in Very Preterm Infants: Relationship Between Breast Feeding, Early Weight Gain and Neurodevelopment Based On Results From Two Cohorts, EPIPAGE and LiftDocument9 pagesThe Apparent Breastfeeding Paradox in Very Preterm Infants: Relationship Between Breast Feeding, Early Weight Gain and Neurodevelopment Based On Results From Two Cohorts, EPIPAGE and LiftkurniawatiNo ratings yet
- Pacifier and Bottle Nipples: The Targets For Poor Breastfeeding OutcomesDocument3 pagesPacifier and Bottle Nipples: The Targets For Poor Breastfeeding Outcomesbeleg100% (1)
- Clinical Nutrition ESPEN: Original ArticleDocument6 pagesClinical Nutrition ESPEN: Original ArticleclaudyNo ratings yet
- Reliability of Breathing Rate Assessment and Chest Expansion MeasDocument6 pagesReliability of Breathing Rate Assessment and Chest Expansion MeasAnandhu GNo ratings yet
- Arenz Int J Obes 2004Document10 pagesArenz Int J Obes 2004Endank TaurinaNo ratings yet
- Lactancia MaternaDocument6 pagesLactancia MaternaFernandaNo ratings yet
- 2023 REYNOLDS Regulaçao Energia LactenteDocument9 pages2023 REYNOLDS Regulaçao Energia LactenteMélanie DíazNo ratings yet
- Preterm Infant Growth Velocity Calculations - A Systematic ReviewDocument12 pagesPreterm Infant Growth Velocity Calculations - A Systematic ReviewLeonardo CardozoNo ratings yet
- Interpreting Immunogenicity Data in UK Studies: Arch. Dis. ChildDocument9 pagesInterpreting Immunogenicity Data in UK Studies: Arch. Dis. ChildMargaretha MonikaNo ratings yet
- Contemporary Clinical Trials: SciencedirectDocument12 pagesContemporary Clinical Trials: SciencedirectJelisaaNo ratings yet
- Genetic Markers of Obesity Risk: Stronger Associations With Body Composition in Overweight Compared To Normal-Weight ChildrenDocument4 pagesGenetic Markers of Obesity Risk: Stronger Associations With Body Composition in Overweight Compared To Normal-Weight ChildrenLautaro AndradeNo ratings yet
- Espghan 2015 - Abstracts JPGN FinalDocument963 pagesEspghan 2015 - Abstracts JPGN FinalAdriana RockerNo ratings yet
- Mid-Arm Circumference Can Be Used To Estimate Weight of Adult and Adolescent PatientsDocument6 pagesMid-Arm Circumference Can Be Used To Estimate Weight of Adult and Adolescent PatientsQhialdy SusetyoNo ratings yet
- Comparison of The Accuracy of Clinical Methods For Estimation of Fetal WeightDocument7 pagesComparison of The Accuracy of Clinical Methods For Estimation of Fetal WeightArdika PutraNo ratings yet
- Mid-Arm Circumference Can Be Used To Estimate Weight of Adult and Adolescent PatientsDocument6 pagesMid-Arm Circumference Can Be Used To Estimate Weight of Adult and Adolescent PatientsLoreNo ratings yet
- Pediatric JournalDocument9 pagesPediatric JournalSatrianiNo ratings yet
- Curva Nutricional de Prematuros Basasos en Indice de Masa CorporalDocument12 pagesCurva Nutricional de Prematuros Basasos en Indice de Masa CorporalWilliam Arellano SantillanNo ratings yet
- NIH Public AccessDocument13 pagesNIH Public AccessmedrihanNo ratings yet
- Weighing TestDocument3 pagesWeighing TestImmawantiNo ratings yet
- Clinical Nutrition: Kristie L. Bell, Roslyn N. Boyd, Jacqueline L. Walker, Richard D. Stevenson, Peter S.W. DaviesDocument6 pagesClinical Nutrition: Kristie L. Bell, Roslyn N. Boyd, Jacqueline L. Walker, Richard D. Stevenson, Peter S.W. DaviesJorgeAdalbertoCabralPerezNo ratings yet
- Estimated Fetal Weight: Comparison of Clinical Versus Ultrasound EstimateDocument6 pagesEstimated Fetal Weight: Comparison of Clinical Versus Ultrasound EstimateNadia AyuningtiasNo ratings yet
- Caloric Intake Data AccuracyDocument6 pagesCaloric Intake Data AccuracylyleNo ratings yet
- Nutritional Neuroscience and Education5Document14 pagesNutritional Neuroscience and Education5Ingrid DíazNo ratings yet
- 10.1542@Peds.2012-0764.PDF Junal Nutrition 1Document9 pages10.1542@Peds.2012-0764.PDF Junal Nutrition 1bobkevinNo ratings yet
- 2016 Weight Change Nomograms For First Month PediatricsDocument9 pages2016 Weight Change Nomograms For First Month PediatricsMarco GunawanNo ratings yet
- Farmacocinética Propofol PDFDocument9 pagesFarmacocinética Propofol PDFFrancisco Ferrer TorresNo ratings yet
- Newborn ModuleDocument13 pagesNewborn Modulekrf8qbqmmfNo ratings yet
- Standardization of Early Feeding Skills (EFS) Scale in Preterm InfantsDocument7 pagesStandardization of Early Feeding Skills (EFS) Scale in Preterm InfantsMárcia FernandesNo ratings yet
- The Timing of Initiating Complementary Feeding in Preterm Infants and Its Effect On Overweight: A Systematic ReviewDocument9 pagesThe Timing of Initiating Complementary Feeding in Preterm Infants and Its Effect On Overweight: A Systematic ReviewDaniel PuertasNo ratings yet
- Baby Carrying Method Impacts Caregiver Postural.2Document7 pagesBaby Carrying Method Impacts Caregiver Postural.2Cata Gomez UbillaNo ratings yet
- NICUDocument11 pagesNICUCleoanne GallegosNo ratings yet
- Jurnal 3Document6 pagesJurnal 3Zaimatul HamdiyahNo ratings yet
- Influence of Obesity On Foot Loading Characteristics in Gait For Children Aged 1 To 12 YearsDocument12 pagesInfluence of Obesity On Foot Loading Characteristics in Gait For Children Aged 1 To 12 Yearstania martinezNo ratings yet
- Comparative-Study-Of-Four-Methods-Of-Clinical-Estimation-Of-Fetal-Weight 2Document9 pagesComparative-Study-Of-Four-Methods-Of-Clinical-Estimation-Of-Fetal-Weight 2Abegail Fermanejo-GeneraoNo ratings yet
- PYMS TamizajeDocument6 pagesPYMS TamizajeKevinGallagherNo ratings yet
- Wil Born 2018Document17 pagesWil Born 2018Clara RodriguesNo ratings yet
- Early Life Risk Factors For ObesityDocument13 pagesEarly Life Risk Factors For Obesitybarragan-prosisaNo ratings yet
- Maternal Diet, BreastfeedingDocument6 pagesMaternal Diet, BreastfeedingRiska Diene PratiwiNo ratings yet
- A Systematic Review of Practice Surveys On Parenteral Nutrition For Preterm InfantsDocument5 pagesA Systematic Review of Practice Surveys On Parenteral Nutrition For Preterm InfantsKhor Chin PooNo ratings yet
- Early Human Development: Madalynn Neu, Nicholas A. Hazel, Joann Robinson, Sarah J. Schmiege, Mark LaudenslagerDocument7 pagesEarly Human Development: Madalynn Neu, Nicholas A. Hazel, Joann Robinson, Sarah J. Schmiege, Mark LaudenslageryuliaNo ratings yet
- Pfister S Reflujo GastroDocument6 pagesPfister S Reflujo GastroAriadna de la GarzaNo ratings yet
- Duration of Breastfeeding and Developmental Milestones During The Latter Half of InfancyDocument6 pagesDuration of Breastfeeding and Developmental Milestones During The Latter Half of InfancyErwin SetiawanNo ratings yet
- Breastfeeding and The Use of Human Milk: An Analysis of The American Academy of Pediatrics 2012 Breastfeeding Policy StatementDocument2 pagesBreastfeeding and The Use of Human Milk: An Analysis of The American Academy of Pediatrics 2012 Breastfeeding Policy StatementBayna Lestari LubisNo ratings yet
- 1233 FullDocument4 pages1233 FullMarielos Livengood de SanabriaNo ratings yet
- Alchemical Complete Proteinligand Presenting No Cost Efforts With Regard To Medication Design and StyleufwbbDocument1 pageAlchemical Complete Proteinligand Presenting No Cost Efforts With Regard To Medication Design and Styleufwbbdugoutsquid65No ratings yet
- Antidepressants in Breast Milk Comparative Analysis of Excretion RatiosDocument8 pagesAntidepressants in Breast Milk Comparative Analysis of Excretion RatiosRubiNo ratings yet
- Prevalence of Overweight and Obesity in Irish Ambulant Children With Cerebral PalsyDocument7 pagesPrevalence of Overweight and Obesity in Irish Ambulant Children With Cerebral PalsymiNo ratings yet
- Artikel EBF & CFDocument7 pagesArtikel EBF & CFdayana nopridaNo ratings yet
- 18381-Article Text-59445-1-10-20171011Document6 pages18381-Article Text-59445-1-10-20171011maxmaxNo ratings yet
- Asesment of Growth and Nutrition in Children With Cerebral PalsyDocument4 pagesAsesment of Growth and Nutrition in Children With Cerebral Palsypratiwi dinia sariNo ratings yet
- BBLR 2Document6 pagesBBLR 2refiNo ratings yet
- Weight Gain After Adenotonsillectomy: A Case Control StudyDocument6 pagesWeight Gain After Adenotonsillectomy: A Case Control StudyMuhammad Aamir RizwanNo ratings yet
- Introduction To Social Work An Advocacy Based Profession Social Work in The New Century 2nd Edition Ebook PDFDocument62 pagesIntroduction To Social Work An Advocacy Based Profession Social Work in The New Century 2nd Edition Ebook PDFmary.krueger918100% (44)
- Geria - CT 7Document2 pagesGeria - CT 7Leighanne Clyve FerrerNo ratings yet
- Pamet Code of EthicsDocument2 pagesPamet Code of EthicsDiana LiNo ratings yet
- Conceptual Model of HRQoLDocument7 pagesConceptual Model of HRQoLNursyafiq Ali ShibramulisiNo ratings yet
- NCP JaundiceDocument3 pagesNCP JaundiceCamille Joy BaliliNo ratings yet
- Resume - Geraldine Wright 2013dec01norefsDocument2 pagesResume - Geraldine Wright 2013dec01norefsapi-242134202No ratings yet
- Diver Medical - Physician S Evaluation FormDocument1 pageDiver Medical - Physician S Evaluation Formcrispin quadrosNo ratings yet
- Annex I National Leprosy Eradication ProgrammeDocument5 pagesAnnex I National Leprosy Eradication ProgrammespmdocNo ratings yet
- Daniel's ResumeDocument2 pagesDaniel's ResumeDtron99No ratings yet
- Use of A Modified Matrix Band Technique To Restore Subgingival Root CariesDocument6 pagesUse of A Modified Matrix Band Technique To Restore Subgingival Root CariesDina NovaniaNo ratings yet
- NCP Ortho TanakaDocument4 pagesNCP Ortho TanakaJopaii TanakaNo ratings yet
- PHIN LectureDocument13 pagesPHIN Lecturedanilotinio2No ratings yet
- Opioid Whistleblower Amended ComplaintDocument118 pagesOpioid Whistleblower Amended ComplaintMitchell BlackNo ratings yet
- Voluntary AdmissionDocument1 pageVoluntary Admissionapi-414703292No ratings yet
- Is The Smile Line A Valid Parameter For Esthetic Evaluation A Systematic Literature ReviewDocument14 pagesIs The Smile Line A Valid Parameter For Esthetic Evaluation A Systematic Literature Reviewmaroun ghalebNo ratings yet
- Value Proposition Apollo HospitalsDocument2 pagesValue Proposition Apollo Hospitalsakashkr619No ratings yet
- Shadowing Journal 1Document3 pagesShadowing Journal 1api-542121618No ratings yet
- Management of Karnasrava - A Case ReportDocument3 pagesManagement of Karnasrava - A Case ReportEditor IJTSRDNo ratings yet
- IA Grp06Document21 pagesIA Grp06Sanjana SambanaNo ratings yet
- A Comparison of Four Caries Risk Assessment MethodsDocument13 pagesA Comparison of Four Caries Risk Assessment Methodsovy primaNo ratings yet
- Chapter 1 Pharmacology Complete Notes PDF D.Pharma ER20 PCI Noteskarts Pharmacology Notes PDFDocument16 pagesChapter 1 Pharmacology Complete Notes PDF D.Pharma ER20 PCI Noteskarts Pharmacology Notes PDFNagur123 ShaikNo ratings yet
- Nystatin OralDocument3 pagesNystatin OralRangga Prabu PradanaNo ratings yet
- Contributions of Ibn Zuhr (Avenzoar) To The Progress of Medicine and UrologyDocument7 pagesContributions of Ibn Zuhr (Avenzoar) To The Progress of Medicine and UrologyRabie E. Abdel-HalimNo ratings yet
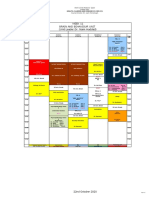
- Week 11 Brain and Behaviour Unit (Unit Leader:Dr. Naim Haddad)Document1 pageWeek 11 Brain and Behaviour Unit (Unit Leader:Dr. Naim Haddad)f3er3No ratings yet
- Early Warning ScoresDocument14 pagesEarly Warning ScoresmuchtarNo ratings yet
- 1344257272WebFinal - County Seat - July 2012 28 PagesDocument28 pages1344257272WebFinal - County Seat - July 2012 28 PagesCoolerAdsNo ratings yet