You might also like
- PainDocument35 pagesPainixora n100% (1)
- Measuring Health A Review of Quality of Life Measurement ScalesDocument227 pagesMeasuring Health A Review of Quality of Life Measurement ScalessharethefilesNo ratings yet
- Community Health Nursing - REVIEWERDocument45 pagesCommunity Health Nursing - REVIEWERmary navalNo ratings yet
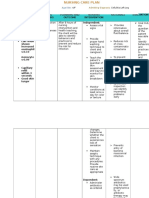
- NCP Cellulitis Risk For InfectionDocument3 pagesNCP Cellulitis Risk For Infectionchin ramos50% (2)
- Family Case StudyDocument24 pagesFamily Case StudyJulius BravoNo ratings yet
- Pterygium Major Care Plan 3CP SheetsDocument3 pagesPterygium Major Care Plan 3CP SheetsJoy100% (5)
- FDS Amp 2020Document140 pagesFDS Amp 2020Shahrukh ali khan100% (1)
- Prescription - 540660 - 12 11 2020 - Dr. Bikash Majumder - Apollo 247Document2 pagesPrescription - 540660 - 12 11 2020 - Dr. Bikash Majumder - Apollo 247soumitra choudhuryNo ratings yet
- MS 2 NCP Deep Vein ThrombosisDocument4 pagesMS 2 NCP Deep Vein ThrombosisRosaree Mae PantojaNo ratings yet
- Comparative-Study-Of-Four-Methods-Of-Clinical-Estimation-Of-Fetal-Weight 2Document9 pagesComparative-Study-Of-Four-Methods-Of-Clinical-Estimation-Of-Fetal-Weight 2Abegail Fermanejo-GeneraoNo ratings yet
- Jog 12115Document7 pagesJog 12115niko4eyesNo ratings yet
- Obesity and PregnancyDocument6 pagesObesity and PregnancyBudiarto BaskoroNo ratings yet
- 33219-Article Text-97197-1-10-20201204Document6 pages33219-Article Text-97197-1-10-20201204ZisuhNo ratings yet
- Protocol - PaedsDocument3 pagesProtocol - PaedsShradha PrakashNo ratings yet
- A Comparison Between Palpation Method and Johnsons Rule To Estimate Fetal WeightDocument8 pagesA Comparison Between Palpation Method and Johnsons Rule To Estimate Fetal WeightbamcobgyneNo ratings yet
- Proforma Synopsis For Registration of SubjectDocument15 pagesProforma Synopsis For Registration of SubjectTamilArasiNo ratings yet
- Comparison Between Three Methods of Fetal Weight Estimation During The Active Stage of Labor Performed by Residents: A Prospective Cohort StudyDocument7 pagesComparison Between Three Methods of Fetal Weight Estimation During The Active Stage of Labor Performed by Residents: A Prospective Cohort StudyMahida El shafiNo ratings yet
- Estimated Fetal Weight: Comparison of Clinical Versus Ultrasound EstimateDocument6 pagesEstimated Fetal Weight: Comparison of Clinical Versus Ultrasound EstimateNadia AyuningtiasNo ratings yet
- Oligohydramnion PDFDocument6 pagesOligohydramnion PDFhusain abdul halimNo ratings yet
- Article in Press: Effects of Central Obesity On Maternal Complications in Korean Women of Reproductive AgeDocument8 pagesArticle in Press: Effects of Central Obesity On Maternal Complications in Korean Women of Reproductive AgeMhmmd FasyaNo ratings yet
- Eclinicalmedicine: Berit Mortensen, Marit Lieng, Lien My Diep, Mirjam Lukasse, Kefaya Atieh, Erik FosseDocument8 pagesEclinicalmedicine: Berit Mortensen, Marit Lieng, Lien My Diep, Mirjam Lukasse, Kefaya Atieh, Erik FosseNur fajrina TamimiNo ratings yet
- Predictors of Induction of Labor and Success Rate Among MothersDocument9 pagesPredictors of Induction of Labor and Success Rate Among MothersAdmasu BelayNo ratings yet
- Reliability of Routine Anthropometric Measurements To Estimate Body Composition in Term InfantsDocument5 pagesReliability of Routine Anthropometric Measurements To Estimate Body Composition in Term InfantsLuana BarrosNo ratings yet
- Exercise in Pregnant Women and Birth WeightDocument4 pagesExercise in Pregnant Women and Birth WeightJelita SihombingNo ratings yet
- Pregnancy Exercise Overweight MetaanalysisDocument11 pagesPregnancy Exercise Overweight MetaanalysisAisleenHNo ratings yet
- Evaluation of Some Anthropometric IndicesDocument7 pagesEvaluation of Some Anthropometric IndicesMuhammad Al-TohamyNo ratings yet
- 2012 Article 61Document5 pages2012 Article 61Al MubartaNo ratings yet
- ijwh-5-501Document7 pagesijwh-5-501MarianaafiatiNo ratings yet
- Maternal BMI's impact on pre-eclampsia phenotypeDocument7 pagesMaternal BMI's impact on pre-eclampsia phenotypeAchmad Deza FaristaNo ratings yet
- Short Stature Is Associated With An Increased Risk of Caesarean Deliveries in Low Risk PopulationDocument6 pagesShort Stature Is Associated With An Increased Risk of Caesarean Deliveries in Low Risk PopulationManangioma ManNo ratings yet
- InformaciónDocument6 pagesInformaciónVIOLETA JACKELINE ARMAS CHAVEZNo ratings yet
- Hyperemesis Gravidarum and Its Relation With Maternal Body Fat CompositionDocument6 pagesHyperemesis Gravidarum and Its Relation With Maternal Body Fat CompositionEver Medina UnchupaicoNo ratings yet
- Evaluation of World Health Organization Par To Graph Implementation by Midwives For Maternity Home Birth in MedanDocument17 pagesEvaluation of World Health Organization Par To Graph Implementation by Midwives For Maternity Home Birth in MedanInnocentia Nonhlanhla MtoloNo ratings yet
- ResearchDocument20 pagesResearchtedypsNo ratings yet
- 10 1111@jog 143436777777Document17 pages10 1111@jog 143436777777Epiphany SonderNo ratings yet
- Breast Self-Examination: Knowledge and Practice Among Nurses in United Arab EmiratesDocument4 pagesBreast Self-Examination: Knowledge and Practice Among Nurses in United Arab EmiratesDemiar Madlansacay QuintoNo ratings yet
- Impact of Oligohydramnios On Maternal and PerinataDocument6 pagesImpact of Oligohydramnios On Maternal and PerinataDiana SchlittlerNo ratings yet
- Bakker 2012Document10 pagesBakker 2012ieoNo ratings yet
- V11n3oa04 PDFDocument6 pagesV11n3oa04 PDFGohar Ali UsmanNo ratings yet
- The Effect of Obesity On Pregnancy and Its Outcome in The Population of Oman, Seeb ProvinceDocument12 pagesThe Effect of Obesity On Pregnancy and Its Outcome in The Population of Oman, Seeb ProvinceHazley ZeeNo ratings yet
- D'Souza-2019-Maternal Body Mass Index and PregDocument17 pagesD'Souza-2019-Maternal Body Mass Index and PregMARIATUL QIFTIYAHNo ratings yet
- Third Trimester Ultrasound Scan Combined With A Clinical Method For Accurate Birthweight Prediction at Term: A Cohort Study in SpainDocument12 pagesThird Trimester Ultrasound Scan Combined With A Clinical Method For Accurate Birthweight Prediction at Term: A Cohort Study in SpainRegina PizanNo ratings yet
- Role of Gastric Lavage in Newborn With Meconium Stained Amniotic Fluid:a Randomized Controlled TrailDocument3 pagesRole of Gastric Lavage in Newborn With Meconium Stained Amniotic Fluid:a Randomized Controlled TrailtriaanggareniNo ratings yet
- Partus LamaDocument8 pagesPartus LamaSulis SipinNo ratings yet
- Vegetarian Diet Safety During Pregnancy Meta-AnalysisDocument41 pagesVegetarian Diet Safety During Pregnancy Meta-AnalysisyuliaNo ratings yet
- G0632933 PDFDocument5 pagesG0632933 PDFIta ChawNo ratings yet
- Safety of Acupuncture During Pregnancy: A Retrospective Cohort Study in KoreaDocument8 pagesSafety of Acupuncture During Pregnancy: A Retrospective Cohort Study in Koreaindra coolNo ratings yet
- rtcog,+Journal+manager,+Korranat+Thanaratsiriworakul Vol.24 No.3 pp.161-168Document8 pagesrtcog,+Journal+manager,+Korranat+Thanaratsiriworakul Vol.24 No.3 pp.161-168Waode RadmilaNo ratings yet
- Validity of Hysteroscopy in Detection of Uterine Cavity Abnormalities in Women With Recurrent Pregnancy LossDocument5 pagesValidity of Hysteroscopy in Detection of Uterine Cavity Abnormalities in Women With Recurrent Pregnancy LossPeertechz Publications Inc.No ratings yet
- Cervical Stitch (Cerclage) For Preventing Pregnancy Loss: Individual Patient Data Meta-AnalysisDocument17 pagesCervical Stitch (Cerclage) For Preventing Pregnancy Loss: Individual Patient Data Meta-AnalysisNi Wayan Ana PsNo ratings yet
- Shahad 7Document10 pagesShahad 7Mohammed OmarNo ratings yet
- Zhao2015 PDFDocument9 pagesZhao2015 PDFmavarthavaNo ratings yet
- Knee Chest Position To Reduce The Incidence of Breech PresentationDocument5 pagesKnee Chest Position To Reduce The Incidence of Breech PresentationNoviaNo ratings yet
- Risk Factors and Long-Term Health Consequences of MacrosomiaDocument6 pagesRisk Factors and Long-Term Health Consequences of MacrosomiaKhuriyatun NadhifahNo ratings yet
- 2019 Article 505Document12 pages2019 Article 505Xiomara Alfaro AraujoNo ratings yet
- Maternal and Fetal Outcomes of Obese Pregnant Women: A Prospective Cohort StudyDocument5 pagesMaternal and Fetal Outcomes of Obese Pregnant Women: A Prospective Cohort StudyCostin VrabieNo ratings yet
- Guidelines On 8 Key Evidence Based Practices During Labour - 353Document35 pagesGuidelines On 8 Key Evidence Based Practices During Labour - 353National Child Health Resource Centre (NCHRC)No ratings yet
- 08 AimukhametovaDocument10 pages08 AimukhametovahendraNo ratings yet
- The World Health Organization Fetal Growth ChartsDocument36 pagesThe World Health Organization Fetal Growth ChartsAndri SistikaNo ratings yet
- BMJ f6398Document13 pagesBMJ f6398Luis Gerardo Pérez CastroNo ratings yet
- Jurnal CrossectionalDocument9 pagesJurnal CrossectionalRheaNo ratings yet
- International Journal of Health Sciences and Research: Fetal Umbilical Cord Circumference Measurement and Birth WeightDocument6 pagesInternational Journal of Health Sciences and Research: Fetal Umbilical Cord Circumference Measurement and Birth WeightFatma ElzaytNo ratings yet
- Population Based Study of EpisiotomyDocument6 pagesPopulation Based Study of EpisiotomyMeriton Stanly ANo ratings yet
- 26 Device Improves Swallowing in Newborns: CommentDocument33 pages26 Device Improves Swallowing in Newborns: CommentWahyuni M. Ali MreNo ratings yet
- Maternal and Perinatal Maternal and Perinatal Outcome of Maternal Obesity Outcome of Maternal Obesity at RSCM in 2014-2019 at RSCM in 2014-2019Document1 pageMaternal and Perinatal Maternal and Perinatal Outcome of Maternal Obesity Outcome of Maternal Obesity at RSCM in 2014-2019 at RSCM in 2014-2019heidi leeNo ratings yet
- Gestational Age Assessment - StatPearls - NCBI BookshelfDocument8 pagesGestational Age Assessment - StatPearls - NCBI BookshelfFantya Cerebella AslamyNo ratings yet
- GUias de Practica Clinica de Ecografias de 2do TrimestreDocument11 pagesGUias de Practica Clinica de Ecografias de 2do TrimestreRodrigo BenitezNo ratings yet
- The Interactive Effect of Prepregnancy Overweight/Obesity and Isolated Maternal Hypothyroxinemia On MacrosomiaDocument8 pagesThe Interactive Effect of Prepregnancy Overweight/Obesity and Isolated Maternal Hypothyroxinemia On MacrosomiaAndres GallegosNo ratings yet
- 345 668 1 SMDocument5 pages345 668 1 SMAgya Nanda PrasetyaNo ratings yet
- Penatalaksanaan Glaukoma Fakomorfik - Lucky FitradaDocument10 pagesPenatalaksanaan Glaukoma Fakomorfik - Lucky FitradaArdika PutraNo ratings yet
- Who HerpesDocument56 pagesWho HerpesYanna RizkiaNo ratings yet
- PENCEGAHANREAKTIVASIDocument6 pagesPENCEGAHANREAKTIVASIDio AnandaNo ratings yet
- Correlation Between Diabetes Autoantibodies and Environmental Parameters inDocument8 pagesCorrelation Between Diabetes Autoantibodies and Environmental Parameters inArdika PutraNo ratings yet
- Nutrition and The Elderly: DR Putra Hendra SPPD UnibaDocument35 pagesNutrition and The Elderly: DR Putra Hendra SPPD UnibaArdika PutraNo ratings yet
- Health Education and Health Promotion Skills of Health Care Professionals Working in Family Health CentresDocument7 pagesHealth Education and Health Promotion Skills of Health Care Professionals Working in Family Health CentresArdika PutraNo ratings yet
- Effect of Socio-Demographic and Clinical Characteristics On Physical Activity of Pregnant Women at Referral Hospital in Riyadh, KSADocument7 pagesEffect of Socio-Demographic and Clinical Characteristics On Physical Activity of Pregnant Women at Referral Hospital in Riyadh, KSAArdika PutraNo ratings yet
- Effect of Water Pollution On Blood Elements in The Human Population of Hail, KSADocument6 pagesEffect of Water Pollution On Blood Elements in The Human Population of Hail, KSAArdika PutraNo ratings yet
- T MR MediastinumDocument19 pagesT MR MediastinumArdika PutraNo ratings yet
- Perilaku Sarapan Pagi Anak Sekolah Dasar: Program Pascasarjana Kesehatan Masyarakat Stikes Mitra LampungDocument9 pagesPerilaku Sarapan Pagi Anak Sekolah Dasar: Program Pascasarjana Kesehatan Masyarakat Stikes Mitra LampungArdika PutraNo ratings yet
- Nursing Care PlanDocument6 pagesNursing Care PlanJohann OrtizNo ratings yet
- Parcare Assessment MaxillofacialDocument22 pagesParcare Assessment Maxillofacialqta omerNo ratings yet
- Nutritionist and DietitiansDocument8 pagesNutritionist and DietitiansJoan Morta EdquilaNo ratings yet
- B30 Patient Monitor: GE HealthcareDocument6 pagesB30 Patient Monitor: GE HealthcareFrancisco MartinezNo ratings yet
- Appendix 1 Guideline Evaluation Anticancer Medicinal Products Man Methodological Consideration Using enDocument8 pagesAppendix 1 Guideline Evaluation Anticancer Medicinal Products Man Methodological Consideration Using enpir purwokertoNo ratings yet
- Journal Reading Pneumoni Aspirasi - Kelompok 8Document21 pagesJournal Reading Pneumoni Aspirasi - Kelompok 8Rifly PradanaNo ratings yet
- School Mental Health Accomplishment Report 2021 - : DivisionDocument8 pagesSchool Mental Health Accomplishment Report 2021 - : DivisionCriselda DuatinNo ratings yet
- Björngren Cuadra, Carin Und Sandro Cattacin (HG.) (2007) - Migration and Health. Difference Sensitivity From An Organisational Perspective. Malmö: IMER.Document148 pagesBjörngren Cuadra, Carin Und Sandro Cattacin (HG.) (2007) - Migration and Health. Difference Sensitivity From An Organisational Perspective. Malmö: IMER.sandro.cattacin6471No ratings yet
- Kelsey Nash ResumeDocument2 pagesKelsey Nash Resumeapi-349578979No ratings yet
- Communication Barrier Between Nurse and Patient at The Hospital: A Systematic ReviewDocument6 pagesCommunication Barrier Between Nurse and Patient at The Hospital: A Systematic ReviewSilvister MendonsaNo ratings yet
- Drug Development: Basic: Phase I-III: Overview of Clinical TrialsDocument71 pagesDrug Development: Basic: Phase I-III: Overview of Clinical TrialsKomal KhanNo ratings yet
- Bramley 2000Document5 pagesBramley 2000Andres SalcedoNo ratings yet
- Jadwal Pit (Fetomaternal Room)Document3 pagesJadwal Pit (Fetomaternal Room)Dwi Adi NugrohoNo ratings yet
- DFCR NY Sign-On Letter FINALDocument6 pagesDFCR NY Sign-On Letter FINALNick ReismanNo ratings yet
- Adverse Childhood Experiences and Adult Health: Vincent J. Felitti, MDDocument3 pagesAdverse Childhood Experiences and Adult Health: Vincent J. Felitti, MDAndreea PalNo ratings yet
- 436 - ResumeDocument2 pages436 - Resumeapi-520858833No ratings yet
- ETHICO OutlineDocument5 pagesETHICO Outline'emotera' Gudbai DotaNo ratings yet
- ProgrammeDocument4 pagesProgrammeapi-240583264No ratings yet
- Aquino 2018Document64 pagesAquino 2018Annisaa FitriNo ratings yet
- Philippines' Community Health Network SystemDocument2 pagesPhilippines' Community Health Network SystemQueenie BacolodNo ratings yet
- HEADS-ED EnglishDocument1 pageHEADS-ED EnglishmarselyagNo ratings yet