0% found this document useful (0 votes)
50 views1 pageCellulitis Management Guidelines for Adults
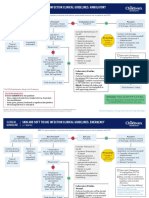
This document provides guidance on the management of cellulitis in adults. It outlines the diagnosis, assessment of severity, investigations and treatment options for cellulitis depending on severity. Treatment involves antibiotics such as flucloxacillin, doxycycline or clindamycin. For more severe cases such as sepsis or necrotizing fasciitis, IV antibiotics and surgical review are recommended. Oral antibiotics may be used once symptoms are improving and markers decreasing.
Uploaded by
Intan Mega PratidianaCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd
0% found this document useful (0 votes)
50 views1 pageCellulitis Management Guidelines for Adults
This document provides guidance on the management of cellulitis in adults. It outlines the diagnosis, assessment of severity, investigations and treatment options for cellulitis depending on severity. Treatment involves antibiotics such as flucloxacillin, doxycycline or clindamycin. For more severe cases such as sepsis or necrotizing fasciitis, IV antibiotics and surgical review are recommended. Oral antibiotics may be used once symptoms are improving and markers decreasing.
Uploaded by
Intan Mega PratidianaCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd