You might also like
- Adult Infectious Disease Bulletpoints HandbookFrom EverandAdult Infectious Disease Bulletpoints HandbookRating: 4.5 out of 5 stars4.5/5 (9)
- Antibiotic Surgical Prophylaxis Protocol SMH October 2018 UpdateDocument7 pagesAntibiotic Surgical Prophylaxis Protocol SMH October 2018 Updatessrnew2023No ratings yet
- Antimicrobial Therapy in Veterinary MedicineFrom EverandAntimicrobial Therapy in Veterinary MedicineSteeve GiguèreRating: 4 out of 5 stars4/5 (1)
- CNS: Ent:: Review Antibiotic Therapy Daily - Can You: Stop? Switch? Simplify? or State Duration?Document1 pageCNS: Ent:: Review Antibiotic Therapy Daily - Can You: Stop? Switch? Simplify? or State Duration?Fitri RachmadaniNo ratings yet
- Antibiotic hospital manDocument1 pageAntibiotic hospital manarshiya.manasekiNo ratings yet
- Icu Antibiotic GuidelinesDocument4 pagesIcu Antibiotic GuidelinesTia MonitaNo ratings yet
- Protcolo NacDocument2 pagesProtcolo NacJdmp Lopez MorenoNo ratings yet
- Sepsis and Catheter Infections: Early Conversion From IV To Oral AntibioticsDocument4 pagesSepsis and Catheter Infections: Early Conversion From IV To Oral AntibioticsChaim HerreraNo ratings yet
- Central Nervous System InfectionsDocument9 pagesCentral Nervous System InfectionsSaddamNo ratings yet
- IDSA - ATS 2016 Guideline for HAP and VAPDocument1 pageIDSA - ATS 2016 Guideline for HAP and VAPMariana MarpaungNo ratings yet
- Paclitaxel With Dose Dense EC Adjuvant or Neo-Adjuvant Protocol V1.0Document7 pagesPaclitaxel With Dose Dense EC Adjuvant or Neo-Adjuvant Protocol V1.0smokkerNo ratings yet
- Empiric Antibiotic ListDocument2 pagesEmpiric Antibiotic ListpasswordNo ratings yet
- NAG Upper Respiratory Tract InfectionsDocument20 pagesNAG Upper Respiratory Tract InfectionsJun JimenezNo ratings yet
- Adult Sepsis Order SetDocument3 pagesAdult Sepsis Order SetYoussef MokdadNo ratings yet
- Sepsis Antibiotics 2019 PDFDocument3 pagesSepsis Antibiotics 2019 PDFKobra CaktusNo ratings yet
- Treatment of MalariaDocument49 pagesTreatment of MalariaShanza AmaanNo ratings yet
- TREATING OBSTETRIC/GYNECOLOGIC INFECTIONSDocument3 pagesTREATING OBSTETRIC/GYNECOLOGIC INFECTIONSHarshit RastogiNo ratings yet
- Paclitaxel With EC Adjuvant or Neoadjuvant Protocol V1.1Document7 pagesPaclitaxel With EC Adjuvant or Neoadjuvant Protocol V1.1smokkerNo ratings yet
- Paclitaxel Trastuzumab Breast Cancer ProtocolDocument9 pagesPaclitaxel Trastuzumab Breast Cancer ProtocolsmokkerNo ratings yet
- 2012 Aug IMG Poster 165760a SepsisDocument1 page2012 Aug IMG Poster 165760a SepsisTeng Huei LeeNo ratings yet
- SQC ABx Guidelines 2-21-2011 PDFDocument2 pagesSQC ABx Guidelines 2-21-2011 PDFMinh SteveNo ratings yet
- Guidelines For First-Line Empirical Antibiotic Therapy in AdultsDocument1 pageGuidelines For First-Line Empirical Antibiotic Therapy in AdultsAnonymous s4yarxNo ratings yet
- Internal-Abdominal-infection-Treatment-ProtocolDocument9 pagesInternal-Abdominal-infection-Treatment-Protocolhatem newishyNo ratings yet
- Severe Sepsis and Septic Shock Antibiotic Guide: Community AcquiredDocument6 pagesSevere Sepsis and Septic Shock Antibiotic Guide: Community AcquiredAnonymous G6zDTD2yNo ratings yet
- Pneumonia Treatment Algorithm With Addendum For Aspiration 2015-2016.01.19Document2 pagesPneumonia Treatment Algorithm With Addendum For Aspiration 2015-2016.01.19Irsalina TriastutikNo ratings yet
- BTUH Antibiotics Pocket Guidelines For Prescribing in Adults 2017 2018Document2 pagesBTUH Antibiotics Pocket Guidelines For Prescribing in Adults 2017 2018Corry ApriliaNo ratings yet
- Obstetrics / Gynaecological Infections: Indications First Line AlternateDocument2 pagesObstetrics / Gynaecological Infections: Indications First Line AlternateAli ShanNo ratings yet
- Medicine RotatationbookletDocument20 pagesMedicine RotatationbookletJanelle JosephsNo ratings yet
- SHC Antimicrobial Prophylaxis RecommendationsDocument3 pagesSHC Antimicrobial Prophylaxis RecommendationsCatherine MorrisNo ratings yet
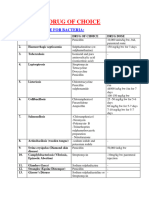
- Share Drugs of Choice To DiseasesDocument4 pagesShare Drugs of Choice To DiseasesDrkhanmianiNo ratings yet
- Febrile NeutropeniaDocument3 pagesFebrile Neutropeniatheseus5No ratings yet
- Fluconazole: ErthromycinDocument7 pagesFluconazole: ErthromycinAseel AlsheeshNo ratings yet
- Antibiotic Guidelines For PediatricsDocument33 pagesAntibiotic Guidelines For PediatricsVarshini Tamil SelvanNo ratings yet
- Antimicrobials - SPDocument27 pagesAntimicrobials - SPAmisha VastaniNo ratings yet
- Vancomycin & Vancomycin Resistant Enterococci: Abdullah M. Kharbosh, B.SC., PharmDocument78 pagesVancomycin & Vancomycin Resistant Enterococci: Abdullah M. Kharbosh, B.SC., Pharmkharbosham100% (1)
- Pocket Guide June2013 PDFDocument2 pagesPocket Guide June2013 PDFSergeyGruntov100% (1)
- NICU ABX ChartDocument11 pagesNICU ABX ChartdrchiNo ratings yet
- Cisplatin-Pemetrexed (NSCLC)Document5 pagesCisplatin-Pemetrexed (NSCLC)Sindu SankarNo ratings yet
- CAP Guidance 2020 Revision Final UpdatedDocument11 pagesCAP Guidance 2020 Revision Final UpdatedNeerajaNo ratings yet
- GDL 01240Document7 pagesGDL 01240Christian KosiNo ratings yet
- Antimicrobial Dosage Adjustments in Renal Impairment For FormularyDocument20 pagesAntimicrobial Dosage Adjustments in Renal Impairment For Formularyangkatanjuli2019No ratings yet
- Guidelines For Inpatient Management of PneumoniaDocument2 pagesGuidelines For Inpatient Management of PneumoniaHamza El-ȜfifiNo ratings yet
- NAG Central Nervous System Infections As of Nov 2017Document9 pagesNAG Central Nervous System Infections As of Nov 2017Rhod Bernaldez EstaNo ratings yet
- Management of CAP in Adults - Ontario GovernmentDocument2 pagesManagement of CAP in Adults - Ontario GovernmentSukhvir AujlaNo ratings yet
- AHS антибиотики рекомендацDocument42 pagesAHS антибиотики рекомендацMaksym DemianchukNo ratings yet
- Wound Infections: Common PathogensDocument1 pageWound Infections: Common PathogensAnonymous KGxzow5zxhNo ratings yet
- Paediatric Cardiac Surgical Antibiotic Prophylaxis: PurposeDocument9 pagesPaediatric Cardiac Surgical Antibiotic Prophylaxis: PurposeZamzam DomaNo ratings yet
- Antibiotic/Antiviral Policy - Paediatric PCF (EWMSCDocument9 pagesAntibiotic/Antiviral Policy - Paediatric PCF (EWMSCLizbet parrondoNo ratings yet
- Empiric Treatment Guidelines Common InfectionsDocument9 pagesEmpiric Treatment Guidelines Common InfectionsShiza Batool100% (1)
- Rapid Blood Pathogen Identification Panel: Staphylococcus Genus Analyte Will Be DetectedDocument8 pagesRapid Blood Pathogen Identification Panel: Staphylococcus Genus Analyte Will Be DetectedAlessia JankowskiNo ratings yet
- HSB Pneumonia Antibiotic AlgorithmDocument4 pagesHSB Pneumonia Antibiotic AlgorithmDr.Senthil KumarNo ratings yet
- Antibiotic PolicyDocument10 pagesAntibiotic Policykrutarth shahNo ratings yet
- Antibiotic ProphylaxisDocument2 pagesAntibiotic Prophylaxisabdelhamed aliNo ratings yet
- Day 1 Typhoid Fever_ItableDocument42 pagesDay 1 Typhoid Fever_ItableRye CalderonNo ratings yet
- Bone and Joint Infection Treatment GuidelinesDocument3 pagesBone and Joint Infection Treatment GuidelinesDanissa Fidia PuteriNo ratings yet
- SSTI and Skin Infection Treatment GuideDocument22 pagesSSTI and Skin Infection Treatment GuideAlexis TranNo ratings yet
- Ritemed Clindamycin HCL: Therapeutic CategoryDocument4 pagesRitemed Clindamycin HCL: Therapeutic CategoryJ Ohn P AulNo ratings yet
- Paclitaxel Carboplatin Protocol Gynae CancerDocument8 pagesPaclitaxel Carboplatin Protocol Gynae CancerHeryanti PusparisaNo ratings yet
- Antibiotic Guidelines for Skin and Soft Tissue InfectionsDocument11 pagesAntibiotic Guidelines for Skin and Soft Tissue InfectionslaptopgreyNo ratings yet
- NAG Skin and Soft Tissue Infections AdultsDocument21 pagesNAG Skin and Soft Tissue Infections AdultsJun JimenezNo ratings yet
- Post Graduate Academic Report Vion FinalDocument18 pagesPost Graduate Academic Report Vion FinalVishali RayapudiNo ratings yet
- nuRSING rEVIEWER PART 2Document9 pagesnuRSING rEVIEWER PART 2Johny VillanuevaNo ratings yet
- Surat Buat VisaDocument12 pagesSurat Buat VisaNurul FitrianaNo ratings yet
- In The High Court of Judicature at MadrasDocument17 pagesIn The High Court of Judicature at MadrasChinna Balanna NalamalaNo ratings yet
- Multiple Choice Question (MCQ) Exam: 15 Sample QuestionsDocument4 pagesMultiple Choice Question (MCQ) Exam: 15 Sample QuestionssheryNo ratings yet
- New PRC FormDocument6 pagesNew PRC Formduke1206No ratings yet
- MIT Technology Review 2020 11Document92 pagesMIT Technology Review 2020 11pppaolo100% (1)
- Code of Medical Ethics Chapter 8Document12 pagesCode of Medical Ethics Chapter 8api-324680787No ratings yet
- Improving Attitudes and Perceptions About End-of-Life Nursing On A Hospital-Based Palliative Care UnitDocument8 pagesImproving Attitudes and Perceptions About End-of-Life Nursing On A Hospital-Based Palliative Care UnitSERGIO ANDRES CESPEDES GUERRERONo ratings yet
- Sandra A. Mouloudj Recognized As A Professional of The Year by Strathmore's Who's Who Worldwide PublicationDocument2 pagesSandra A. Mouloudj Recognized As A Professional of The Year by Strathmore's Who's Who Worldwide PublicationPR.comNo ratings yet
- DOH Updates For PHA - May 6 Baguio PDFDocument49 pagesDOH Updates For PHA - May 6 Baguio PDFKaren BalanayNo ratings yet
- Living Donor Transplantation BrochureDocument13 pagesLiving Donor Transplantation BrochureShani KushwahaNo ratings yet
- Correspondence: The Fishmouth Phenomenon in Retinal DetachmentDocument1 pageCorrespondence: The Fishmouth Phenomenon in Retinal DetachmentSushi HtetNo ratings yet
- Children's Hospital Pain Clinic BrochureDocument2 pagesChildren's Hospital Pain Clinic BrochureM CurtissNo ratings yet
- The Gazette April 2013Document12 pagesThe Gazette April 2013St George's Healthcare NHS TrustNo ratings yet
- Draft Guidelines On Post Registration Variations To Registered Pharmaceutical and Biological Drug Products.Document35 pagesDraft Guidelines On Post Registration Variations To Registered Pharmaceutical and Biological Drug Products.vafaashkNo ratings yet
- Young Latina MS PatientDocument14 pagesYoung Latina MS PatientSnezana MihajlovicNo ratings yet
- Cannulation and Venepuncture WorkbookDocument58 pagesCannulation and Venepuncture WorkbookNorbertus Maceka83% (6)
- Ethics in Health CareDocument23 pagesEthics in Health CareShimmering MoonNo ratings yet
- LFD FormatDocument2 pagesLFD FormatKristine Angie RamosNo ratings yet
- Neurología NatalizumabDocument41 pagesNeurología Natalizumablorcy9No ratings yet
- Interview Questions-Ronak ShahDocument3 pagesInterview Questions-Ronak Shahapi-277297976No ratings yet
- Resume - Viroja Sweta For PortfolioDocument1 pageResume - Viroja Sweta For Portfolioapi-608195339No ratings yet
- Lesson 1.1: Historical Perspectives of Nursing InformaticsDocument33 pagesLesson 1.1: Historical Perspectives of Nursing InformaticsJustine Jean GuillermoNo ratings yet
- Long Resume and ApplicationDocument5 pagesLong Resume and ApplicationCarlo Domingo LadieroNo ratings yet
- 1 CBT Sample Questionnaires-1Document101 pages1 CBT Sample Questionnaires-1Mhee FaustinaNo ratings yet
- Essay On Academic BurnoutDocument1 pageEssay On Academic BurnoutrighteousindignationNo ratings yet
- Phs 801 Introduction To Public Health and Primary Health CareDocument107 pagesPhs 801 Introduction To Public Health and Primary Health CareEnobong UsoroNo ratings yet
- Post and Cores CaseDocument7 pagesPost and Cores Caseanuj sharmaNo ratings yet
- Clarion Technologies: at A GlanceDocument7 pagesClarion Technologies: at A GlanceChetan PrasadNo ratings yet