You might also like
- Differentiating Anesthesia Equipment: Identify and Understand Anesthesia Equipment in 1 Hour (Including the most popular manufacturers and suppliers to buy Anesthesia Equipment)From EverandDifferentiating Anesthesia Equipment: Identify and Understand Anesthesia Equipment in 1 Hour (Including the most popular manufacturers and suppliers to buy Anesthesia Equipment)No ratings yet
- Clinical Audit Proposal Form: Obstetrics & GynecologyDocument4 pagesClinical Audit Proposal Form: Obstetrics & GynecologyWeam AlsouriNo ratings yet
- Local Anesthesia Made Easy: Complete Guide on How to make your Local Anesthetic Procedure a Success (Including a List of Anesthetic Equipment and their Uses)From EverandLocal Anesthesia Made Easy: Complete Guide on How to make your Local Anesthetic Procedure a Success (Including a List of Anesthetic Equipment and their Uses)No ratings yet
- Policies and Procedures On Continuous Quality ImprovementDocument16 pagesPolicies and Procedures On Continuous Quality ImprovementSooraj ThomasNo ratings yet
- Principles of More Complex ExodontiaDocument40 pagesPrinciples of More Complex ExodontiaMara CiocoNo ratings yet
- Surgery Practical Exam Rating GuideDocument3 pagesSurgery Practical Exam Rating GuideMelrose Del Pilar CondinoNo ratings yet
- Slides Surgical Instruments Update 1.7Document43 pagesSlides Surgical Instruments Update 1.7Paul Christian P. Santos, RN100% (32)
- Standing OrdersDocument18 pagesStanding OrdersVijith.V.kumar78% (9)
- General Management of A Patient Undergoing SurgeryDocument30 pagesGeneral Management of A Patient Undergoing SurgeryFan Eli100% (2)
- Drug StudyDocument10 pagesDrug StudyBandana RajpootNo ratings yet
- Seminar On Standing Orders and Protocols and Use of Selected Life SavingDocument18 pagesSeminar On Standing Orders and Protocols and Use of Selected Life SavingmalathiNo ratings yet
- Nursing FoundationDocument12 pagesNursing Foundationsangeeta palNo ratings yet
- Misoprostol - PPT 1Document61 pagesMisoprostol - PPT 1Hussein AminNo ratings yet
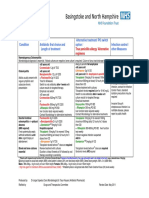
- Adult ENT Antibiotic Surgical Prophylaxis Guidelines: Full Title of Guideline: AuthorDocument7 pagesAdult ENT Antibiotic Surgical Prophylaxis Guidelines: Full Title of Guideline: Authorai naNo ratings yet
- Pedia Drug StudyDocument11 pagesPedia Drug Studyryan50% (2)
- Fundamentals of Nursing Part 1Document8 pagesFundamentals of Nursing Part 1Evergreen Verds100% (1)
- Pedia EnhancementDocument28 pagesPedia EnhancementJan Crizza Dale R. FrancoNo ratings yet
- Antibiotics-Generation OperationDocument5 pagesAntibiotics-Generation OperationZamzami Ahmad FahmiNo ratings yet
- Surgical Site Infection (SSI)Document3 pagesSurgical Site Infection (SSI)Sahrul RiadiNo ratings yet
- Paediatric Cardiac Surgical Antibiotic Prophylaxis: PurposeDocument9 pagesPaediatric Cardiac Surgical Antibiotic Prophylaxis: PurposeZamzam DomaNo ratings yet
- Antibiotic Prophylaxis in Gustilo Grade I To III Open Fractures of The Lower LimbV5 - April18th2012Document1 pageAntibiotic Prophylaxis in Gustilo Grade I To III Open Fractures of The Lower LimbV5 - April18th2012Yopi ArdhiaswariNo ratings yet
- Antibiotic Prophylaxis OrthoDocument4 pagesAntibiotic Prophylaxis OrthoDonNo ratings yet
- AHS антибиотики рекомендацDocument42 pagesAHS антибиотики рекомендацMaksym DemianchukNo ratings yet
- Commonly Used Veterinary Drugs in VTH, SPANA, DONKEY SANCTUARYDocument36 pagesCommonly Used Veterinary Drugs in VTH, SPANA, DONKEY SANCTUARYyomifNo ratings yet
- Pharmacology: Antibiotic PrescribingDocument4 pagesPharmacology: Antibiotic PrescribingekanovicaNo ratings yet
- Sepsis and Catheter Infections: Early Conversion From IV To Oral AntibioticsDocument4 pagesSepsis and Catheter Infections: Early Conversion From IV To Oral AntibioticsChaim HerreraNo ratings yet
- Recommendation For The Use of Antibiotics For The Treatment of InfectionDocument5 pagesRecommendation For The Use of Antibiotics For The Treatment of InfectionGem BorjaNo ratings yet
- Iraqi Ministry of Health Medical City Baghdad Teaching Hospital Training Center of Clinical PharmacyDocument12 pagesIraqi Ministry of Health Medical City Baghdad Teaching Hospital Training Center of Clinical PharmacyDergam HaithamNo ratings yet
- Max Fax Surgical GuidanceDocument1 pageMax Fax Surgical GuidanceMax FaxNo ratings yet
- Bone and Joint Infections BNHFT 2010 PDFDocument3 pagesBone and Joint Infections BNHFT 2010 PDFDanissa Fidia PuteriNo ratings yet
- Tetanus Treatment & Management - Approach Considerations, Initial Supportive Therapy and Wound Care, Pharmacologic TherapyDocument11 pagesTetanus Treatment & Management - Approach Considerations, Initial Supportive Therapy and Wound Care, Pharmacologic TherapyFuad Adi PrasetyoNo ratings yet
- Antibiotic PolicyDocument10 pagesAntibiotic Policykrutarth shahNo ratings yet
- Surgical Antibiotic Prophylaxis Guideline 220719Document7 pagesSurgical Antibiotic Prophylaxis Guideline 220719MuathNo ratings yet
- Antibiotic PolicyDocument16 pagesAntibiotic PolicykariNo ratings yet
- Revised: May 2018 AN: 00005/2018Document8 pagesRevised: May 2018 AN: 00005/2018Kishyorr KarthikNo ratings yet
- Subtenon Bupivacaine RCTDocument5 pagesSubtenon Bupivacaine RCTSitipradyta KasimNo ratings yet
- Injectable Contraceptives 1Document17 pagesInjectable Contraceptives 1Alfreda MeggyNo ratings yet
- Programmed Labour: Dr. Bharti KalraDocument13 pagesProgrammed Labour: Dr. Bharti KalraYoser ThamtonoNo ratings yet
- PDF Surgical Prophylaxis Poster Dec 2021Document1 pagePDF Surgical Prophylaxis Poster Dec 2021Midhun KishorNo ratings yet
- Guide Paed Bone JNTDocument11 pagesGuide Paed Bone JNTDorica GiurcaNo ratings yet
- PJI ManagementDocument11 pagesPJI ManagementHandi SuntamaNo ratings yet
- SHC Open Fracture ABX Prophylaxis GuidelineDocument2 pagesSHC Open Fracture ABX Prophylaxis GuidelineAulia OkhidNo ratings yet
- Anticipatory Analgesic Effects of Tramadol and Ibuprofen in Impacted Mandibular Third Molar Extraction A Comparative StudyDocument5 pagesAnticipatory Analgesic Effects of Tramadol and Ibuprofen in Impacted Mandibular Third Molar Extraction A Comparative StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Amoxicillin - Drug Information - UpToDateDocument47 pagesAmoxicillin - Drug Information - UpToDateMikaela lNo ratings yet
- Antibiotic Prophylaxis in Orthopedic Surgery: GeneralDocument4 pagesAntibiotic Prophylaxis in Orthopedic Surgery: GeneralWiindha Tahta Alfina CiigejeeNo ratings yet
- Meropenem Meropenem: (Lexi-Drugs Multinational)Document1 pageMeropenem Meropenem: (Lexi-Drugs Multinational)Jhoann JamanilaNo ratings yet
- Ketamin Dan Blok Peritonsiler Untuk Penatalaksanaan Nyeri Post OperasiDocument6 pagesKetamin Dan Blok Peritonsiler Untuk Penatalaksanaan Nyeri Post OperasiranirahmaniNo ratings yet
- Anesthesia ProjectDocument37 pagesAnesthesia ProjectRaj Kumar100% (1)
- BCCDC Non-Certified Practice Decision Support Tool Pelvic Inflammatory Disease (PID)Document10 pagesBCCDC Non-Certified Practice Decision Support Tool Pelvic Inflammatory Disease (PID)sandeepv08No ratings yet
- 2264-Article Text-5024-4-10-20151024Document6 pages2264-Article Text-5024-4-10-20151024shivamNo ratings yet
- Keywords:-: Ibuprofen, Ketorolac, Nsaid, Vas, Preemptive AnalgesiaDocument8 pagesKeywords:-: Ibuprofen, Ketorolac, Nsaid, Vas, Preemptive AnalgesiaAnonymous izrFWiQNo ratings yet
- MTP 170513153856Document43 pagesMTP 170513153856Sachin SinghNo ratings yet
- Antibiotics in ENT Surgery: Magdy M. Amin RIADDocument57 pagesAntibiotics in ENT Surgery: Magdy M. Amin RIAD1974sathyaNo ratings yet
- Medical Management of Closed Pyometra in A Bitch: A Case ReportDocument4 pagesMedical Management of Closed Pyometra in A Bitch: A Case ReportRonny Alberto GallegoNo ratings yet
- Efficacy of Postoperative Analgesia of Local Ketamine Wound Instillation Following Total ThyroidectomyDocument20 pagesEfficacy of Postoperative Analgesia of Local Ketamine Wound Instillation Following Total ThyroidectomyCristina RamirezNo ratings yet
- Extrapyramidal Side Effects After Metoclopramide Administration in A Post-Anesthesia Care UnitDocument3 pagesExtrapyramidal Side Effects After Metoclopramide Administration in A Post-Anesthesia Care Unitkhilwa alfaynaNo ratings yet
- Chemo Protocol PermetrexedDocument4 pagesChemo Protocol PermetrexedSangireddy NarreddyNo ratings yet
- Antibiotic Guidelines For BONE AND JOINT INFECTIONSDocument3 pagesAntibiotic Guidelines For BONE AND JOINT INFECTIONSKhurram NadeemNo ratings yet
- Tetanus Treatment NewDocument25 pagesTetanus Treatment NewDavid HermawanNo ratings yet
- Fibrion-Tetagam DXMDocument33 pagesFibrion-Tetagam DXMDella Puspita SariNo ratings yet
- AntibiocardDocument25 pagesAntibiocardchildicuNo ratings yet
- Surgical Antibiotic Prophylaxis Neurosurgery Adult and Paediatric PatientsDocument6 pagesSurgical Antibiotic Prophylaxis Neurosurgery Adult and Paediatric PatientsPraveen PadalaNo ratings yet
- Tetanus Immune Globulin (Human) : Revision Date: May 27, 2013Document3 pagesTetanus Immune Globulin (Human) : Revision Date: May 27, 2013DrscottmccallNo ratings yet
- Presentation 1Document24 pagesPresentation 1Nancy JeanetteNo ratings yet
- Why Treat Only Ill PeopleDocument6 pagesWhy Treat Only Ill PeopleIona DarkNo ratings yet
- 1 SMDocument12 pages1 SMAgung KurniawanNo ratings yet
- Comparison of Antiemetics: Pharmacist'S Letter / Prescriber'S LetterDocument6 pagesComparison of Antiemetics: Pharmacist'S Letter / Prescriber'S LetterMichelle NguyenNo ratings yet
- On A of The Appropriate Timing For Surgical Intervention in Orthognathic SurgeryDocument10 pagesOn A of The Appropriate Timing For Surgical Intervention in Orthognathic SurgeryKira LagoNo ratings yet
- New Book AnnotationsDocument1 pageNew Book Annotationslee tohNo ratings yet
- TonsillectomyDocument6 pagesTonsillectomyBen David0% (1)
- Removal of Broken HardwareDocument8 pagesRemoval of Broken Hardwarecronoss21No ratings yet
- Burst Abdomen DR TotoDocument37 pagesBurst Abdomen DR TotofahlevyNo ratings yet
- Surgical Complications of Minor Oral SurgeryDocument53 pagesSurgical Complications of Minor Oral SurgeryDrNagendra Dutt Sharma100% (1)
- ECPD YR1 Student Guidebook 2022-23Document50 pagesECPD YR1 Student Guidebook 2022-23ellieNo ratings yet
- HiQ-series Handinstruments Family-Brochure EN 20111122Document13 pagesHiQ-series Handinstruments Family-Brochure EN 20111122SILVIANo ratings yet
- GWTDocument7 pagesGWTBagus Yudha PratamaNo ratings yet
- Frenectomy Z PlastyDocument4 pagesFrenectomy Z Plastyantonio dlNo ratings yet
- Layers of Abdominal Wall When Performing An AppendicectomyDocument2 pagesLayers of Abdominal Wall When Performing An AppendicectomydrsamnNo ratings yet
- Early Postoperative Complications After Oncoplastic Reduction - PMCDocument14 pagesEarly Postoperative Complications After Oncoplastic Reduction - PMCluis david gomez gonzalezNo ratings yet
- Family PlanningDocument32 pagesFamily Planningapi-263460114No ratings yet
- Medical Error Vs Medical MalpracticeDocument12 pagesMedical Error Vs Medical MalpracticeTarrinni InastyarikusumaNo ratings yet
- Edited by Sashi S. Kommu - Evolving Trends in Urology-InTech (2012)Document88 pagesEdited by Sashi S. Kommu - Evolving Trends in Urology-InTech (2012)Diana IlieNo ratings yet
- Shouldice PDFDocument2 pagesShouldice PDFRizvi SyedNo ratings yet
- Wisdomtooth ComplicationsinextractionDocument4 pagesWisdomtooth ComplicationsinextractionMarcelo SpeschaNo ratings yet
- Final List EMP 01.02.2022Document34 pagesFinal List EMP 01.02.2022Gulshan NaddaNo ratings yet
- 2024 LHC 205Document31 pages2024 LHC 205WaqasSanaNo ratings yet
- Running Head: Post-Operative Delirium 1Document4 pagesRunning Head: Post-Operative Delirium 1Avery ElleNo ratings yet
- A Review On Concept of Trividha Karma in Shalya TantraDocument3 pagesA Review On Concept of Trividha Karma in Shalya TantraEditor IJTSRDNo ratings yet