You might also like
- Antimicrobial Therapy in Veterinary MedicineFrom EverandAntimicrobial Therapy in Veterinary MedicineSteeve GiguèreRating: 4 out of 5 stars4/5 (1)
- Surgical Site Infection (SSI)Document3 pagesSurgical Site Infection (SSI)Sahrul RiadiNo ratings yet
- Antibiotic PolicyDocument38 pagesAntibiotic Policysapphiresalem9No ratings yet
- Adult ENT Antibiotic Surgical Prophylaxis Guidelines: Full Title of Guideline: AuthorDocument7 pagesAdult ENT Antibiotic Surgical Prophylaxis Guidelines: Full Title of Guideline: Authorai naNo ratings yet
- AHS антибиотики рекомендацDocument42 pagesAHS антибиотики рекомендацMaksym DemianchukNo ratings yet
- Neurosurgery Antibiotic GuideDocument6 pagesNeurosurgery Antibiotic GuidePraveen PadalaNo ratings yet
- Antibiotics in NeurosurgeryDocument12 pagesAntibiotics in Neurosurgerylouglee9174100% (1)
- Antibiotic Prophylaxis in Surgery GuideDocument5 pagesAntibiotic Prophylaxis in Surgery GuideKhairul MustafaNo ratings yet
- Lewis and Culligan GYN SSI Reduction 42Document5 pagesLewis and Culligan GYN SSI Reduction 42Ahmed Mohamed SalehNo ratings yet
- Surgical Antibiotic Prophylaxis GuidelineDocument7 pagesSurgical Antibiotic Prophylaxis GuidelineConstantin BudinNo ratings yet
- Tuberculosis Treatment, MDR, XDR, Resistance, Prophylaxis, VaccinationDocument44 pagesTuberculosis Treatment, MDR, XDR, Resistance, Prophylaxis, Vaccinationskeisham11No ratings yet
- Adult Patient Diagnosed With COVID-19: Ministry of Health & Family Welfare, Government of IndiaDocument1 pageAdult Patient Diagnosed With COVID-19: Ministry of Health & Family Welfare, Government of Indiapramodbankhele3845No ratings yet
- COVID Clinical Management 14012022Document1 pageCOVID Clinical Management 14012022Naina DesaiNo ratings yet
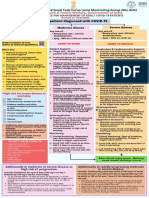
- National Task Force Clinical Guidance for Managing Adult COVID-19 PatientsDocument1 pageNational Task Force Clinical Guidance for Managing Adult COVID-19 PatientsWhiteNo ratings yet
- Single-dose antibiotic prophylaxis more cost-effective than conventional therapyDocument5 pagesSingle-dose antibiotic prophylaxis more cost-effective than conventional therapyكنNo ratings yet
- Antibiotic Guidelines For BONE AND JOINT INFECTIONSDocument3 pagesAntibiotic Guidelines For BONE AND JOINT INFECTIONSKhurram NadeemNo ratings yet
- Wa0094.Document9 pagesWa0094.lider vigilanciaNo ratings yet
- Literature Reading: HomeworkDocument3 pagesLiterature Reading: HomeworkMuhamad Sidik HasanudinNo ratings yet
- Antimicrobials in Gynaecological PracticeDocument5 pagesAntimicrobials in Gynaecological PracticeannisanabilaasNo ratings yet
- Cefazolin (Ancef ®) : D5W, NsDocument9 pagesCefazolin (Ancef ®) : D5W, Nsbabe5606No ratings yet
- CrosstownGeneralSurgeryGuidelineFinal Nov 2007Document8 pagesCrosstownGeneralSurgeryGuidelineFinal Nov 2007Sri Nurliana BasryNo ratings yet
- Surgical Antibiotic ProphylaxisDocument3 pagesSurgical Antibiotic Prophylaxisbellahunter92No ratings yet
- Enhanced Recovery After Surgery ProtocolsDocument5 pagesEnhanced Recovery After Surgery ProtocolsProsanta Kr BhattacharjeeNo ratings yet
- Paediatric Cardiac Surgical Antibiotic Prophylaxis: PurposeDocument9 pagesPaediatric Cardiac Surgical Antibiotic Prophylaxis: PurposeZamzam DomaNo ratings yet
- Meropenem Meropenem: (Lexi-Drugs Multinational)Document1 pageMeropenem Meropenem: (Lexi-Drugs Multinational)Jhoann JamanilaNo ratings yet
- Iraqi Ministry of Health Medical City Baghdad Teaching Hospital Training Center of Clinical PharmacyDocument40 pagesIraqi Ministry of Health Medical City Baghdad Teaching Hospital Training Center of Clinical PharmacyLolo GhostNo ratings yet
- Surgical Antibiotic Prophylaxis Duration Position Statement October 2021 v1Document3 pagesSurgical Antibiotic Prophylaxis Duration Position Statement October 2021 v1debby twonabilaNo ratings yet
- 842 Erskine MythsDocument3 pages842 Erskine MythsFranz Josef TariganNo ratings yet
- Effect of The Site of Infection On Therapy: The Blood-Brain BarrierDocument11 pagesEffect of The Site of Infection On Therapy: The Blood-Brain BarrierTamim Al-TamimiNo ratings yet
- Antibiotic Prophylaxis in SurgeryDocument10 pagesAntibiotic Prophylaxis in SurgeryHaSan Z. MustafaNo ratings yet
- Rational Use of AntibioticsDocument39 pagesRational Use of Antibioticsjun sianNo ratings yet
- Pocket Guide, January 1, 2014 Version Urologic Surgery Antimicrobial Prophyl A XisDocument3 pagesPocket Guide, January 1, 2014 Version Urologic Surgery Antimicrobial Prophyl A XisPraveen RavishankaranNo ratings yet
- Treating Tetanus: Support, Wound Care, AntitoxinsDocument11 pagesTreating Tetanus: Support, Wound Care, AntitoxinsFuad Adi PrasetyoNo ratings yet
- Guideline For Antimicrobial Use in The Orthopaedic and Trauma Department..Document8 pagesGuideline For Antimicrobial Use in The Orthopaedic and Trauma Department..Long Nguyễn HoàngNo ratings yet
- Nosocomial Pneumonia RXDocument3 pagesNosocomial Pneumonia RXCHETAN SOMUNo ratings yet
- Recommendation For The Use of Antibiotics For The Treatment of InfectionDocument5 pagesRecommendation For The Use of Antibiotics For The Treatment of InfectionGem BorjaNo ratings yet
- Folfiri+cetu Gi Col PDocument12 pagesFolfiri+cetu Gi Col PJayelle2No ratings yet
- Week 4 Chemotherapeutic AgentsDocument339 pagesWeek 4 Chemotherapeutic AgentsLassie AbusadoNo ratings yet
- Respiratory SlidesDocument40 pagesRespiratory SlidesmaheshNo ratings yet
- Cephalosporins in Surgical Prophylaxis: ReviewDocument4 pagesCephalosporins in Surgical Prophylaxis: ReviewGemara HanumNo ratings yet
- DUREMDES KAYLA NICOLE Care For Clients With Rheumatic Disease and Immunodeficiency Critical ThinkinDocument4 pagesDUREMDES KAYLA NICOLE Care For Clients With Rheumatic Disease and Immunodeficiency Critical ThinkinOPERAñA ELLAYZA RB DECANONo ratings yet
- Antibiotik ProfilaksisDocument2 pagesAntibiotik ProfilaksisAdel ZilviaNo ratings yet
- Hepatotoxic Effects of Therapies For TuberculosisDocument14 pagesHepatotoxic Effects of Therapies For TuberculosisCarlos LuqueNo ratings yet
- The Rational Use Of: AntibioticsDocument28 pagesThe Rational Use Of: AntibioticsdanielaNo ratings yet
- Antibiotic Prophylaxis in SurgeryDocument23 pagesAntibiotic Prophylaxis in SurgeryRakhmad AdityaNo ratings yet
- Surviving Sepsis Campaign 2021Document28 pagesSurviving Sepsis Campaign 2021Hanny Melati HarahapNo ratings yet
- Antimicrobial ProphylaxisDocument2 pagesAntimicrobial ProphylaxisbournvilleeaterNo ratings yet
- Amoxicillin - Drug Information - UpToDateDocument47 pagesAmoxicillin - Drug Information - UpToDateMikaela lNo ratings yet
- Antibiotics in ENT Surgery: Magdy M. Amin RIADDocument57 pagesAntibiotics in ENT Surgery: Magdy M. Amin RIAD1974sathyaNo ratings yet
- Chemo ProphylaxisDocument13 pagesChemo ProphylaxisSaket DaokarNo ratings yet
- Nursing Care Plan For ThyroidectomyDocument5 pagesNursing Care Plan For ThyroidectomyHARVEY SELIM100% (1)
- Colomycin: What Colomycin Is and What It Used ForDocument5 pagesColomycin: What Colomycin Is and What It Used ForHusam ShawaqfehNo ratings yet
- VancomycinDocument1 pageVancomycinE100% (2)
- Prescribing Tables To Guide Decision Making About AntibioticDocument2 pagesPrescribing Tables To Guide Decision Making About AntibioticDusan OrescaninNo ratings yet
- Rational Use of AntibioticsDocument27 pagesRational Use of AntibioticsTesfaye MegersaNo ratings yet
- Risk Factor PneumoniaDocument6 pagesRisk Factor Pneumoniaali subchanNo ratings yet
- Avent Et Al-2011-Internal Medicine JournalDocument9 pagesAvent Et Al-2011-Internal Medicine JournalAgil Wahyu WicaksonoNo ratings yet
- Everything You Need to Know About Using Antibiotics in SurgeryDocument29 pagesEverything You Need to Know About Using Antibiotics in SurgeryRony RonyNo ratings yet
- Anes 10 3 9Document7 pagesAnes 10 3 9ema moralesNo ratings yet
- Antibiotics-Generation OperationDocument5 pagesAntibiotics-Generation OperationZamzami Ahmad FahmiNo ratings yet
- A K UDocument1 pageA K UZamzami Ahmad FahmiNo ratings yet
- Fracturas Deprimidas PDFDocument5 pagesFracturas Deprimidas PDFAndrés SeguraNo ratings yet
- Good ManDocument2 pagesGood ManZamzami Ahmad FahmiNo ratings yet
- Aim of AyurvedaDocument5 pagesAim of Ayurvedaravisha7kNo ratings yet
- Revised Tle DLLDocument2 pagesRevised Tle DLLJeslie Ann Viñas Cagurungan100% (1)
- Review NotesDocument10 pagesReview NotesPatziedawn GonzalvoNo ratings yet
- AGGRESSIONDocument28 pagesAGGRESSIONMichelle Therese100% (1)
- NCP For Rapid Shallow BreathingDocument1 pageNCP For Rapid Shallow Breathingbamboo2dNo ratings yet
- 1-Collection, Storage and Transportataion of MicrobiologicalDocument49 pages1-Collection, Storage and Transportataion of MicrobiologicalSummi NizNo ratings yet
- Movements of The Cheng Man Ching 37 Form - Just Breathe - Tai Chi - Qigong - YogaDocument4 pagesMovements of The Cheng Man Ching 37 Form - Just Breathe - Tai Chi - Qigong - YogalNo ratings yet
- Vulva CancerDocument2 pagesVulva CancerLim Hui ZhuanNo ratings yet
- Vol BellaDocument33 pagesVol BellaJonathan David Contreras InfanteNo ratings yet
- Qingling Haung Resume - HcaDocument4 pagesQingling Haung Resume - Hcaapi-317607382No ratings yet
- Elyse Torres Resume NowDocument2 pagesElyse Torres Resume Nowapi-395806896No ratings yet
- Septage FAQ Brochure - EnglishDocument2 pagesSeptage FAQ Brochure - EnglishMeghan EbuezaNo ratings yet
- Social Work Group Practice: Models, Stages, SettingsDocument22 pagesSocial Work Group Practice: Models, Stages, SettingsZahoor Ahmad100% (2)
- Reading-Health and Wellness On The GoDocument4 pagesReading-Health and Wellness On The GoAltan CoşkunNo ratings yet
- Practical MoxibustionDocument95 pagesPractical Moxibustionzhik100% (12)
- Deriva MSDocument42 pagesDeriva MSkurutalaNo ratings yet
- Encircle The Best Answer: C) Health Means Not Seeing A DoctorDocument7 pagesEncircle The Best Answer: C) Health Means Not Seeing A DoctorMuhammad Usman KhanNo ratings yet
- Know Your Magnetic FieldDocument75 pagesKnow Your Magnetic FieldAtma Jnani100% (5)
- AuriculotherapyDocument7 pagesAuriculotherapy4gen_7No ratings yet
- Nutritional Analysis of Blenderized Enteral Diets in The PhilippinesDocument6 pagesNutritional Analysis of Blenderized Enteral Diets in The PhilippinesDeni WasistaNo ratings yet
- Neuromuscular Blocking DrugsDocument22 pagesNeuromuscular Blocking DrugsMuhammad Shahid BilalNo ratings yet
- Nichele Filicetti BioDocument1 pageNichele Filicetti BiojaclynrevisNo ratings yet
- Measuring Chlorine Concentration in Water SamplesDocument4 pagesMeasuring Chlorine Concentration in Water SamplesJai MurugeshNo ratings yet
- American BeautyDocument17 pagesAmerican BeautyiamELHIZA100% (4)
- The Ayurvedic Vegan KitchenDocument203 pagesThe Ayurvedic Vegan KitchenHarshad Ashodiya Interior Designer100% (6)
- Medical ForcepsDocument9 pagesMedical ForcepsRachel Ann JimenezNo ratings yet
- 03 Ellman Surgitron 4.0 MHZ Dual RF 120 IEC User ManualDocument32 pages03 Ellman Surgitron 4.0 MHZ Dual RF 120 IEC User ManualDaniele0% (1)
- Efficacy of Levetiracetam in The Treatment Of.21Document3 pagesEfficacy of Levetiracetam in The Treatment Of.21andiNo ratings yet
- Write Cure Codes On Your Arms and Save Yourself From Incurable DiseaseDocument3 pagesWrite Cure Codes On Your Arms and Save Yourself From Incurable DiseaseZindagiDee100% (1)
- 10 - Occupational Stress Reflections On Theory and PracticeDocument15 pages10 - Occupational Stress Reflections On Theory and PracticeCatedra PsihologieNo ratings yet