You might also like
- Further Practice-W11.1Document5 pagesFurther Practice-W11.1Binh Pham Thanh0% (3)
- Long Haul COVID-19 ProtocolDocument3 pagesLong Haul COVID-19 ProtocolAizaz ul HaqNo ratings yet
- FLCCC Alliance's I RECOVER Management Protocol For Long Haul COVID 19 SyndromeDocument3 pagesFLCCC Alliance's I RECOVER Management Protocol For Long Haul COVID 19 SyndromeAlan N100% (1)
- Stroke Society of the Philippines: Guide for Stroke TreatmentDocument22 pagesStroke Society of the Philippines: Guide for Stroke TreatmentSuresh ShresthaNo ratings yet
- COVID vaccination certificateDocument2 pagesCOVID vaccination certificateGeorge HonciugNo ratings yet
- Dental Clinical Advisor PDFDocument589 pagesDental Clinical Advisor PDFRishabh Kapoor100% (4)
- Folfiri Beva Gi Col PDocument12 pagesFolfiri Beva Gi Col Pvera docNo ratings yet
- Ema-Co Gy GTDDocument4 pagesEma-Co Gy GTDTowhidulIslamNo ratings yet
- Chemo Protocol PermetrexedDocument4 pagesChemo Protocol PermetrexedSangireddy NarreddyNo ratings yet
- Gigfolfiri ProtocolDocument6 pagesGigfolfiri ProtocolNurfarah BilqisNo ratings yet
- CetuximabDocument8 pagesCetuximabcrespo2816100% (1)
- Beacopp Hem HL ADocument8 pagesBeacopp Hem HL AAnonymous 9dVZCnTXSNo ratings yet
- Epirubicin X Docetaxel LcaDocument8 pagesEpirubicin X Docetaxel LcaAulia WidyaNo ratings yet
- SMILEPEG HEM TCell ADocument5 pagesSMILEPEG HEM TCell Aphillip.chung89No ratings yet
- Capecitabine 14 DayDocument6 pagesCapecitabine 14 DaybrystyyNo ratings yet
- Carboplatin With Pemetrexed Pembrolizumab Non Squamous Non-Small Cell Lung Cancer Protocol V1.1Document8 pagesCarboplatin With Pemetrexed Pembrolizumab Non Squamous Non-Small Cell Lung Cancer Protocol V1.1Olaru DianaNo ratings yet
- I.5 - Ab Necrotizing FasciitisDocument16 pagesI.5 - Ab Necrotizing FasciitisShameen KhanNo ratings yet
- VeIP GU TESDocument6 pagesVeIP GU TESMohan KumarNo ratings yet
- 311 Topotecan Monotherapy 5 DayDocument4 pages311 Topotecan Monotherapy 5 DayRuxandra BănicăNo ratings yet
- Brajac - ProtocolDocument13 pagesBrajac - Protocolthanh ngôNo ratings yet
- Antibiotics-Generation OperationDocument5 pagesAntibiotics-Generation OperationZamzami Ahmad FahmiNo ratings yet
- LYRICE ProtocolDocument6 pagesLYRICE ProtocolInas UthmanNo ratings yet
- Long Haul COVID-19 Recovery ProtocolDocument3 pagesLong Haul COVID-19 Recovery ProtocolSterr LiingNo ratings yet
- Vancomycin Protocol RQHRDocument15 pagesVancomycin Protocol RQHRl1o2stNo ratings yet
- L 44 Bendamustine 70 R CLLDocument7 pagesL 44 Bendamustine 70 R CLLsatishNo ratings yet
- Capecitabine Irinotecan (CAPIRI) Administration & Toxicity GuideDocument5 pagesCapecitabine Irinotecan (CAPIRI) Administration & Toxicity GuideSindu SankarNo ratings yet
- Cetuximab-200mg Per 100ml InjectionDocument17 pagesCetuximab-200mg Per 100ml InjectionMd. Abdur RahmanNo ratings yet
- Ovarian Cancer Treatment Regimens - Print Article - Cancer Therapy AdvisorDocument5 pagesOvarian Cancer Treatment Regimens - Print Article - Cancer Therapy AdvisorAnonymous g1hIPZNo ratings yet
- IV PO Conversion P&P.V2Document3 pagesIV PO Conversion P&P.V2damondouglasNo ratings yet
- Atezolizumab-FDA LabelDocument38 pagesAtezolizumab-FDA LabelClarissa BCNo ratings yet
- Oritavancin Orbactiv MonographDocument11 pagesOritavancin Orbactiv MonographDani11No ratings yet
- Capecitabine IrinotecanDocument7 pagesCapecitabine Irinotecantanasa adrianNo ratings yet
- Vaccinations Guideline Summary 2022Document4 pagesVaccinations Guideline Summary 2022Faisal PNo ratings yet
- Irinotecan Concentrate for Colorectal CancerDocument24 pagesIrinotecan Concentrate for Colorectal CancerSrechko MilichNo ratings yet
- Cyclophosphamide Doxorubicin Ver 1.1Document6 pagesCyclophosphamide Doxorubicin Ver 1.1Yudi ApriyantoNo ratings yet
- Low Molecular Weight Heparins (LMWH) : I. Mechanism of ActionDocument7 pagesLow Molecular Weight Heparins (LMWH) : I. Mechanism of ActionIniya RajendranNo ratings yet
- Peritonitis in Peritoneal Dialysis Patients 1.0 PDFDocument12 pagesPeritonitis in Peritoneal Dialysis Patients 1.0 PDFIndo MahardikaNo ratings yet
- 1.3.1.1 Ireland Tavanic 500mg SMPC PDFDocument19 pages1.3.1.1 Ireland Tavanic 500mg SMPC PDFНатали КапанадзеNo ratings yet
- Mifepristone Misoprostol Abortion ProtocolDocument6 pagesMifepristone Misoprostol Abortion ProtocolFawaaz KhurwolahNo ratings yet
- Acute Pyelonephritis AdultDocument1 pageAcute Pyelonephritis AdultMeagan SotoNo ratings yet
- (R) Choep: IndicationDocument5 pages(R) Choep: IndicationAlina CrissNo ratings yet
- 2020 Ketamine-Propofol For ProceduralDocument14 pages2020 Ketamine-Propofol For ProceduralAlexis Ormeño JulcaNo ratings yet
- ANTIBIOTIC POLICY FOR Sassoon Hospital & BJGMC, PuneDocument32 pagesANTIBIOTIC POLICY FOR Sassoon Hospital & BJGMC, Puneshah007zaadNo ratings yet
- CP PMN 248Document5 pagesCP PMN 248riwandaNo ratings yet
- Surgical Site Infection (SSI)Document3 pagesSurgical Site Infection (SSI)Sahrul RiadiNo ratings yet
- Guideline: Antibiotic Drug Monitoring: Aminoglycosides and GlycopeptidesDocument8 pagesGuideline: Antibiotic Drug Monitoring: Aminoglycosides and GlycopeptidesKenRodulfReyesVillaruelNo ratings yet
- Abvd Hem HLDocument6 pagesAbvd Hem HLTowhidulIslamNo ratings yet
- Ovarian Germ Cell Tumors Treatment EssentialsDocument7 pagesOvarian Germ Cell Tumors Treatment EssentialsMuhammad Ferhat E.S.No ratings yet
- L 51 R Hypercvad R MaDocument7 pagesL 51 R Hypercvad R MaMohamed MahmoudNo ratings yet
- Case-Based Learning Nausea and Vomiting: Sang Ayu Putu Wahyu Pratiwi NIM. 2208612048Document8 pagesCase-Based Learning Nausea and Vomiting: Sang Ayu Putu Wahyu Pratiwi NIM. 2208612048sang ayu putu wahyu pratiwi233No ratings yet
- ABVDDocument3 pagesABVDEsther WanguiNo ratings yet
- Pharmacy and Pharmacy and Pharmacy and Pharmacy and Therapeutics Therapeutics Therapeutics Therapeutics Newsletter Newsletter Newsletter NewsletterDocument2 pagesPharmacy and Pharmacy and Pharmacy and Pharmacy and Therapeutics Therapeutics Therapeutics Therapeutics Newsletter Newsletter Newsletter NewsletterAnonymous Ou02SWgGZNo ratings yet
- Sepsis and Catheter Infections: Early Conversion From IV To Oral AntibioticsDocument4 pagesSepsis and Catheter Infections: Early Conversion From IV To Oral AntibioticsChaim HerreraNo ratings yet
- Prescribing Tables To Guide Decision Making About AntibioticDocument2 pagesPrescribing Tables To Guide Decision Making About AntibioticDusan OrescaninNo ratings yet
- 249 Intrathecal Methotrexate For Cns Prophylaxis in GTNDocument3 pages249 Intrathecal Methotrexate For Cns Prophylaxis in GTNparamitaekadevaNo ratings yet
- ULUAVNIV ProtocolDocument10 pagesULUAVNIV ProtocolsatishNo ratings yet
- Neratinib Adjuvant Treatment Breast Cancer Protocol V1.1Document6 pagesNeratinib Adjuvant Treatment Breast Cancer Protocol V1.1smokkerNo ratings yet
- Perioperative Steroid GuidelineDocument3 pagesPerioperative Steroid Guidelinebellahunter92No ratings yet
- BC Cancer High-Alert Medications Policy AppendicesDocument10 pagesBC Cancer High-Alert Medications Policy AppendicesAbdur RachmanNo ratings yet
- Antiemetic Guidelines For ChemotherapyDocument11 pagesAntiemetic Guidelines For ChemotherapyAaron AntonioNo ratings yet
- Oncology Antiemetic PolicyDocument8 pagesOncology Antiemetic PolicyAnggy L, dr.No ratings yet
- Cisplatin/ 5-Fluorouracil For Squamous Cell Carcinoma Head and Neck (HNSCC) - Day Unit ProtocolDocument6 pagesCisplatin/ 5-Fluorouracil For Squamous Cell Carcinoma Head and Neck (HNSCC) - Day Unit Protocoldwi harisNo ratings yet
- 1.13 Hyper-CVAD-MA Version 2.1Document5 pages1.13 Hyper-CVAD-MA Version 2.1Alina CrissNo ratings yet
- Frontiers in Clinical Drug Research - Anti-Cancer Agents: Volume 5From EverandFrontiers in Clinical Drug Research - Anti-Cancer Agents: Volume 5No ratings yet
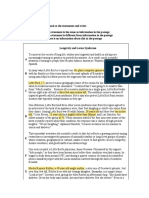
- Rough Draft Coffee ConsumptionDocument5 pagesRough Draft Coffee ConsumptionMariana Cedeño RamosNo ratings yet
- Family Violence Legal Medical and Social Perspectives 7th Wallace Test BankDocument10 pagesFamily Violence Legal Medical and Social Perspectives 7th Wallace Test BankTravis Bogan100% (35)
- Rhinosinusitis: Classification, Symptoms, Diagnosis and TreatmentDocument16 pagesRhinosinusitis: Classification, Symptoms, Diagnosis and TreatmentVictor EnachiNo ratings yet
- Cephalosphorins 3rd Gen 4rt GenDocument24 pagesCephalosphorins 3rd Gen 4rt GenshaitabliganNo ratings yet
- 3 - Evaluation and Management of Rheumatoid ArthritisDocument56 pages3 - Evaluation and Management of Rheumatoid ArthritisDwi Astika SariNo ratings yet
- Prostate Cancer Clinical Pathway - July 2020Document4 pagesProstate Cancer Clinical Pathway - July 2020VincentEguzoNo ratings yet
- Celiac Nutri Geno MixDocument20 pagesCeliac Nutri Geno MixGabriela PrecupNo ratings yet
- PacemakersDocument8 pagesPacemakersVIVEK Kumar Prajapati 72No ratings yet
- Lecture 23 - Gastrointestinal Tract - Part 2 - Clinical CorrelatesDocument36 pagesLecture 23 - Gastrointestinal Tract - Part 2 - Clinical Correlatesspitzmark2030No ratings yet
- RV Ollero MD's Guide to Advanced Trauma Life SupportDocument18 pagesRV Ollero MD's Guide to Advanced Trauma Life SupportPrincess Cate MercadoNo ratings yet
- NCPDocument3 pagesNCPAlexis CoronadoNo ratings yet
- Surgical Site InfectionDocument7 pagesSurgical Site InfectionCaxton ThumbiNo ratings yet
- Drug Study01Document6 pagesDrug Study01JrBong SemaneroNo ratings yet
- Medical History ChecklistDocument2 pagesMedical History ChecklistChristopher LaneNo ratings yet
- EczemaDocument23 pagesEczemaPn Ziza AzwaNo ratings yet
- SchizophreniaDocument5 pagesSchizophreniamercyNo ratings yet
- PsychiartryDocument7 pagesPsychiartryNeeraj SahuNo ratings yet
- Cholestatic Liver Disease & Jaundice: Dr. David Minter, D.ODocument79 pagesCholestatic Liver Disease & Jaundice: Dr. David Minter, D.ONabeel ShahzadNo ratings yet
- RICE or MEAT Protocol For Acute Ligament Sprain TreatmentDocument3 pagesRICE or MEAT Protocol For Acute Ligament Sprain TreatmentEric HoNo ratings yet
- Cannabis TherapeuticDocument26 pagesCannabis TherapeuticRafael IgnacioNo ratings yet
- Needle Prick Injury & PreventionDocument17 pagesNeedle Prick Injury & Preventioniman zainuddinNo ratings yet
- Salvestrols Cures CancerDocument29 pagesSalvestrols Cures CancerJohn Tan100% (1)
- Icf Write-Up Based On Diagnosis LouelDocument7 pagesIcf Write-Up Based On Diagnosis Louelapi-270650064No ratings yet
- Sush Corrected-Unity PSYCH 1700 PDFDocument218 pagesSush Corrected-Unity PSYCH 1700 PDFDr-Jahanzaib GondalNo ratings yet
- Arjo - Flowtron Excel Specs Sheet.1.0.INT - ENDocument4 pagesArjo - Flowtron Excel Specs Sheet.1.0.INT - ENAhmed El KadyNo ratings yet
- NCP3 Skin IntegrityDocument3 pagesNCP3 Skin IntegrityAngela NeriNo ratings yet