You might also like
- Drug Study (Haloperidol)Document3 pagesDrug Study (Haloperidol)Mae Ann Bueno CastillonNo ratings yet
- A Text Book of Materia Medica and Therapeutics of Rare Homoeopathic Remedies by Oscar HansenDocument136 pagesA Text Book of Materia Medica and Therapeutics of Rare Homoeopathic Remedies by Oscar Hansensunnyjamiel75% (4)
- Drug Classification Action Indication Contraindication Nursing ResposibilitiesDocument10 pagesDrug Classification Action Indication Contraindication Nursing ResposibilitiesAngelicaNo ratings yet
- 8 Propofol Drug StudyDocument4 pages8 Propofol Drug Studyshadow gonzalez100% (1)
- 90 MCQsDocument18 pages90 MCQsMarielou CoutinhoNo ratings yet
- Pediatric Resucitation Pediatric Resucitation: Pgi Gasataya, Charisse Ann G Pgi Tabobo, Raymee TDocument30 pagesPediatric Resucitation Pediatric Resucitation: Pgi Gasataya, Charisse Ann G Pgi Tabobo, Raymee TCharisse Ann GasatayaNo ratings yet
- Medical Surgical Nursing Review NotesDocument209 pagesMedical Surgical Nursing Review Notesabusaifluay100% (1)
- CpapDocument33 pagesCpapAtikah Putri AtmojoNo ratings yet
- Neonatal and Pediatric Patient Assessment (Study Guide)Document17 pagesNeonatal and Pediatric Patient Assessment (Study Guide)Fatima Sherrisa SaliNo ratings yet
- Long Covid - The Long Covid Book for Clinicians and Sufferers - Away from Despair and Towards UnderstandingFrom EverandLong Covid - The Long Covid Book for Clinicians and Sufferers - Away from Despair and Towards UnderstandingNo ratings yet
- NCLEX Exam: Respiratory System Disorders (60 Questions) : CorrectDocument41 pagesNCLEX Exam: Respiratory System Disorders (60 Questions) : CorrectErica Veluz LuyunNo ratings yet
- Coronary Artery Disease Pathophysiology PDFDocument3 pagesCoronary Artery Disease Pathophysiology PDFMohd Amir Bin Bashir0% (1)
- 004 Practical-Manual PDFDocument72 pages004 Practical-Manual PDFRicardo Domingos100% (1)
- NCP CompilationDocument11 pagesNCP CompilationRene John FranciscoNo ratings yet
- VancomycinDocument1 pageVancomycinE100% (2)
- BudesonideDocument2 pagesBudesonideDiane Bonita HerreraNo ratings yet
- Mcce CanadaDocument436 pagesMcce CanadakabambaNo ratings yet
- NCP Activity IntoleranceDocument1 pageNCP Activity IntoleranceBen David100% (2)
- National Task Force Clinical Guidance for Managing Adult COVID-19 PatientsDocument1 pageNational Task Force Clinical Guidance for Managing Adult COVID-19 PatientsWhiteNo ratings yet
- Adult Patient Diagnosed With COVID-19: Ministry of Health & Family Welfare, Government of IndiaDocument1 pageAdult Patient Diagnosed With COVID-19: Ministry of Health & Family Welfare, Government of Indiapramodbankhele3845No ratings yet
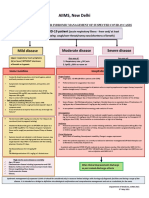
- AIIMS COVID Algorithm Ver 2.0Document1 pageAIIMS COVID Algorithm Ver 2.0jimjose antonyNo ratings yet
- COVID19 Management Algorithm 22042021 v1Document1 pageCOVID19 Management Algorithm 22042021 v1shivani shindeNo ratings yet
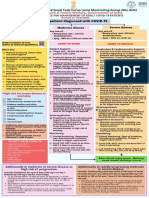
- AIIMS/ ICMR-COVID-19 National Task Force/ Joint Monitoring Group (Dte - GHS) Ministry of Health & Family Welfare, Government of IndiaDocument1 pageAIIMS/ ICMR-COVID-19 National Task Force/ Joint Monitoring Group (Dte - GHS) Ministry of Health & Family Welfare, Government of IndiaSomnath Das GuptaNo ratings yet
- AIIMS COVID Algorithm 1.5-1 PDFDocument1 pageAIIMS COVID Algorithm 1.5-1 PDFAnutosh BhaskarNo ratings yet
- INTERIM CLINICAL GUIDANCE FOR MANAGEMENT OF COVID-19Document1 pageINTERIM CLINICAL GUIDANCE FOR MANAGEMENT OF COVID-19mbhangaleNo ratings yet
- AIIMS Issues New Guidelines For Treatment of CovidDocument7 pagesAIIMS Issues New Guidelines For Treatment of Covidsenthil kumarNo ratings yet
- AIIMS issues new guidelines for treatment of Covid-19 casesDocument7 pagesAIIMS issues new guidelines for treatment of Covid-19 casessenthil kumarNo ratings yet
- AIIMS Syndromic ApproachDocument1 pageAIIMS Syndromic ApproachRagul VNo ratings yet
- FluticasoneDocument3 pagesFluticasoneAmberNo ratings yet
- Pharm Exam Ii NotesDocument24 pagesPharm Exam Ii Noteskatiana louisNo ratings yet
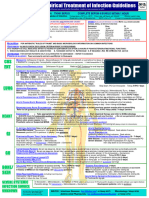
- Recommendation For The Use of Antibiotics For The Treatment of InfectionDocument5 pagesRecommendation For The Use of Antibiotics For The Treatment of InfectionGem BorjaNo ratings yet
- COVID-19 InterimGuidelines Treatment ENGDocument25 pagesCOVID-19 InterimGuidelines Treatment ENGMartin PaturlanneNo ratings yet
- WB Covid Protocol Book 25.09 .20 (1)Document49 pagesWB Covid Protocol Book 25.09 .20 (1)El MirageNo ratings yet
- Treatment Protocol Covid-19Document4 pagesTreatment Protocol Covid-19Shiv singhNo ratings yet
- WB COVID19 Latest Treatment ProtocolDocument1 pageWB COVID19 Latest Treatment ProtocolRahul AwasthiNo ratings yet
- Antibiotics-Generation OperationDocument5 pagesAntibiotics-Generation OperationZamzami Ahmad FahmiNo ratings yet
- COVID-19 InterimGuidelines Treatment ENGDocument24 pagesCOVID-19 InterimGuidelines Treatment ENGHouda LaatabiNo ratings yet
- GHC Lower Respiratory Tract Antimicrobial Guideline V 3 FinalDocument19 pagesGHC Lower Respiratory Tract Antimicrobial Guideline V 3 FinalNicthe Ruiz RodríguezNo ratings yet
- Meropenem Meropenem: (Lexi-Drugs Multinational)Document1 pageMeropenem Meropenem: (Lexi-Drugs Multinational)Jhoann JamanilaNo ratings yet
- Component 3: Pharmacologic TherapyDocument47 pagesComponent 3: Pharmacologic TherapypharmryadNo ratings yet
- PrednisoneDocument3 pagesPrednisoneShaira TanNo ratings yet
- Pedoman Penggunaan Antibiotik Pada PasienDocument5 pagesPedoman Penggunaan Antibiotik Pada PasienErvina Lie100% (1)
- Rheumatic Heart DDocument12 pagesRheumatic Heart DHein HtetNo ratings yet
- Croup Summary PDFDocument2 pagesCroup Summary PDFnurfitriaNo ratings yet
- CortisoneDocument2 pagesCortisoneJulioNo ratings yet
- DrugsDocument2 pagesDrugsgailannreyesNo ratings yet
- DrugsDocument2 pagesDrugsgailannreyesNo ratings yet
- Ventilator: Associated Pneumonia (VAP)Document36 pagesVentilator: Associated Pneumonia (VAP)D. Melba S.S ChinnaNo ratings yet
- Midazolam FinalDocument2 pagesMidazolam FinalAhmad AbqariNo ratings yet
- Adverse Effects of Anti Tubercular Drugs. MDR TBDocument75 pagesAdverse Effects of Anti Tubercular Drugs. MDR TBDr.U.P.Rathnakar.MD.DIH.PGDHM100% (1)
- DIPIRO 9th PHARMACOTHERAPY-PATOPHISIOLOGY APPROACH EDISI 9 (PDF - Io)Document31 pagesDIPIRO 9th PHARMACOTHERAPY-PATOPHISIOLOGY APPROACH EDISI 9 (PDF - Io)NingrumSindayaniNo ratings yet
- COVID-19 Guidelines for Management of PatientsDocument2 pagesCOVID-19 Guidelines for Management of PatientsSpecial OPD SVMCHRCNo ratings yet
- Nutrition and Fluid Therapy: CroupDocument2 pagesNutrition and Fluid Therapy: CroupnasibdinNo ratings yet
- Antibiotic hospital manDocument1 pageAntibiotic hospital manarshiya.manasekiNo ratings yet
- COVID - Management 14 April 2021Document20 pagesCOVID - Management 14 April 2021Zain ZaidiNo ratings yet
- Bronchial AsthmaDocument45 pagesBronchial Asthmaprincesszahra6498No ratings yet
- Drug Study No.1 Brand Name: Paracetamol Generic Name: Tempra Classification: Anti-Infectives Dosage: 100mg, 1ml Drops q4hrDocument7 pagesDrug Study No.1 Brand Name: Paracetamol Generic Name: Tempra Classification: Anti-Infectives Dosage: 100mg, 1ml Drops q4hrMary EnsomoNo ratings yet
- COVID MX BsmmuDocument2 pagesCOVID MX BsmmuNuhiat NahreenNo ratings yet
- COVID-19 Infection in Children GuideDocument12 pagesCOVID-19 Infection in Children GuideSutirtha RoyNo ratings yet
- Sedation & Analgesia in PICU: Goals, Tools and Adjuvant TherapyDocument21 pagesSedation & Analgesia in PICU: Goals, Tools and Adjuvant TherapyDr AhmedNo ratings yet
- Covid Drug TherapyDocument35 pagesCovid Drug TherapyNandha KumarNo ratings yet
- Methylprednisolone Drug Profile and Nursing ConsiderationsDocument4 pagesMethylprednisolone Drug Profile and Nursing ConsiderationsadryananestesiNo ratings yet
- Medical Ward Drug StudyDocument9 pagesMedical Ward Drug StudygorgeazNo ratings yet
- ASTHMA RestriveraDocument18 pagesASTHMA RestriveraAoi ShinNo ratings yet
- BNM Covid FrancesDocument4 pagesBNM Covid FrancesMISSAEL ESPINOZANo ratings yet
- Management of Acute Severe Asthma in PediatricsDocument53 pagesManagement of Acute Severe Asthma in PediatricsAmit AnandNo ratings yet
- Drug StudyDocument5 pagesDrug Studyboxed juiceNo ratings yet
- Top 5 Corticosteroids For Use in Emergency SettingsDocument4 pagesTop 5 Corticosteroids For Use in Emergency SettingsIulian Cătălin GrămadăNo ratings yet
- An Approach To Treating Long COVID: First Line TherapiesDocument3 pagesAn Approach To Treating Long COVID: First Line TherapiesflorentinaNo ratings yet
- Summary Antimicrobial Prescribing Guidance - July 21 For BNFDocument31 pagesSummary Antimicrobial Prescribing Guidance - July 21 For BNFbarcanbiancaNo ratings yet
- Drug Study23Document2 pagesDrug Study23Joh Acedo BantingNo ratings yet
- Directorate of Tourism, Govt. of Maharashtra: Mous Signed With Iprcl and MCDCDocument2 pagesDirectorate of Tourism, Govt. of Maharashtra: Mous Signed With Iprcl and MCDCNaina DesaiNo ratings yet
- News Letter World Tourism DayDocument1 pageNews Letter World Tourism DayNaina DesaiNo ratings yet
- Bombay High Court building opens for heritage walksDocument2 pagesBombay High Court building opens for heritage walksNaina DesaiNo ratings yet
- Press Note On New Adventure Tourism Policy Gets ApprovalDocument2 pagesPress Note On New Adventure Tourism Policy Gets ApprovalNaina DesaiNo ratings yet
- Press Note - Agri Tourism Traininge - EnglishDocument3 pagesPress Note - Agri Tourism Traininge - EnglishNaina DesaiNo ratings yet
- Format For Vendor/Service Provider Details (On Letter Head of Vendor Only)Document1 pageFormat For Vendor/Service Provider Details (On Letter Head of Vendor Only)Naina DesaiNo ratings yet
- Form GST REG-25: Government of India and Government of GujaratDocument1 pageForm GST REG-25: Government of India and Government of GujaratNaina DesaiNo ratings yet
- Vendor Code Vendor Name Vendor Code Vendor NameDocument2 pagesVendor Code Vendor Name Vendor Code Vendor NameNaina DesaiNo ratings yet
- COVID HOME CARE en 05012022Document1 pageCOVID HOME CARE en 05012022Deepak RanakotiNo ratings yet
- D) Ûfp G/P Z (B (0) T BFT (NFZ CF (JF V/U (GF (NFB, F (D (/JJF Afat: S, (S8Z SR (ZL4Document7 pagesD) Ûfp G/P Z (B (0) T BFT (NFZ CF (JF V/U (GF (NFB, F (D (/JJF Afat: S, (S8Z SR (ZL4Naina DesaiNo ratings yet
- Case ReportDocument14 pagesCase ReportJalalludin AnNo ratings yet
- Right-Sided Heart Failure: College of NursingDocument30 pagesRight-Sided Heart Failure: College of NursingMatelyn OargaNo ratings yet
- Mater PIR - Dr. Siti Chandra W., SP - KFR-K High Intensity Laser For Post COVID RehabilitationDocument20 pagesMater PIR - Dr. Siti Chandra W., SP - KFR-K High Intensity Laser For Post COVID RehabilitationGhea Putri HendrianiNo ratings yet
- Husel Lawsuit Against Mount Carmel-Trinity 12.26.19Document52 pagesHusel Lawsuit Against Mount Carmel-Trinity 12.26.19WOSUNo ratings yet
- P1 P2 Mastery Examination Reviewer in FNP LECTUREDocument34 pagesP1 P2 Mastery Examination Reviewer in FNP LECTUREMary Ann G. CorsanesNo ratings yet
- Palliative CareDocument82 pagesPalliative Carejoycebrenda348No ratings yet
- RT Skills ChecklistDocument3 pagesRT Skills ChecklistMond SantosNo ratings yet
- Correct Answer: 4. Premedicate The Client With An Analgesic Before AmbulatingDocument49 pagesCorrect Answer: 4. Premedicate The Client With An Analgesic Before AmbulatingPortage ExamsNo ratings yet
- History of Present IllnessDocument7 pagesHistory of Present IllnessBena GichiaNo ratings yet
- Massachusetts General Hospital (MGH) COVID-19 Treatment GuidanceDocument24 pagesMassachusetts General Hospital (MGH) COVID-19 Treatment Guidancerajesh BNo ratings yet
- Modern Management of Cardiogenic Pulmonary Edema: Amal Mattu, MD, Joseph P. Martinez, MD, Brian S. Kelly, MDDocument21 pagesModern Management of Cardiogenic Pulmonary Edema: Amal Mattu, MD, Joseph P. Martinez, MD, Brian S. Kelly, MDJoni MokodoNo ratings yet
- Implanted Venous Access Device (IVAD) - "Dome" or "Port"Document12 pagesImplanted Venous Access Device (IVAD) - "Dome" or "Port"JunkNo ratings yet
- Heart Failure Nursing Care Management - A Study GuideDocument16 pagesHeart Failure Nursing Care Management - A Study GuideJOSHUA DICHOSONo ratings yet
- COVID-19 visitor screening logDocument1 pageCOVID-19 visitor screening logۦۦ ۦۦNo ratings yet
- FU-M2-CU6 LEC Planning Phase-Towards Goals and Outcomes.Document6 pagesFU-M2-CU6 LEC Planning Phase-Towards Goals and Outcomes.Shiro KagomeNo ratings yet
- 04 MSDS Catalyst (Vandium Penta Oxide)Document6 pages04 MSDS Catalyst (Vandium Penta Oxide)Furqan SiddiquiNo ratings yet
- CVD Diagnosis and Clinical ManifestationsDocument4 pagesCVD Diagnosis and Clinical ManifestationsIca JustitiaNo ratings yet
- Respiratory System: Haitham N.KhalidDocument71 pagesRespiratory System: Haitham N.KhalidJockerNo ratings yet