You might also like
- RxPrep 2020 Drug and Guideline UpdatesDocument5 pagesRxPrep 2020 Drug and Guideline Updatessyed100% (1)
- Dosing of Ivermectin & Other TherapeuticsDocument7 pagesDosing of Ivermectin & Other TherapeuticsTom100% (2)
- Recommended doses of Ivermectin for COVID-19 prevention and treatmentDocument3 pagesRecommended doses of Ivermectin for COVID-19 prevention and treatmentRonald LunasNo ratings yet
- FLCCC Ivermectin in The Prophylaxis and Treatment of COVID 19Document28 pagesFLCCC Ivermectin in The Prophylaxis and Treatment of COVID 19brunorepettoNo ratings yet
- Long Haul COVID-19 Recovery ProtocolDocument3 pagesLong Haul COVID-19 Recovery ProtocolSterr LiingNo ratings yet
- FLCCC Alliance's I RECOVER Management Protocol For Long Haul COVID 19 SyndromeDocument3 pagesFLCCC Alliance's I RECOVER Management Protocol For Long Haul COVID 19 SyndromeAlan N100% (1)
- Pharmaceutical Marketing: Marketing Strategy Alternative Strategic ThrustsDocument29 pagesPharmaceutical Marketing: Marketing Strategy Alternative Strategic Thrustspremoshin100% (4)
- Sylvia PlathDocument12 pagesSylvia Plathapi-534201968No ratings yet
- Long Covid - The Long Covid Book for Clinicians and Sufferers - Away from Despair and Towards UnderstandingFrom EverandLong Covid - The Long Covid Book for Clinicians and Sufferers - Away from Despair and Towards UnderstandingNo ratings yet
- India 2030 PDFDocument188 pagesIndia 2030 PDFGray HouserNo ratings yet
- DLP Eng3 - q3 Cot 2 Giving Possible Solutions To A ProblemDocument6 pagesDLP Eng3 - q3 Cot 2 Giving Possible Solutions To A ProblemNardita Castro100% (1)
- Drug Data: Doxycycline Mechanism of Action and Nursing ResponsibilitiesDocument2 pagesDrug Data: Doxycycline Mechanism of Action and Nursing ResponsibilitiesAMIN BARINo ratings yet
- I PREVENT Protection Protocol V1 June2022Document4 pagesI PREVENT Protection Protocol V1 June2022Hector CorralesNo ratings yet
- I PREVENT Protection Protocol V1 June2022Document4 pagesI PREVENT Protection Protocol V1 June2022yilongwei.comNo ratings yet
- I CARE Protocol SummaryDocument4 pagesI CARE Protocol SummaryServaas OostrikNo ratings yet
- A Guide To Early Treatment of COVID-19: First Line TherapiesDocument4 pagesA Guide To Early Treatment of COVID-19: First Line TherapiesHector CorralesNo ratings yet
- Long Haul COVID-19 ProtocolDocument3 pagesLong Haul COVID-19 ProtocolAizaz ul HaqNo ratings yet
- I PREVENT COVID FLU RSV SummaryDocument3 pagesI PREVENT COVID FLU RSV SummaryServaas OostrikNo ratings yet
- FLCCC - Alliance I RECOVER Protocol Post VaccineDocument3 pagesFLCCC - Alliance I RECOVER Protocol Post VaccineWallfayerNo ratings yet
- FLCCC - Alliance I RECOVER Protocol PostVaccine v3 EnglishDocument3 pagesFLCCC - Alliance I RECOVER Protocol PostVaccine v3 EnglishLuciana Castilho QuinetNo ratings yet
- FLCCC Alliance MATHplus Protocol ENGLISHDocument3 pagesFLCCC Alliance MATHplus Protocol ENGLISHfernandohNo ratings yet
- FLCCC Alliance MATHplus Protocol ENGLISHDocument3 pagesFLCCC Alliance MATHplus Protocol ENGLISHJhonn BlackNo ratings yet
- MX Protocol Book FinalDocument42 pagesMX Protocol Book FinalPawan ChoudharyNo ratings yet
- FLCCC Alliance MATHplus Protocol ENGLISHDocument3 pagesFLCCC Alliance MATHplus Protocol ENGLISHDavid GrayNo ratings yet
- COVID & SARS - MATH+ Protocol W IvermectinDocument47 pagesCOVID & SARS - MATH+ Protocol W IvermectinisBubbaNo ratings yet
- FLCCC Ivermectin in The Prophylaxis and Treatment of COVID 19Document22 pagesFLCCC Ivermectin in The Prophylaxis and Treatment of COVID 19Juan Carlos Kuan HigueraNo ratings yet
- Summary Antimicrobial Prescribing Guidance - July 21 For BNFDocument31 pagesSummary Antimicrobial Prescribing Guidance - July 21 For BNFbarcanbiancaNo ratings yet
- FLCCC I MASS ProtocolDocument1 pageFLCCC I MASS Protocolnimrod20032003No ratings yet
- FLCCC Alliance I Maskplus Protocol EnglishDocument2 pagesFLCCC Alliance I Maskplus Protocol EnglishAlan NNo ratings yet
- Vaccinations Guideline Summary 2022Document4 pagesVaccinations Guideline Summary 2022Faisal PNo ratings yet
- GHC Lower Respiratory Tract Antimicrobial Guideline V 3 FinalDocument19 pagesGHC Lower Respiratory Tract Antimicrobial Guideline V 3 FinalNicthe Ruiz RodríguezNo ratings yet
- Query 1 Modified Systematic ApproachDocument3 pagesQuery 1 Modified Systematic ApproachAntoNo ratings yet
- PrednisoneDocument3 pagesPrednisoneShaira TanNo ratings yet
- Bedaquiline TB PDFDocument2 pagesBedaquiline TB PDFHana Fauzyyah HanifinNo ratings yet
- COVID-19 Protocol: Immune Boosting Protocol For Aiding Corona Viral Infection Prevention/RecoveryDocument4 pagesCOVID-19 Protocol: Immune Boosting Protocol For Aiding Corona Viral Infection Prevention/RecoverySabri MouradNo ratings yet
- UntitledDocument8 pagesUntitledDr. Jonathan CampilloNo ratings yet
- Short MDR Regimen Factsheet PDFDocument2 pagesShort MDR Regimen Factsheet PDFnasyiahNo ratings yet
- FLCCC Alliance I RECOVER Management Protocol For Long Haul COVID 19 SyndromeDocument4 pagesFLCCC Alliance I RECOVER Management Protocol For Long Haul COVID 19 SyndromeEric McKearneyNo ratings yet
- Buletin HS Bil3.2020Document14 pagesBuletin HS Bil3.2020Shaharaman ShariNo ratings yet
- Adult Patient Diagnosed With COVID-19: Ministry of Health & Family Welfare, Government of IndiaDocument1 pageAdult Patient Diagnosed With COVID-19: Ministry of Health & Family Welfare, Government of Indiapramodbankhele3845No ratings yet
- Management of Infection in Primary Care Adapted For Local UseDocument15 pagesManagement of Infection in Primary Care Adapted For Local UseWizri SuharianiNo ratings yet
- Prevention & Early Outpatient Treatment Protocol For Covid-19Document2 pagesPrevention & Early Outpatient Treatment Protocol For Covid-19mariaNo ratings yet
- COVID-19 Treatment Guidelines: Clinical ManagementDocument6 pagesCOVID-19 Treatment Guidelines: Clinical ManagementPetra SpringNo ratings yet
- COVID19 Management Algorithm 22042021 v1Document1 pageCOVID19 Management Algorithm 22042021 v1shivani shindeNo ratings yet
- COVID-19 PKPD Treatment VietnamDocument27 pagesCOVID-19 PKPD Treatment VietnamNhanLiNo ratings yet
- Drug StudyDocument5 pagesDrug StudyinjilbalazoNo ratings yet
- Methylprednisolone Drug Profile and Nursing ConsiderationsDocument4 pagesMethylprednisolone Drug Profile and Nursing ConsiderationsadryananestesiNo ratings yet
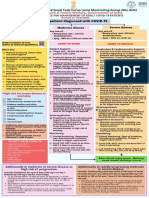
- National Task Force Clinical Guidance for Managing Adult COVID-19 PatientsDocument1 pageNational Task Force Clinical Guidance for Managing Adult COVID-19 PatientsWhiteNo ratings yet
- COVID Clinical Management 14012022Document1 pageCOVID Clinical Management 14012022Naina DesaiNo ratings yet
- I RECOVER Post Vaccine ProtocolDocument58 pagesI RECOVER Post Vaccine ProtocolJohnny SmithNo ratings yet
- Dudley Dementia Prescribing Guidance Final 1626174181Document9 pagesDudley Dementia Prescribing Guidance Final 1626174181Abdualaziz AlmalkiNo ratings yet
- FLCCC - Alliance I RECOVER Protocol PostVaccine v1 25may2022Document2 pagesFLCCC - Alliance I RECOVER Protocol PostVaccine v1 25may2022JohnNo ratings yet
- Drug Study23Document2 pagesDrug Study23Joh Acedo BantingNo ratings yet
- FRONT LINE COVID-19 CRITICAL CARE ALLIANCE PROTOCOLSDocument2 pagesFRONT LINE COVID-19 CRITICAL CARE ALLIANCE PROTOCOLSCornel ComanNo ratings yet
- New Drugs and Regimens for TB: 2015 UpdateDocument21 pagesNew Drugs and Regimens for TB: 2015 UpdateNop PiromNo ratings yet
- Pre Vaccination Screening FormDocument10 pagesPre Vaccination Screening Formbersabeh abayNo ratings yet
- What Is New in Management of Pediatric Tuberculosis ?Document8 pagesWhat Is New in Management of Pediatric Tuberculosis ?VijayyyNo ratings yet
- Im Butler Lecture - AsthmaDocument21 pagesIm Butler Lecture - Asthmaapi-602288180No ratings yet
- COVID Vaccination Side Effect Reducing OTC Medicines and NutraceuticalsDocument1 pageCOVID Vaccination Side Effect Reducing OTC Medicines and NutraceuticalsGlowstarNo ratings yet
- AIIMS issues new guidelines for treatment of Covid-19 casesDocument7 pagesAIIMS issues new guidelines for treatment of Covid-19 casessenthil kumarNo ratings yet
- AIIMS Issues New Guidelines For Treatment of CovidDocument7 pagesAIIMS Issues New Guidelines For Treatment of Covidsenthil kumarNo ratings yet
- Brajac - ProtocolDocument13 pagesBrajac - Protocolthanh ngôNo ratings yet
- FLCCC Alliance I Maskplus Protocol EnglishDocument2 pagesFLCCC Alliance I Maskplus Protocol EnglishThe BFDNo ratings yet
- CEMP-Framework Beach Project Scope Rev0Document152 pagesCEMP-Framework Beach Project Scope Rev0gowthamNo ratings yet
- Case Study Attendance Score DisputeDocument3 pagesCase Study Attendance Score DisputeSyed Aamir Ahmed0% (2)
- Noncompliance Unilateral Maxillary Molar DistalizationDocument6 pagesNoncompliance Unilateral Maxillary Molar Distalizationaa bbNo ratings yet
- Indian EthosDocument19 pagesIndian Ethosshahid veettil100% (2)
- Ethics in ResearchDocument29 pagesEthics in ResearchnationindiaNo ratings yet
- The Tamil Nadu Dr. M.G.R. Medical University, CHENNAI - 600 032Document18 pagesThe Tamil Nadu Dr. M.G.R. Medical University, CHENNAI - 600 032ArtemisNo ratings yet
- Pengumuman Jadwal Rapid Test Antigen Gratis Bagi Peserta Ujian SKB CPNS Pemerintah Kota Pangkalpinang 2021Document16 pagesPengumuman Jadwal Rapid Test Antigen Gratis Bagi Peserta Ujian SKB CPNS Pemerintah Kota Pangkalpinang 2021Syahrul SalehNo ratings yet
- CS 704 Socio-Emotional and Moral Development in Middle ChildhoodDocument25 pagesCS 704 Socio-Emotional and Moral Development in Middle ChildhoodPatricia PamintuanNo ratings yet
- Zimmer Cemented CPTDocument20 pagesZimmer Cemented CPTJayjeet BhoiteNo ratings yet
- CareGroup Case Study QuestionsDocument1 pageCareGroup Case Study QuestionsEnrica Melissa PanjaitanNo ratings yet
- LAC 2-OUTPUT On LDM2Document10 pagesLAC 2-OUTPUT On LDM2NaruffRalliburNo ratings yet
- Reading 3Document3 pagesReading 3Astri R SitumorangNo ratings yet
- Centric Relation Registration With Intraoral Central Bearing On Curved vs. Flat Plates With Rim Trays in Edentulous PatientsDocument8 pagesCentric Relation Registration With Intraoral Central Bearing On Curved vs. Flat Plates With Rim Trays in Edentulous PatientsCamila MuñozNo ratings yet
- Approach To Child With Headache: Dr. Vijaya Kumar Chikanbanjar 2nd Year Resident Department of PediatricsDocument49 pagesApproach To Child With Headache: Dr. Vijaya Kumar Chikanbanjar 2nd Year Resident Department of Pediatricsar bindraNo ratings yet
- Use Bloom's Taxonomy to Achieve Learning GoalsDocument61 pagesUse Bloom's Taxonomy to Achieve Learning GoalsSouvik DasNo ratings yet
- Lesson 1:: Introduction To Science, Technology and SocietyDocument17 pagesLesson 1:: Introduction To Science, Technology and SocietyAlexis A. AguilarNo ratings yet
- UPSC Prelims 2021 Geography Revision: High Probable Topics Part 2Document86 pagesUPSC Prelims 2021 Geography Revision: High Probable Topics Part 2PreethiNo ratings yet
- Vijaya Diagnostic HIV Test ReportDocument1 pageVijaya Diagnostic HIV Test Reportpasham bharat simha reddy100% (1)
- Ebook Conflict and Communication 1St Edition Jandt Test Bank Full Chapter PDFDocument27 pagesEbook Conflict and Communication 1St Edition Jandt Test Bank Full Chapter PDFgladysvanx3z100% (9)
- H.O.P.e - Module 1-The Role of Physical Activity Assessment in Managing One's StressDocument3 pagesH.O.P.e - Module 1-The Role of Physical Activity Assessment in Managing One's StressJoshua BaunNo ratings yet
- Time Magazine USA - December 22 2023Document98 pagesTime Magazine USA - December 22 2023paccs2006No ratings yet
- Tool Box Talk - MK - Emergency Response ProceduresDocument2 pagesTool Box Talk - MK - Emergency Response ProceduresPaul McGahanNo ratings yet
- The Corporation Reflection PaperDocument3 pagesThe Corporation Reflection PaperDevadutt M.SNo ratings yet
- Thesis Statement For Nickel and DimedDocument8 pagesThesis Statement For Nickel and Dimedafkntwbla100% (2)
- SR No. District Name Address Contact NoDocument3 pagesSR No. District Name Address Contact Nochirag sabhayaNo ratings yet
- Experienced Pharmacist Seeking New OpportunityDocument3 pagesExperienced Pharmacist Seeking New OpportunityIman ElshafieNo ratings yet