You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Reviewing Literature Learning Disability Fiction and The Social Work PerspectiveDocument13 pagesReviewing Literature Learning Disability Fiction and The Social Work Perspectiveauthor.avengingangelNo ratings yet
- DLP Eng3 - q3 Cot 2 Giving Possible Solutions To A ProblemDocument6 pagesDLP Eng3 - q3 Cot 2 Giving Possible Solutions To A ProblemNardita Castro100% (1)
- Breastfeeding Benefits and RecommendationsDocument46 pagesBreastfeeding Benefits and RecommendationsPriya bhattiNo ratings yet
- Hospital departments, medical terms, and anatomyDocument18 pagesHospital departments, medical terms, and anatomyThanh ToànNo ratings yet
- Sop Saad 3Document2 pagesSop Saad 3ZarmeenaGauharNo ratings yet
- Indian EthosDocument19 pagesIndian Ethosshahid veettil100% (2)
- Ethics in ResearchDocument29 pagesEthics in ResearchnationindiaNo ratings yet
- Thesis Statement For Nickel and DimedDocument8 pagesThesis Statement For Nickel and Dimedafkntwbla100% (2)
- Time Magazine USA - December 22 2023Document98 pagesTime Magazine USA - December 22 2023paccs2006No ratings yet
- Strengthening Mental Health and Psychosocial Support Systems and ServicesDocument116 pagesStrengthening Mental Health and Psychosocial Support Systems and ServicesPan PanNo ratings yet
- 175 Hys, Matuszek, Olejnik, BierczyńskiDocument9 pages175 Hys, Matuszek, Olejnik, BierczyńskiRadek PolonusNo ratings yet
- Meaning and Definition of Management DevelopmentDocument7 pagesMeaning and Definition of Management DevelopmentRiteshTirkey100% (2)
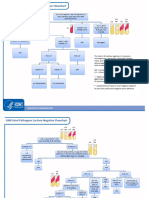
- GNR Stool Pathogens Lactose Negative FlowchartDocument2 pagesGNR Stool Pathogens Lactose Negative FlowchartKeithNo ratings yet
- Ey Work SampleDocument10 pagesEy Work SampleKris ANo ratings yet
- ACUTE KIDNEY INJURY SIGNS, SYMPTOMS, AND CAUSESDocument10 pagesACUTE KIDNEY INJURY SIGNS, SYMPTOMS, AND CAUSESYanti TandjungNo ratings yet
- The History of The Treatment of Maxillo-Facial TraumaDocument21 pagesThe History of The Treatment of Maxillo-Facial TraumaThanh NguyễnNo ratings yet
- قواعد التوثيق في البحوث والدراسات التربويةDocument19 pagesقواعد التوثيق في البحوث والدراسات التربويةnemra1No ratings yet
- Bilateral Congenitally Missing Second Premolars in A Growing Female PatientDocument5 pagesBilateral Congenitally Missing Second Premolars in A Growing Female PatientIJAR JOURNALNo ratings yet
- Sub-Adventitial Divestment Technique For Resecting Artery-Involved Pancreatic Cancer: A Retrospective Cohort StudyDocument11 pagesSub-Adventitial Divestment Technique For Resecting Artery-Involved Pancreatic Cancer: A Retrospective Cohort StudyMatias Jurado ChaconNo ratings yet
- Australian VSK 2018 LRDocument13 pagesAustralian VSK 2018 LRmuhamadrafie1975No ratings yet
- De-Escalation - Aggression Management TechniquesDocument14 pagesDe-Escalation - Aggression Management Techniquesparis emmaNo ratings yet
- Vale FormDocument1 pageVale FormRANDY BAOGBOGNo ratings yet
- Changing Light Bulbs SafelyDocument1 pageChanging Light Bulbs SafelyAshok Suresh100% (4)
- NEW - Hormone Balancing DrinkDocument9 pagesNEW - Hormone Balancing DrinkTAE'S POTATONo ratings yet
- Industrial Security Management SyllabusDocument7 pagesIndustrial Security Management SyllabusZefren Botilla100% (2)
- Vijaya Diagnostic HIV Test ReportDocument1 pageVijaya Diagnostic HIV Test Reportpasham bharat simha reddy100% (1)
- CHN Files Complete 1Document316 pagesCHN Files Complete 1ASTR4 BABYNo ratings yet
- CEMP-Framework Beach Project Scope Rev0Document152 pagesCEMP-Framework Beach Project Scope Rev0gowthamNo ratings yet
- Stiletto - Spring 2015Document24 pagesStiletto - Spring 2015TGI Justice ProjectNo ratings yet
- Silverstein L, Kurtzman G y Shatz P. (2009) Suturing For Optimal Soft Tissue Manament. Journal of Oral Implantology Vol. 35 (2), 82-90 PDFDocument9 pagesSilverstein L, Kurtzman G y Shatz P. (2009) Suturing For Optimal Soft Tissue Manament. Journal of Oral Implantology Vol. 35 (2), 82-90 PDFamilesco0% (1)