You might also like
- Naplex Complete Study Outline A Topic-Wise Approach DiabetesFrom EverandNaplex Complete Study Outline A Topic-Wise Approach DiabetesRating: 4 out of 5 stars4/5 (2)
- Fullsize SBAR Report SheetDocument1 pageFullsize SBAR Report SheetShane LambertNo ratings yet
- OB - Normal Labor and DeliveryDocument51 pagesOB - Normal Labor and DeliveryJosh Matthew Rosales33% (3)
- Case Presentation: - Vuppu BhavaniDocument53 pagesCase Presentation: - Vuppu BhavaniLohith Kumar MenchuNo ratings yet
- NLN Medication Exam Study Guide QuizletDocument36 pagesNLN Medication Exam Study Guide Quizletmaniz442No ratings yet
- Omeprazole 2018: Newborn Use OnlyDocument5 pagesOmeprazole 2018: Newborn Use OnlyHengky AntonNo ratings yet
- Manual of Definitive Surgical Trauma CareDocument256 pagesManual of Definitive Surgical Trauma Carebovine splendor100% (3)
- Module Answers 1 60 MCN 2Document151 pagesModule Answers 1 60 MCN 2bekbekk cabahug100% (6)
- Albuterol (Salbutamol)Document3 pagesAlbuterol (Salbutamol)Mae Ann Bueno CastillonNo ratings yet
- Nephrotic SyndromeDocument57 pagesNephrotic SyndromePradnya WartheNo ratings yet
- Acute Gastroenteritis FinalDocument40 pagesAcute Gastroenteritis FinalAlbertina Aipinge NandjilaNo ratings yet
- DM & DI ExamsDocument11 pagesDM & DI ExamsTomzki CornelioNo ratings yet
- Neprotic Syndrome PDFDocument30 pagesNeprotic Syndrome PDFAlana KuruvillaNo ratings yet
- Evaluation Entomological WarfareDocument62 pagesEvaluation Entomological WarfareReid Kirby100% (1)
- Roundworm Infections, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandRoundworm Infections, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Guideline For Management Protocol of Children With Fever and Respiratory SymptomsDocument44 pagesGuideline For Management Protocol of Children With Fever and Respiratory SymptomsKushagr GautamNo ratings yet
- Acute RhinosinusitisDocument39 pagesAcute RhinosinusitisHamoud AlshehriNo ratings yet
- Bronchial AsthmaDocument45 pagesBronchial Asthmaprincesszahra6498No ratings yet
- GE Problems 1st & 3rd Sept-2022Document7 pagesGE Problems 1st & 3rd Sept-2022Doctor iVJNo ratings yet
- COVID19 Management Algorithm 22042021 v1Document1 pageCOVID19 Management Algorithm 22042021 v1shivani shindeNo ratings yet
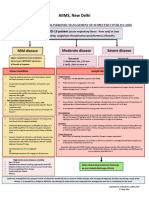
- AIIMS Issues New Guidelines For Treatment of CovidDocument7 pagesAIIMS Issues New Guidelines For Treatment of Covidsenthil kumarNo ratings yet
- TreatmentProtocol 10-4-2021Document3 pagesTreatmentProtocol 10-4-2021Anishk SinghNo ratings yet
- AIIMS Issues New Guidelines For Treatment of Covid-19 Cases: (Enter Post Title Here)Document7 pagesAIIMS Issues New Guidelines For Treatment of Covid-19 Cases: (Enter Post Title Here)senthil kumarNo ratings yet
- Covid-19 Management: FAQs by HCWsDocument31 pagesCovid-19 Management: FAQs by HCWsKabirNo ratings yet
- Guidelines For Management of COVID-19 in Children (Below 18 Years)Document10 pagesGuidelines For Management of COVID-19 in Children (Below 18 Years)Juhi NeogiNo ratings yet
- Query 1 Modified Systematic ApproachDocument3 pagesQuery 1 Modified Systematic ApproachAntoNo ratings yet
- Home Isolation For Covid Care FinalDocument9 pagesHome Isolation For Covid Care FinalAmy LalringhluaniNo ratings yet
- Treatment Protocol Covid-19Document4 pagesTreatment Protocol Covid-19Shiv singhNo ratings yet
- COVID-19 Protocol KGMU Version 6.0 17-4-21Document34 pagesCOVID-19 Protocol KGMU Version 6.0 17-4-21Kirtivaan MishraNo ratings yet
- Sindrom NefrotikDocument31 pagesSindrom NefrotikMohammed Ramzy GhifariNo ratings yet
- Aanp Practice Questions and AnswersDocument32 pagesAanp Practice Questions and Answersanahmburu966No ratings yet
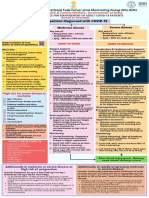
- AIIMS/ ICMR-COVID-19 National Task Force/ Joint Monitoring Group (Dte - GHS) Ministry of Health & Family Welfare, Government of IndiaDocument1 pageAIIMS/ ICMR-COVID-19 National Task Force/ Joint Monitoring Group (Dte - GHS) Ministry of Health & Family Welfare, Government of IndiaSomnath Das GuptaNo ratings yet
- Adult Patient Diagnosed With COVID-19: Ministry of Health & Family Welfare, Government of IndiaDocument1 pageAdult Patient Diagnosed With COVID-19: Ministry of Health & Family Welfare, Government of Indiapramodbankhele3845No ratings yet
- Acute Viral Syndrome: Case Presentation OnDocument22 pagesAcute Viral Syndrome: Case Presentation OnSafoora RafeeqNo ratings yet
- Monterozo, Ronel Von O. Prime 4Document7 pagesMonterozo, Ronel Von O. Prime 4Ronel MonterozoNo ratings yet
- Basic and Advance Clinical Outpatient Management For Polillo RHUDocument122 pagesBasic and Advance Clinical Outpatient Management For Polillo RHUHamilton EscaraNo ratings yet
- Revised Guidelines For Homoeopathy Practitioners For Prophylaxis and Symptomatic Management of COVID-19 Patients in Home IsolationDocument6 pagesRevised Guidelines For Homoeopathy Practitioners For Prophylaxis and Symptomatic Management of COVID-19 Patients in Home IsolationBABUNo ratings yet
- Clinical Management Protocol PDFDocument7 pagesClinical Management Protocol PDFAJEET KUMAR PANDEYNo ratings yet
- Case Based Learning Antimicrobials 05-12-2023Document50 pagesCase Based Learning Antimicrobials 05-12-2023aditya.3757No ratings yet
- Hiv & Aids-Related Drugs: Pharma - Semis GutierrezDocument3 pagesHiv & Aids-Related Drugs: Pharma - Semis GutierrezYsabelle GutierrezNo ratings yet
- Covid-19 Management ProtocolDocument27 pagesCovid-19 Management ProtocolGovindNo ratings yet
- Pharma NotesDocument5 pagesPharma Noteschauncey tuazonNo ratings yet
- Management Guidelines For Short Febrile Illness Including ILIDocument6 pagesManagement Guidelines For Short Febrile Illness Including ILIVenkata Nagaraj MummadisettyNo ratings yet
- Swine Flu Swine Flu: Ministry of Health and Family Welfare Government of IndiaDocument19 pagesSwine Flu Swine Flu: Ministry of Health and Family Welfare Government of IndiagirismgNo ratings yet
- Typhoid Fever: by DR .. Magdi Elbaloola Ahmed Physcian & GastrohepatologistDocument25 pagesTyphoid Fever: by DR .. Magdi Elbaloola Ahmed Physcian & GastrohepatologistÅbübâkêř Äbd-ëřhēēm BãřřîNo ratings yet
- Lascano, Joanne Alyssa H. - Parasitology SGDDocument8 pagesLascano, Joanne Alyssa H. - Parasitology SGDJoanne Alyssa Hernandez LascanoNo ratings yet
- Caz ClinicDocument15 pagesCaz ClinicAlina Maria DucaNo ratings yet
- AIIMS Syndromic ApproachDocument1 pageAIIMS Syndromic ApproachRagul VNo ratings yet
- COVID - Management 14 April 2021Document20 pagesCOVID - Management 14 April 2021Zain ZaidiNo ratings yet
- BUDESONIDEDocument3 pagesBUDESONIDEshiraz.aNo ratings yet
- SCENARIO: at 8:30am, Mrs. Cercan Come in at The Unit With Her Husband. They Are Bringing The ReferralDocument3 pagesSCENARIO: at 8:30am, Mrs. Cercan Come in at The Unit With Her Husband. They Are Bringing The ReferralDinarkram Rabreca EculNo ratings yet
- Leptospirosis: Pauline Teo Siew ChinDocument18 pagesLeptospirosis: Pauline Teo Siew Chinfarmasi_hmNo ratings yet
- Clinical Management Protocol and Infection Control GuidelinesDocument16 pagesClinical Management Protocol and Infection Control Guidelinesalfaz lakhaniNo ratings yet
- MIS C Algorithim Version 2Document8 pagesMIS C Algorithim Version 2Saima UmairNo ratings yet
- Museum IDocument37 pagesMuseum ISirish KunwarNo ratings yet
- MethylprednisoloneDocument4 pagesMethylprednisoloneadryananestesiNo ratings yet
- NP1 BulletsDocument17 pagesNP1 BulletsJea VesagasNo ratings yet
- NP1 BulletsDocument17 pagesNP1 BulletsJea VesagasNo ratings yet
- Session 4-Management of Paediatric COVID19Document24 pagesSession 4-Management of Paediatric COVID19Uncertain NeuronNo ratings yet
- Child With Fever in ER Non Covid 19Document6 pagesChild With Fever in ER Non Covid 19Suwandi AlghozyNo ratings yet
- Erythromycin & Pneumococcal VaccineDocument6 pagesErythromycin & Pneumococcal VaccineNikki Joy NavarroNo ratings yet
- International Journal of Nursing and Health Research: Management of Traveler's Diarrhea: Short ReviewDocument2 pagesInternational Journal of Nursing and Health Research: Management of Traveler's Diarrhea: Short ReviewAri PutraNo ratings yet
- Dengue-Who Treatment ProtocolsDocument39 pagesDengue-Who Treatment ProtocolsushapadminivadivelswamyNo ratings yet
- Teachng DemoDocument32 pagesTeachng DemoNom NomNo ratings yet
- My Experiments With Corona - Revised Edition April, 2021Document35 pagesMy Experiments With Corona - Revised Edition April, 2021Vijay ShankarNo ratings yet
- COVID Management 17th January 2022 DR Suvrankar Datta AIIMSDocument1 pageCOVID Management 17th January 2022 DR Suvrankar Datta AIIMSWhiteNo ratings yet
- Health Advice and Immunizations for TravelersFrom EverandHealth Advice and Immunizations for TravelersNo ratings yet
- 50 Years of Neonatology in India Progress and FutureDocument3 pages50 Years of Neonatology in India Progress and FutureSutirtha RoyNo ratings yet
- 2022 NMC DM NeonatologyDocument30 pages2022 NMC DM NeonatologySutirtha RoyNo ratings yet
- Juan DiceDocument12 pagesJuan DiceSutirtha RoyNo ratings yet
- Jaundice (Summary)Document7 pagesJaundice (Summary)Sutirtha RoyNo ratings yet
- Carnatic and Hindustani RaagasDocument5 pagesCarnatic and Hindustani RaagasSutirtha RoyNo ratings yet
- Tempo MarkingsDocument1 pageTempo MarkingsSutirtha RoyNo ratings yet
- Does The Universe Have A PurposeDocument17 pagesDoes The Universe Have A PurposejaquesbloodhoundNo ratings yet
- Effect of Periodontal Therapy On C-Reactive Protein Levels in Gingival Crevicular Fluid of Patients With Gingivitis and Chronic PeriodontitisDocument5 pagesEffect of Periodontal Therapy On C-Reactive Protein Levels in Gingival Crevicular Fluid of Patients With Gingivitis and Chronic PeriodontitisKanagavalli VijayakumarNo ratings yet
- PHARM 315: Cheza May Baldado BS Pharm IIIDocument12 pagesPHARM 315: Cheza May Baldado BS Pharm IIIKathleen B BaldadoNo ratings yet
- Antenatal Care Services: by DR - Chinedu Ibeh Thursday, 16 APRIL 2015Document81 pagesAntenatal Care Services: by DR - Chinedu Ibeh Thursday, 16 APRIL 2015SehaRizaNo ratings yet
- FibromaDocument3 pagesFibromaAsiyath HNo ratings yet
- C-Reactive Protein: TurbilatexDocument1 pageC-Reactive Protein: TurbilatexAssane Senghor100% (1)
- Team Approach With Diabetes Patients: HistoryDocument5 pagesTeam Approach With Diabetes Patients: HistoryEdgar SchultzNo ratings yet
- Canine Influenza FactsDocument5 pagesCanine Influenza FactsWIS Digital News StaffNo ratings yet
- Immature GranulocytesDocument10 pagesImmature Granulocytespieterinpretoria391No ratings yet
- Sas 39Document2 pagesSas 39Sistine Rose LabajoNo ratings yet
- Drugs For Diarrhea and ConstipationDocument24 pagesDrugs For Diarrhea and ConstipationFaddi BoyNo ratings yet
- Intramedullary Spinal Cord Tumors: Part II - Management Options and OutcomesDocument10 pagesIntramedullary Spinal Cord Tumors: Part II - Management Options and OutcomeszixzaxoffNo ratings yet
- Pertussis - Not Just For Kids: Clinical PracticeDocument8 pagesPertussis - Not Just For Kids: Clinical PracticeMihaela-Alexandra PopNo ratings yet
- Concept PaperDocument12 pagesConcept Paperjlventigan100% (1)
- Week 3 Acute TracheobronchitisDocument2 pagesWeek 3 Acute TracheobronchitisLu BeibeiNo ratings yet
- Course in The WardDocument7 pagesCourse in The WardDanicaEdonFelarcaNo ratings yet
- General DeclarationDocument1 pageGeneral DeclarationPos SMB IINo ratings yet
- Papanicolaou StainDocument1 pagePapanicolaou StainRitam JoarderNo ratings yet
- Hematology Unit: Complete Blood Count (CBC)Document2 pagesHematology Unit: Complete Blood Count (CBC)Rasha ElbannaNo ratings yet
- Topical Finasteride Consent Form April 2017Document6 pagesTopical Finasteride Consent Form April 2017Krsmanovic ZoranNo ratings yet
- Standard Operating Procedure (Biochemistry - Diasys RESPONS - 910)Document17 pagesStandard Operating Procedure (Biochemistry - Diasys RESPONS - 910)Aniruddha ChatterjeeNo ratings yet
- Family Medicine Timeline 1Document6 pagesFamily Medicine Timeline 1api-259973261No ratings yet
- 16 Fluid Electrolytes and Acid-Base ImbalancesDocument29 pages16 Fluid Electrolytes and Acid-Base ImbalancesBea Bianca CruzNo ratings yet
- Soal SBMPTN - B. INGGRISDocument4 pagesSoal SBMPTN - B. INGGRISMarva Sadira SuksmoputriNo ratings yet