You might also like
- Sports Cardiology: Care of the Athletic Heart from the Clinic to the SidelinesFrom EverandSports Cardiology: Care of the Athletic Heart from the Clinic to the SidelinesDavid J. EngelNo ratings yet
- Exercise Physiology for the Pediatric and Congenital CardiologistFrom EverandExercise Physiology for the Pediatric and Congenital CardiologistNo ratings yet
- Jurnal CardioDocument10 pagesJurnal CardiohengkileonardNo ratings yet
- European Journal of Preventive Cardiology-2016-Groehs-2047487316654025Document11 pagesEuropean Journal of Preventive Cardiology-2016-Groehs-2047487316654025Michelly MachadoNo ratings yet
- 3086 FullDocument10 pages3086 FullMaulida PuspitasariNo ratings yet
- Articulo TidierDocument7 pagesArticulo TidierNúria EsponaNo ratings yet
- The Effects of Baduanjin Exercise On Fatigue and Quality of Life in Patients With Heart Failure A Randomized Controlled TrialDocument11 pagesThe Effects of Baduanjin Exercise On Fatigue and Quality of Life in Patients With Heart Failure A Randomized Controlled Trial동생옹녤No ratings yet
- Effect of Acupressure On Physiological and Psychological Maladies Among Peri and Post Menopausal WomenDocument6 pagesEffect of Acupressure On Physiological and Psychological Maladies Among Peri and Post Menopausal WomenInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Fsurg 09 851113Document7 pagesFsurg 09 851113Cuide e se CuideNo ratings yet
- Ogmundsdottiretal EJPCPerfect CR2019Document11 pagesOgmundsdottiretal EJPCPerfect CR2019Faheem ullahNo ratings yet
- Suprascapular Nerve Block For Shoulder Pain in The First Year After StrokeDocument10 pagesSuprascapular Nerve Block For Shoulder Pain in The First Year After StrokeDiego Pinto PatroniNo ratings yet
- The Effect of Physical Training in Chronic Heart FailureDocument5 pagesThe Effect of Physical Training in Chronic Heart FailureDitaris GINo ratings yet
- Effects of Acupuncture StimulationDocument13 pagesEffects of Acupuncture StimulationtibaNo ratings yet
- Coronary Heart DiseaseDocument10 pagesCoronary Heart DiseaseMauludin BilaleyaNo ratings yet
- Belardi Nell I 1999Document11 pagesBelardi Nell I 1999LidiyahNo ratings yet
- Association of Six Minute Push Test Distance And.1197Document1 pageAssociation of Six Minute Push Test Distance And.1197Santi RopNo ratings yet
- JR AMI and Rehab CardiovascularDocument17 pagesJR AMI and Rehab CardiovascularFandy Hazzy AlfataNo ratings yet
- Pre-Hospital Management of Patients With Chest Pain And/ or Dyspnoea of Cardiac Origin. A Position Paper of The Acute Cardiovascular Care Association (ACCA) of The ESCDocument23 pagesPre-Hospital Management of Patients With Chest Pain And/ or Dyspnoea of Cardiac Origin. A Position Paper of The Acute Cardiovascular Care Association (ACCA) of The ESCReniNo ratings yet
- Cardiac Rehabilitation ThesisDocument5 pagesCardiac Rehabilitation ThesisScott Donald100% (1)
- Effects of Aromatherapy Acupressure On Hemiplegic Shoulder Pain and Motor Power in Stroke Patients: A Pilot StudyDocument6 pagesEffects of Aromatherapy Acupressure On Hemiplegic Shoulder Pain and Motor Power in Stroke Patients: A Pilot StudyAnggelia jopa sariNo ratings yet
- Cardiac RehabilitationDocument19 pagesCardiac RehabilitationAstrid Karina PutriNo ratings yet
- Acupuncture For Balance Dysfunction in Patients With StrokeDocument5 pagesAcupuncture For Balance Dysfunction in Patients With StrokeTinnitus Man IndonesiaNo ratings yet
- Letter To The Editor Hydrotherapy in Heart Failure: A Case: BackgroundDocument4 pagesLetter To The Editor Hydrotherapy in Heart Failure: A Case: BackgroundElizabete MonteiroNo ratings yet
- Ejercicio IntervalosDocument7 pagesEjercicio IntervalosOmar DVNo ratings yet
- Dimensi Dan IndikatorDocument9 pagesDimensi Dan IndikatorAndreas Leonardo T SimanjuntakNo ratings yet
- Artículo Intervención II.Document10 pagesArtículo Intervención II.Sofia Jimenez GilNo ratings yet
- CADthe BenefitofexerciseDocument5 pagesCADthe BenefitofexerciseDIMAS PRASETYONo ratings yet
- Dziubek 2016Document13 pagesDziubek 2016pangaribuansantaNo ratings yet
- PaolucciDocument379 pagesPaoluccijuanNo ratings yet
- 1 Ijpotdec20171Document8 pages1 Ijpotdec20171TJPRC PublicationsNo ratings yet
- Comparison of Electroacupuncture and Body Acupuncture On Gastrocnemius Muscle Tone in Children With Spastic Cerebral Palsy: A Single Blinded, Randomized Controlled Pilot TrialDocument6 pagesComparison of Electroacupuncture and Body Acupuncture On Gastrocnemius Muscle Tone in Children With Spastic Cerebral Palsy: A Single Blinded, Randomized Controlled Pilot TrialrezteevicNo ratings yet
- PNF 5 Effect of PNF On Standing Ballance Control Among Post StrokeDocument5 pagesPNF 5 Effect of PNF On Standing Ballance Control Among Post StrokeAnonymous j0xAgHs3No ratings yet
- Pone 0159966Document16 pagesPone 0159966JESICA PAOLA RODRIGUEZ PEREZNo ratings yet
- The Egyptian Heart Journal: Ahmed Elshazly, Hazem Khorshid, Hany Hanna, Ammar AliDocument3 pagesThe Egyptian Heart Journal: Ahmed Elshazly, Hazem Khorshid, Hany Hanna, Ammar AliImran TarmiziNo ratings yet
- Sudarshan Kriya Yoga Mejora El Control Autonómico Cardíaco en Pacientes Con Trastornos de Ansiedad-DepresiónDocument7 pagesSudarshan Kriya Yoga Mejora El Control Autonómico Cardíaco en Pacientes Con Trastornos de Ansiedad-DepresiónPablo Ignacio González GálvezNo ratings yet
- Exercise - 22 - C - MedicineDocument18 pagesExercise - 22 - C - MedicinemaryNo ratings yet
- Scalp Acupuncture2Document64 pagesScalp Acupuncture2Ganga Singh100% (1)
- Pending 1666841661 DownloadDocument8 pagesPending 1666841661 Downloadmilena martinsNo ratings yet
- Suppl55 PDFDocument310 pagesSuppl55 PDFUbaidillah Romadlon AlfairuziNo ratings yet
- NeuroDocument4 pagesNeuroFrancisca Aravena RiquelmeNo ratings yet
- Cardiac Rehabilitation: Interventions and Outcomes 631: ROC Curve For The Cut-Off Value of 6MWDDocument1 pageCardiac Rehabilitation: Interventions and Outcomes 631: ROC Curve For The Cut-Off Value of 6MWDKings AndrewNo ratings yet
- Stroke PreventionDocument10 pagesStroke PreventionPetar ČolakNo ratings yet
- 1 s2.0 S1836955322001163 MainDocument2 pages1 s2.0 S1836955322001163 MainIhuoma AnaghaNo ratings yet
- Rop 3Document4 pagesRop 3Andi SusantoNo ratings yet
- Different Types of Resistance Training in Type 2 Diabetes Mellitus: Effects On Glycaemic Control, Muscle Mass and StrengthDocument10 pagesDifferent Types of Resistance Training in Type 2 Diabetes Mellitus: Effects On Glycaemic Control, Muscle Mass and StrengthMumtaz Maulana HidayatNo ratings yet
- HF AnsietasDocument5 pagesHF AnsietasFairuzarsyadNo ratings yet
- Bahan Inc TranslateDocument8 pagesBahan Inc TranslateDedi Irawandi Angela NursisNo ratings yet
- Pengaruh Mobilisasi DiniDocument22 pagesPengaruh Mobilisasi DiniJULIANINo ratings yet
- FCVM 09 788503Document7 pagesFCVM 09 788503angiebarNo ratings yet
- Effects of Progressive Resistance Training in Individuals With Type 2 Diabetic Polyneuropathy A Randomised Assessor-Blinded Controlled TrialDocument12 pagesEffects of Progressive Resistance Training in Individuals With Type 2 Diabetic Polyneuropathy A Randomised Assessor-Blinded Controlled TrialJesusNavarrete97No ratings yet
- Qin Et Al-2019-Physiological ReportsDocument14 pagesQin Et Al-2019-Physiological ReportsEndin Nokik StujannaNo ratings yet
- 6aum Etyw Q8XV 8xacDocument16 pages6aum Etyw Q8XV 8xaccah bagusNo ratings yet
- Arthroscopic Shoulder Surgery - 2011 - Journal of PhysiotherapyDocument1 pageArthroscopic Shoulder Surgery - 2011 - Journal of PhysiotherapyCông Tác Xã Hội PhòngNo ratings yet
- EurJPrevCardiol19BriefRecommendationsForParticipationInLeisureTimeOrCompetitiveSportsAthletesPtsWithCAD SportsCardiologySectionEuropeanAssociationOfPreventiveCardiology (EAPC)Document7 pagesEurJPrevCardiol19BriefRecommendationsForParticipationInLeisureTimeOrCompetitiveSportsAthletesPtsWithCAD SportsCardiologySectionEuropeanAssociationOfPreventiveCardiology (EAPC)Phitsanu SuntornpiyapanNo ratings yet
- 7452-Article Text-13296-1-10-20210611Document15 pages7452-Article Text-13296-1-10-20210611fitrianiNo ratings yet
- Exercise Improves Physical Function and Mental Health of Brain Cancer Survivors: Two Exploratory Case StudiesDocument7 pagesExercise Improves Physical Function and Mental Health of Brain Cancer Survivors: Two Exploratory Case StudiesWahdin AdinaNo ratings yet
- Acs 33 539Document3 pagesAcs 33 539MOVEMENT SCHOOLNo ratings yet
- Article: Ana P. Rossi, Debra D. Burris, F. Leslie Lucas, Gail A. Crocker, and James C. WassermanDocument8 pagesArticle: Ana P. Rossi, Debra D. Burris, F. Leslie Lucas, Gail A. Crocker, and James C. WassermandanielaNo ratings yet
- Ergometer Cycling Improves The Ambulatory Function and Cardiovascular Fitness of Stroke Patients-A Randomized Controlled TrialDocument6 pagesErgometer Cycling Improves The Ambulatory Function and Cardiovascular Fitness of Stroke Patients-A Randomized Controlled Trialayu lestariNo ratings yet
- Athlete’s Heart: A Multimodal Approach – From Physiological to Pathological Cardiac AdaptationsFrom EverandAthlete’s Heart: A Multimodal Approach – From Physiological to Pathological Cardiac AdaptationsNo ratings yet
- CLTIDocument8 pagesCLTIFandy Hazzy AlfataNo ratings yet
- Fluid Management Strategies in Heart Failure PDFDocument16 pagesFluid Management Strategies in Heart Failure PDFFandy Hazzy AlfataNo ratings yet
- Use Only: Cardiac Failure in - Thalassemia: Diagnosis, Prevention and ManagementDocument7 pagesUse Only: Cardiac Failure in - Thalassemia: Diagnosis, Prevention and ManagementFandy Hazzy AlfataNo ratings yet
- Garcia 2009Document7 pagesGarcia 2009Fandy Hazzy AlfataNo ratings yet
- Vip Rakas It 2018Document19 pagesVip Rakas It 2018Fandy Hazzy AlfataNo ratings yet
- The New Advanced Cardiac Life Support GuidelinesDocument52 pagesThe New Advanced Cardiac Life Support GuidelinesFandy Hazzy AlfataNo ratings yet
- Syncope Dr. Adrian RIzal PKB 2019Document39 pagesSyncope Dr. Adrian RIzal PKB 2019Fandy Hazzy AlfataNo ratings yet
- Acute Heart Failure: Fandy Hazzy AlfataDocument46 pagesAcute Heart Failure: Fandy Hazzy AlfataFandy Hazzy AlfataNo ratings yet
- HF 2012Document61 pagesHF 2012Fandy Hazzy AlfataNo ratings yet
- JR AMI and Rehab CardiovascularDocument17 pagesJR AMI and Rehab CardiovascularFandy Hazzy AlfataNo ratings yet
- 1 PDFDocument15 pages1 PDFFandy Hazzy AlfataNo ratings yet
- Carson LiberalvsRestrictiveTransfusionforSymptomaticCAD AmHeartJ 2013 PDFDocument9 pagesCarson LiberalvsRestrictiveTransfusionforSymptomaticCAD AmHeartJ 2013 PDFDio AlexanderNo ratings yet
- Clinical Standards For Heart Disease 2010Document59 pagesClinical Standards For Heart Disease 2010Novita Dwi MardiningtyasNo ratings yet
- Features of The Course of Cholecystocardial SyndromeDocument4 pagesFeatures of The Course of Cholecystocardial SyndromeCentral Asian StudiesNo ratings yet
- PNM 2018 358-360 PDFDocument3 pagesPNM 2018 358-360 PDFputriNo ratings yet
- CH02 Data Mining A Closer LookDocument34 pagesCH02 Data Mining A Closer LookÜmit BüyükduruNo ratings yet
- ABIM Quick Hits For MDsDocument7 pagesABIM Quick Hits For MDscinosure1100% (2)
- Oral Implantology Review A Study Guide, 2nd EditionDocument274 pagesOral Implantology Review A Study Guide, 2nd EditionThu Phuong NguyenNo ratings yet
- Doctor Away PDFDocument362 pagesDoctor Away PDFAnonymous 6OPLC9U100% (4)
- Swammy Plab 1 MockDocument32 pagesSwammy Plab 1 Mockfreelancer08No ratings yet
- OET 2.0 ReadingDocument202 pagesOET 2.0 ReadingCandy Benitez100% (1)
- 2015 To 2019 Super Speciality Dissertation Topics PDFDocument35 pages2015 To 2019 Super Speciality Dissertation Topics PDFJoseph John Crasto100% (4)
- Medif Information Sheet For Passengers Requiring Medical Clearence - Part 1-2 - Tarom From 4122 - 2Document2 pagesMedif Information Sheet For Passengers Requiring Medical Clearence - Part 1-2 - Tarom From 4122 - 2ViolleteMorenaNo ratings yet
- Chest Pain FinalDocument17 pagesChest Pain FinalVarun R'MenonNo ratings yet
- Cardiac Function Tests Anatomy of The HeartDocument8 pagesCardiac Function Tests Anatomy of The HeartJosiah BimabamNo ratings yet
- Case Scenario Week 15Document9 pagesCase Scenario Week 15karenbescaserNo ratings yet
- 6.6 CardiovascularDocument9 pages6.6 CardiovascularGhianx Carlox PioquintoxNo ratings yet
- Amazing DIY Breathing DeviceDocument60 pagesAmazing DIY Breathing DeviceArtour Rakhimov67% (9)
- Critical Care NoteDocument10 pagesCritical Care NoteHanis Rozib99% (69)
- Acute Coronary Syndrome, MI & ADHF-1Document28 pagesAcute Coronary Syndrome, MI & ADHF-1Hank WangNo ratings yet
- Module 4. Ebj. Pingul, MCDocument4 pagesModule 4. Ebj. Pingul, MCCharline PingulNo ratings yet
- Goodbye To Bypass SurgeryDocument6 pagesGoodbye To Bypass SurgeryrohitindiaNo ratings yet
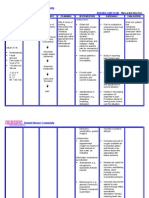
- Nursing Care Plan - Myocardial InfarctionDocument3 pagesNursing Care Plan - Myocardial Infarctionderic80% (10)
- Angina Pectoris: Dr. Naitik D Trivedi & Dr. Upama N. TrivediDocument15 pagesAngina Pectoris: Dr. Naitik D Trivedi & Dr. Upama N. TrivediNaveen KumarNo ratings yet
- Angina PectorisDocument24 pagesAngina PectorisDr AUNo ratings yet
- STEMIDocument29 pagesSTEMIHemanthNo ratings yet
- Working With Labor Laws (Samson&Young) Book Cases Compilation Chap 1 (Full Text)Document42 pagesWorking With Labor Laws (Samson&Young) Book Cases Compilation Chap 1 (Full Text)Yeppuda BarreraNo ratings yet
- NursingDocument30 pagesNursingWilmaBongotanPadawilNo ratings yet
- P.E and Health ReviewerrDocument14 pagesP.E and Health ReviewerrJoyce Anne Mae AdorioNo ratings yet
- Milta 4Document14 pagesMilta 4Victor RoticivNo ratings yet
- Resuscitation 1.1 Airway: ACEM Fellowship Exam Syllabus - Medical ExpertiseDocument27 pagesResuscitation 1.1 Airway: ACEM Fellowship Exam Syllabus - Medical ExpertiseAdeelZ.SiddiqiNo ratings yet