You might also like
- The Effect of Baby Massage Toward Baby Sleep Quantity On He Age of 3-6 Months in South Sempaja Sub-District, North Samarinda in 2019Document6 pagesThe Effect of Baby Massage Toward Baby Sleep Quantity On He Age of 3-6 Months in South Sempaja Sub-District, North Samarinda in 2019MbNo ratings yet
- Pediatric Massage Therapy Research: A Narrative ReviewDocument12 pagesPediatric Massage Therapy Research: A Narrative ReviewArturo Martí-CarvajalNo ratings yet
- 1 SMDocument12 pages1 SMMbNo ratings yet
- Resume LamarDocument1 pageResume LamarMbNo ratings yet
- Job Assignment Meeting Morning: YUSUF PRABA RAHMAN M10.01.0029Document1 pageJob Assignment Meeting Morning: YUSUF PRABA RAHMAN M10.01.0029MbNo ratings yet
- Release NotesDocument4 pagesRelease NotesDaniel Alexandru NyisztorNo ratings yet
- Hubungan Penurunan Fungsi Gerak Lansia Terhadap Strategi KopingDocument6 pagesHubungan Penurunan Fungsi Gerak Lansia Terhadap Strategi KopingMbNo ratings yet
- Speaking at Healthcare Meetings (Anatomy of The Presentation)Document3 pagesSpeaking at Healthcare Meetings (Anatomy of The Presentation)MbNo ratings yet
- TransGaming SwiftShader Whitepaper-20130129Document10 pagesTransGaming SwiftShader Whitepaper-20130129Tomz DwNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Review of Spiking Illness Syndrome of Broiler Chickens in Nepal 2008Document39 pagesReview of Spiking Illness Syndrome of Broiler Chickens in Nepal 2008Dr.Kedar Karki ,M.V.Sc.Preventive Vet.Medicine CLSU Philippines100% (1)
- Polio A Shot in The DarkDocument11 pagesPolio A Shot in The DarkJohnathanSteinNo ratings yet
- Impaired MemoryDocument1 pageImpaired MemoryHarmony Grace0% (1)
- UwomjDocument88 pagesUwomjjeffaguilarNo ratings yet
- Obtaining Electrocardiogram (Ecg) : Clinical Nursing SkillsDocument2 pagesObtaining Electrocardiogram (Ecg) : Clinical Nursing SkillsSwillight meNo ratings yet
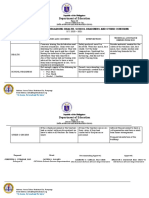
- Grade 5 - ISSUES-AND-CONCERNS-FOR-HEALTH-SCHOOL-READINESS-OTHER-CONCERNSDocument2 pagesGrade 5 - ISSUES-AND-CONCERNS-FOR-HEALTH-SCHOOL-READINESS-OTHER-CONCERNSDanny LineNo ratings yet
- Immediate Newborn Care Definition 23Document6 pagesImmediate Newborn Care Definition 23Courtney Dela FierraNo ratings yet
- Tooth Wear and AgingDocument5 pagesTooth Wear and AgingSARA TREJO GONZALEZNo ratings yet
- Can "Daniel's Diabetic Miracle" Naturally Heal Diabetes in As Little As 3 DaysDocument33 pagesCan "Daniel's Diabetic Miracle" Naturally Heal Diabetes in As Little As 3 Daysaz75% (4)
- Short Form Plan - August 2013Document3 pagesShort Form Plan - August 2013Anonymous s0QUn5CtHUNo ratings yet
- PATHO OB DystociaDocument14 pagesPATHO OB Dystociasailor MoonNo ratings yet
- Iñaki Gamborena 2020Document19 pagesIñaki Gamborena 2020Ulises DiazNo ratings yet
- Needle Stick InjuriesDocument1 pageNeedle Stick InjuriesAgnes BNo ratings yet
- Occupational Hazzards Affecting Healthcare ProffesionalsDocument17 pagesOccupational Hazzards Affecting Healthcare ProffesionalsMehnaz AbkrNo ratings yet
- Unit 10Document22 pagesUnit 10hafizur rahmanNo ratings yet
- Eye ImmunologyDocument35 pagesEye ImmunologySingo DemurNo ratings yet
- A Case of Aspartate Aminotransferase MacroenzymeDocument3 pagesA Case of Aspartate Aminotransferase MacroenzymeOlfiany Laurenzia PongohNo ratings yet
- R C N F A C T S H e e TDocument7 pagesR C N F A C T S H e e TScott MackenzieNo ratings yet
- 21.child With Diarrhea and Vomiting-SeminarDocument65 pages21.child With Diarrhea and Vomiting-SeminarRhomizal MazaliNo ratings yet
- Flabby Alveolar Ridges: A Modified Technique To Treat This Clinical ChallengeDocument4 pagesFlabby Alveolar Ridges: A Modified Technique To Treat This Clinical ChallengeammarkochiNo ratings yet
- Diabetes Advisor - A Medical Expert System For Diabetes ManagementDocument5 pagesDiabetes Advisor - A Medical Expert System For Diabetes ManagementPrincess LunieNo ratings yet
- Adedayo Osholowu VisualCV ResumeDocument5 pagesAdedayo Osholowu VisualCV ResumeAdedayo OsholowuNo ratings yet
- Baird 2017Document20 pagesBaird 2017Jhasmyn MartinezNo ratings yet
- Fitness & Wellness Industry in IndiaDocument12 pagesFitness & Wellness Industry in IndiaPrince SinghNo ratings yet
- Colloidal Silver Cures MRSA ReportDocument16 pagesColloidal Silver Cures MRSA ReportGodwinNo ratings yet
- Esposito Et Al-2014-Cochrane Database of Systematic Reviews PDFDocument93 pagesEsposito Et Al-2014-Cochrane Database of Systematic Reviews PDFTomNo ratings yet
- Nursing Care of A Child With Immune DisordersDocument4 pagesNursing Care of A Child With Immune DisordersChin T. OndongNo ratings yet
- PIA Press ReleaseDocument9 pagesPIA Press ReleaseShynne RPhNo ratings yet
- Monitoring Terapi Obat Dalam Pharmaceutical CareDocument55 pagesMonitoring Terapi Obat Dalam Pharmaceutical CareMaya ngoyemNo ratings yet
- Risk Management PlanDocument9 pagesRisk Management PlanCj Binalay Arao100% (2)