You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Adult History Taking and Physical ExaminationDocument6 pagesAdult History Taking and Physical ExaminationDoc Prince Caballero100% (1)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Nursing Practice Skills: Adult Intensive Care Unit PatientsDocument10 pagesNursing Practice Skills: Adult Intensive Care Unit PatientsMona Doria67% (3)
- Natural History of DiseaseDocument9 pagesNatural History of DiseaseAan Sucitra Hollan Fm'sNo ratings yet
- Children and Death: Dr. Chua 07/25/2013 Group 6 - Witwew!Document6 pagesChildren and Death: Dr. Chua 07/25/2013 Group 6 - Witwew!Doc Prince CaballeroNo ratings yet
- Is Schizophrenia Really Demonic PossessionDocument5 pagesIs Schizophrenia Really Demonic PossessionUproottNo ratings yet
- Grief, Mourning and BereavementDocument5 pagesGrief, Mourning and BereavementDoc Prince Caballero100% (1)
- San Antonio Elem. School: Contingency Plan ON Covid - 19Document12 pagesSan Antonio Elem. School: Contingency Plan ON Covid - 19Loraine Anna100% (2)
- Antepartum Fetal MonitoringDocument9 pagesAntepartum Fetal MonitoringDoc Prince CaballeroNo ratings yet
- Talk It Out Before You Say I DoDocument6 pagesTalk It Out Before You Say I DoDoc Prince CaballeroNo ratings yet
- Panunumpa NG Propesyonal PDFDocument2 pagesPanunumpa NG Propesyonal PDFAngelo Bonje100% (1)
- CPR With AedDocument37 pagesCPR With AedDoc Prince CaballeroNo ratings yet
- New Guidelines in Attendance Tracker SubmissionDocument1 pageNew Guidelines in Attendance Tracker SubmissionDoc Prince CaballeroNo ratings yet
- Bone Growth and Growth Pattern in ChildhoodDocument6 pagesBone Growth and Growth Pattern in ChildhoodDoc Prince CaballeroNo ratings yet
- The Midlife: Henrietta V. Cabado-Española, MD, FPPADocument7 pagesThe Midlife: Henrietta V. Cabado-Española, MD, FPPADoc Prince CaballeroNo ratings yet
- GI Disorders During Newborn PeriodDocument5 pagesGI Disorders During Newborn PeriodDoc Prince CaballeroNo ratings yet
- Medical Problems in AdolescentsDocument3 pagesMedical Problems in AdolescentsDoc Prince CaballeroNo ratings yet
- Principles of ImmunizationDocument4 pagesPrinciples of ImmunizationDoc Prince CaballeroNo ratings yet
- The Midlife: Henrietta V. Cabado-Española, MD, FPPADocument7 pagesThe Midlife: Henrietta V. Cabado-Española, MD, FPPADoc Prince CaballeroNo ratings yet
- GI Disorders During Newborn PeriodDocument5 pagesGI Disorders During Newborn PeriodDoc Prince CaballeroNo ratings yet
- NEONATAL RESUSCITATION GUIDELINESDocument5 pagesNEONATAL RESUSCITATION GUIDELINESDoc Prince CaballeroNo ratings yet
- Ballard Scoring: Component Description How To IllicitDocument4 pagesBallard Scoring: Component Description How To IllicitDoc Prince CaballeroNo ratings yet
- Current Status of The Filipino YouthDocument10 pagesCurrent Status of The Filipino YouthDoc Prince CaballeroNo ratings yet
- Early and Middle AdulthoodDocument6 pagesEarly and Middle AdulthoodDoc Prince CaballeroNo ratings yet
- Current Status of The Filipino YouthDocument10 pagesCurrent Status of The Filipino YouthDoc Prince CaballeroNo ratings yet
- Initial Care of Newborn & Newborn Screening Group 5 (Joy Marie Pillado's Conflicted Copy 2013-06-25)Document4 pagesInitial Care of Newborn & Newborn Screening Group 5 (Joy Marie Pillado's Conflicted Copy 2013-06-25)Doc Prince CaballeroNo ratings yet
- Surgical Problems in NewbornsDocument7 pagesSurgical Problems in NewbornsDoc Prince CaballeroNo ratings yet
- Breastfeeding BenefitsDocument4 pagesBreastfeeding BenefitsDoc Prince CaballeroNo ratings yet
- Aural Toilet Guideline1Document2 pagesAural Toilet Guideline1Ariska Peradilla100% (1)
- Systemic Response To InjuryDocument4 pagesSystemic Response To InjuryDoc Prince CaballeroNo ratings yet
- MenopauseDocument9 pagesMenopauseDoc Prince CaballeroNo ratings yet
- OB Tickler 1 PDFDocument22 pagesOB Tickler 1 PDFAnonymous de6SlW1No ratings yet
- Neonatal JaundiceDocument6 pagesNeonatal JaundiceDoc Prince CaballeroNo ratings yet
- Early Onset SchizophreniaDocument3 pagesEarly Onset SchizophreniaDoc Prince CaballeroNo ratings yet
- Pharmacology '' Routes of Administration #Local RouteDocument13 pagesPharmacology '' Routes of Administration #Local RouteNitin NawaleNo ratings yet
- Ethical Issues in NeonateDocument11 pagesEthical Issues in Neonatethilaga880% (1)
- The Key Role of The Dental Practitioner in Early Diagnosis of Periodontal Ehlers Danlos Syndromes A Rare Case Report of SiblingsDocument9 pagesThe Key Role of The Dental Practitioner in Early Diagnosis of Periodontal Ehlers Danlos Syndromes A Rare Case Report of SiblingsnadhiracindyNo ratings yet
- JT 4412/11 AUG/SIN-DPS Flight PlanDocument62 pagesJT 4412/11 AUG/SIN-DPS Flight PlanWahdhan HadiNo ratings yet
- Serious Fungal Infections in The Philippines: Original ArticleDocument5 pagesSerious Fungal Infections in The Philippines: Original ArticleAilen LagulaNo ratings yet
- Lumpy Skin DiseaseDocument99 pagesLumpy Skin DiseaseDaoud IssaNo ratings yet
- Cap 2019 04 01 PDFDocument58 pagesCap 2019 04 01 PDFRajeev PareekNo ratings yet
- DFM, Colombo, ProspectusDocument16 pagesDFM, Colombo, ProspectusMatin Ahmad Khan100% (1)
- Chest Tube InsertionDocument3 pagesChest Tube InsertionprofarmahNo ratings yet
- Hyperacusis: Major Research Questions: Background Epidemiology and Natural HistoryDocument6 pagesHyperacusis: Major Research Questions: Background Epidemiology and Natural HistoryFuninganaNo ratings yet
- Mount Carmel Medication Management Pocket GuideDocument2 pagesMount Carmel Medication Management Pocket GuideWOSU100% (1)
- NCM 112 - Rle Nursing Care Plan: To Have Baseline Data. Normal Values Indicate Adequate Tissue PerfusionDocument7 pagesNCM 112 - Rle Nursing Care Plan: To Have Baseline Data. Normal Values Indicate Adequate Tissue Perfusiontherese BNo ratings yet
- Involution and LochiaDocument2 pagesInvolution and Lochiaapi-316491996100% (1)
- Copptech: Successful Tests Against Sars-Cov-2Document2 pagesCopptech: Successful Tests Against Sars-Cov-2enologiacomNo ratings yet
- Cadi PDFDocument66 pagesCadi PDFpradeepsj ReddyNo ratings yet
- Sir ModelDocument5 pagesSir ModelJaehun JeongNo ratings yet
- Getting To The Roots of Failure: The Left May Be Down, But It Is Certainly Not Out. How May It Renew Itself?Document2 pagesGetting To The Roots of Failure: The Left May Be Down, But It Is Certainly Not Out. How May It Renew Itself?Priyank BhatiaNo ratings yet
- Terapi ToxoplasmosisDocument9 pagesTerapi Toxoplasmosissarah disaNo ratings yet
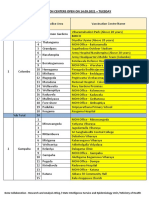
- Vaccination Centers On 14.09.2021Document8 pagesVaccination Centers On 14.09.2021Chanu On CTNo ratings yet
- Treatment Outcome and Factors Affecting Time To Recovery in Children With Severe Acute Malnutrition Treated at Outpatient Therapeutic Care ProgramDocument11 pagesTreatment Outcome and Factors Affecting Time To Recovery in Children With Severe Acute Malnutrition Treated at Outpatient Therapeutic Care ProgramMelkamuMeridNo ratings yet
- CFR - Code of Federal Regulations Title 21Document2 pagesCFR - Code of Federal Regulations Title 21Faradina Astari MunandarNo ratings yet
- Covid Vaccine Status Class MasandiganDocument4 pagesCovid Vaccine Status Class MasandiganServus DeiNo ratings yet
- Ceftriaxone Compared With Sodium Penicillin G For Treatment of Severe LeptospirosisDocument9 pagesCeftriaxone Compared With Sodium Penicillin G For Treatment of Severe LeptospirosisFifi SumarwatiNo ratings yet
- NURS FPX 6414 Assessment 3 Tool Kit for BioinformaticsDocument5 pagesNURS FPX 6414 Assessment 3 Tool Kit for BioinformaticsCarolyn HarkerNo ratings yet
- Evidence Based PostpartumDocument75 pagesEvidence Based PostpartumAnnisatus SholehahNo ratings yet
- C1 Editable Quiz 3 - 0Document3 pagesC1 Editable Quiz 3 - 0Hiền Vũ Thị MaiNo ratings yet