You might also like
- Damanik Indonesian Translation - Kuesioner DASS 42Document8 pagesDamanik Indonesian Translation - Kuesioner DASS 42Tisa Anindita Diandra Putri50% (2)
- The Crashing Ventilated Patient Algorthm (Jairo I. Santanilla, ACEP, 2011)Document1 pageThe Crashing Ventilated Patient Algorthm (Jairo I. Santanilla, ACEP, 2011)PkernNo ratings yet
- Aortic Valve Disease Guidelines PDFDocument36 pagesAortic Valve Disease Guidelines PDFStefan Marev GerganovNo ratings yet
- 2022 JAMA Diagnosis and Treatment of ACSDocument14 pages2022 JAMA Diagnosis and Treatment of ACSPeter Albeiro Falla Cortes100% (1)
- All You Need To Know About Clips: AckermannDocument9 pagesAll You Need To Know About Clips: AckermannjulzcatNo ratings yet
- 1 s2.0 S2405500X22010945Document14 pages1 s2.0 S2405500X22010945FideoPereNo ratings yet
- Major Global Coron Art Calcium CAC Guidel SOTA Golub JACC 2023Document20 pagesMajor Global Coron Art Calcium CAC Guidel SOTA Golub JACC 2023Percy DurandNo ratings yet
- J Jacc 2018 05 027Document14 pagesJ Jacc 2018 05 027totya91No ratings yet
- ACC/AHA Versus ESC Guidelines On Prosthetic Heart Valve ManagementDocument12 pagesACC/AHA Versus ESC Guidelines On Prosthetic Heart Valve ManagementKorejatNo ratings yet
- 2015 Article 52Document10 pages2015 Article 52Attilio Del RossoNo ratings yet
- Cathet Cardio Intervent - 2019 - Baran - SCAI Clinical Expert Consensus Statement On The Classification of CardiogenicDocument9 pagesCathet Cardio Intervent - 2019 - Baran - SCAI Clinical Expert Consensus Statement On The Classification of CardiogenicvaleriaNo ratings yet
- SincopeDocument14 pagesSincopeLuis GuerraNo ratings yet
- Strokeaha 115 003390 FullDocument15 pagesStrokeaha 115 003390 FullMartoiu MariaNo ratings yet
- Unstable Angina and Non-ST-Segment Elevation Myocardial InfarctionDocument8 pagesUnstable Angina and Non-ST-Segment Elevation Myocardial InfarctionRohaniNo ratings yet
- AHA/ACC Guidelines For Secondary Prevention For Patients With Coronary and Other Atherosclerotic Vascular Disease: 2006 UpdateDocument11 pagesAHA/ACC Guidelines For Secondary Prevention For Patients With Coronary and Other Atherosclerotic Vascular Disease: 2006 UpdategogmasiraitNo ratings yet
- CirculationahaDocument10 pagesCirculationahaTaufiqurrokhman RofiiNo ratings yet
- Echocardiographic Assessment of Valve Stenosis: EAE/ASE Recommendations For Clinical PracticeDocument23 pagesEchocardiographic Assessment of Valve Stenosis: EAE/ASE Recommendations For Clinical PracticeAurora CrawfordNo ratings yet
- Acute Aortic Syndrome RevisitedDocument20 pagesAcute Aortic Syndrome RevisitedVictor ChiabaiNo ratings yet
- Preoperative Cardiac Risk AssessmentDocument16 pagesPreoperative Cardiac Risk Assessmentkrysmelis MateoNo ratings yet
- Impact of Statins On Cardiovascular Outcomes Following Coronary Artery Calcium ScoringDocument10 pagesImpact of Statins On Cardiovascular Outcomes Following Coronary Artery Calcium ScoringJNo ratings yet
- Diagnosis of Acute Gout: A Clinical Practice Guideline From The American College of PhysiciansDocument8 pagesDiagnosis of Acute Gout: A Clinical Practice Guideline From The American College of PhysiciansRgm UyNo ratings yet
- Editorial: The 2019 Update of The European Abdominal Aortic Aneurysm GuidelinesDocument2 pagesEditorial: The 2019 Update of The European Abdominal Aortic Aneurysm GuidelinesNazliah SyarbinNo ratings yet
- J Jacadv 2022 100120Document14 pagesJ Jacadv 2022 100120Axel Hiram Hernandez PinedaNo ratings yet
- 2014 NSTE ACS Slide SetDocument109 pages2014 NSTE ACS Slide SetGiorgiana NicoletaNo ratings yet
- Osborn 2019Document7 pagesOsborn 2019Doctor's BettaNo ratings yet
- Analysis of Risk Factors For Different Subtypes of Acute Coronary SyndromeDocument12 pagesAnalysis of Risk Factors For Different Subtypes of Acute Coronary SyndromeAfrial ImamNo ratings yet
- Management of Atrial Fibrillation in 2021 An Updated Comparison of The Current CCS CHRS, ESC, and AHA ACC HRS GuidelinesDocument12 pagesManagement of Atrial Fibrillation in 2021 An Updated Comparison of The Current CCS CHRS, ESC, and AHA ACC HRS GuidelinessunhaolanNo ratings yet
- Current Endovascular Strategies For Cerebral Venous Thrombosis: Report of The SNIS Standards and Guidelines CommitteeDocument8 pagesCurrent Endovascular Strategies For Cerebral Venous Thrombosis: Report of The SNIS Standards and Guidelines CommitteeRafika Ayu NadiaNo ratings yet
- Identificacion Choque Cardiogenico ERDocument9 pagesIdentificacion Choque Cardiogenico ERZai RojasNo ratings yet
- J Jacadv 2022 100034Document14 pagesJ Jacadv 2022 100034Rui FonteNo ratings yet
- Standardized Team-Based Care For Cardiogenic Shock: BackgroundDocument11 pagesStandardized Team-Based Care For Cardiogenic Shock: BackgroundLucas MatheusNo ratings yet
- Inter Society Consensus For The Management of PAOD TASC II GuidelinesDocument70 pagesInter Society Consensus For The Management of PAOD TASC II GuidelinesPitoAdhiNo ratings yet
- 201 FullDocument14 pages201 FullMelita Aditya SariNo ratings yet
- 2021 ACR VF Guideline For Management of Giant Cell Arteritis and Takayasu ArtheritisDocument17 pages2021 ACR VF Guideline For Management of Giant Cell Arteritis and Takayasu Artheritisfatima amaliaNo ratings yet
- Subutilizacion de ACO en Adultos Mayores en EEUU-2022Document12 pagesSubutilizacion de ACO en Adultos Mayores en EEUU-2022Walter ReyesNo ratings yet
- Atualização de Síncope CCS 2020Document11 pagesAtualização de Síncope CCS 2020Carlos RenatoNo ratings yet
- Impacto de Prehabi en TAVIDocument10 pagesImpacto de Prehabi en TAVIPatricio DelgadilloNo ratings yet
- Indikasi TrombektomiDocument6 pagesIndikasi TrombektomiNatasha BastiaanNo ratings yet
- Iam 2022Document14 pagesIam 2022Mateo Daniel Gutierrez CastañedaNo ratings yet
- (23931817 - The Journal of Critical Care Medicine) The Diagnosis and Hemodynamic Monitoring of Circulatory Shock - Current and Future Trends-1Document9 pages(23931817 - The Journal of Critical Care Medicine) The Diagnosis and Hemodynamic Monitoring of Circulatory Shock - Current and Future Trends-1Kamal NasirNo ratings yet
- Comparacion SCORES de Gravedad de Choque CardiogenicoDocument7 pagesComparacion SCORES de Gravedad de Choque CardiogenicoAnandiBellotaNo ratings yet
- Probabilitate Pre-TestDocument3 pagesProbabilitate Pre-TestCorina NedelcuNo ratings yet
- J Annemergmed 2018 10 001Document3 pagesJ Annemergmed 2018 10 001dandinovtiardi20No ratings yet
- Jantung2 2014 VDocument9 pagesJantung2 2014 Vmuhammad zhafranNo ratings yet
- 2019 Atrial Fibrillation Type and Renal Dysfunction As Important Predictors of Left Atrial ThrombusDocument6 pages2019 Atrial Fibrillation Type and Renal Dysfunction As Important Predictors of Left Atrial ThrombusbernardoNo ratings yet
- Hypertension Arterielle 2016Document5 pagesHypertension Arterielle 2016Nabil YahioucheNo ratings yet
- ACC/AHA Versus ESC/ESH On Hypertension Guidelines: JACC Guideline ComparisonDocument9 pagesACC/AHA Versus ESC/ESH On Hypertension Guidelines: JACC Guideline ComparisonCamila ZorrillaNo ratings yet
- ASCO 2017 Prevention and Monitoring of Cardiac Dysfunction in Survivors of Adult CancersDocument21 pagesASCO 2017 Prevention and Monitoring of Cardiac Dysfunction in Survivors of Adult CancerslinxiaNo ratings yet
- Enfermedad Valvular CardiacaDocument10 pagesEnfermedad Valvular CardiacaBrayan HuayraNo ratings yet
- Jurnal PrognosisDocument9 pagesJurnal PrognosisNovita AfsariNo ratings yet
- Second Asymptomatic Carotid Surgery Trial (ACST-2) : A Randomised Comparison of Carotid Artery Stenting Versus Carotid EndarterectomyDocument9 pagesSecond Asymptomatic Carotid Surgery Trial (ACST-2) : A Randomised Comparison of Carotid Artery Stenting Versus Carotid EndarterectomySergio PalermoNo ratings yet
- Advances in The Management of Cardiogenic ShockDocument12 pagesAdvances in The Management of Cardiogenic ShockJoelGámezNo ratings yet
- Stirrup - Comparison of ESC and ACC:AHA Guidelines For Myocardial RevascularizationDocument8 pagesStirrup - Comparison of ESC and ACC:AHA Guidelines For Myocardial RevascularizationM. PurnomoNo ratings yet
- New England Journal Medicine: The ofDocument9 pagesNew England Journal Medicine: The ofHesbon MomanyiNo ratings yet
- Guideline Management Giant Cell Arteritis Takayasu Arteritis 2021Document17 pagesGuideline Management Giant Cell Arteritis Takayasu Arteritis 2021Jorge Álvarez GómezNo ratings yet
- Transfusion Reactions: Prevention, Diagnosis, and TreatmentDocument12 pagesTransfusion Reactions: Prevention, Diagnosis, and TreatmentAriNo ratings yet
- Acs 33 241Document9 pagesAcs 33 241Ratna AyieNo ratings yet
- 2021 ACR Guideline For Treatment Rheumatoid Arthritis Early ViewDocument16 pages2021 ACR Guideline For Treatment Rheumatoid Arthritis Early ViewCharles PinheiroNo ratings yet
- Assessment of Left Ventricular Function by EchocardiographyDocument15 pagesAssessment of Left Ventricular Function by EchocardiographyramangNo ratings yet
- Clinical Guideline: DescriptionDocument18 pagesClinical Guideline: DescriptionCamila Andrea Hernández HeinrichNo ratings yet
- 2015 Systematic Review of Guidelines For The ManagementDocument14 pages2015 Systematic Review of Guidelines For The ManagementGyörgy HalászNo ratings yet
- Clinical Handbook of Cardiac ElectrophysiologyFrom EverandClinical Handbook of Cardiac ElectrophysiologyBenedict M. GloverNo ratings yet
- Issn Faktor-Faktor Yang Berhubungan Dengan Perilaku Hidup Bersih Dan Sehat Sebagai Upaya Untuk Pencegahan Penyakit Diare Pada Siswa Di SDN PDFDocument8 pagesIssn Faktor-Faktor Yang Berhubungan Dengan Perilaku Hidup Bersih Dan Sehat Sebagai Upaya Untuk Pencegahan Penyakit Diare Pada Siswa Di SDN PDFVevi InakuNo ratings yet
- 4578 9988 1 SM PDFDocument11 pages4578 9988 1 SM PDFmike apriliaNo ratings yet
- Optimal Treatment of Patients With NSTE-ACS in The Dutch Health Care SystemDocument7 pagesOptimal Treatment of Patients With NSTE-ACS in The Dutch Health Care Systemmike apriliaNo ratings yet
- Pengaruh Penyuluhan Media Audio Visual Video Terhadap Perilaku Cuci Tangan Pakai Sabun Pada Siswa Kelas Iii Di SDN 027 SamarindaDocument9 pagesPengaruh Penyuluhan Media Audio Visual Video Terhadap Perilaku Cuci Tangan Pakai Sabun Pada Siswa Kelas Iii Di SDN 027 Samarindamike apriliaNo ratings yet
- Pengaruh Penyuluhan Media Audio Visual Video Terhadap Perilaku Cuci Tangan Pakai Sabun Pada Siswa Kelas Iii Di SDN 027 SamarindaDocument9 pagesPengaruh Penyuluhan Media Audio Visual Video Terhadap Perilaku Cuci Tangan Pakai Sabun Pada Siswa Kelas Iii Di SDN 027 Samarindamike apriliaNo ratings yet
- Budi Purwanti PDFDocument6 pagesBudi Purwanti PDFKuncung Pancal WernoNo ratings yet
- Prevalensi Indo PDFDocument8 pagesPrevalensi Indo PDFmike apriliaNo ratings yet
- Evaluasi Program Gerakan 21 Hari (G21H) Cuci Tangan Pakai Sabun Terhadap Perilaku Cuci Tangan Siswa Di SD Islam Al-Azhar 14 SemarangDocument8 pagesEvaluasi Program Gerakan 21 Hari (G21H) Cuci Tangan Pakai Sabun Terhadap Perilaku Cuci Tangan Siswa Di SD Islam Al-Azhar 14 SemarangLusita AdestiNo ratings yet
- Abu BakarDocument1 pageAbu Bakarmike apriliaNo ratings yet
- Abdul Wakhid PENERAPAN TERAPI LATIHAN KETRAMPILAN SOSIAL PADA KLIEN ISOL PDFDocument15 pagesAbdul Wakhid PENERAPAN TERAPI LATIHAN KETRAMPILAN SOSIAL PADA KLIEN ISOL PDFanang kurniawanNo ratings yet
- Evaluasi Program Gerakan 21 Hari (G21H) Cuci Tangan Pakai Sabun Terhadap Perilaku Cuci Tangan Siswa Di SD Islam Al-Azhar 14 SemarangDocument8 pagesEvaluasi Program Gerakan 21 Hari (G21H) Cuci Tangan Pakai Sabun Terhadap Perilaku Cuci Tangan Siswa Di SD Islam Al-Azhar 14 SemarangLusita AdestiNo ratings yet
- Menangani Stres Remaja Dengan Dukungan Sosial Teman Sebaya: December 2016Document10 pagesMenangani Stres Remaja Dengan Dukungan Sosial Teman Sebaya: December 2016mike apriliaNo ratings yet
- Faktor-Faktor Yang Berhubungan Dengan Praktik Sanitasi Melalui Perilaku Hidup Bersih Dan Sehat Pada Siswa Sekolah Dasar Di Kecamatan BanyumanikDocument6 pagesFaktor-Faktor Yang Berhubungan Dengan Praktik Sanitasi Melalui Perilaku Hidup Bersih Dan Sehat Pada Siswa Sekolah Dasar Di Kecamatan Banyumanikmike apriliaNo ratings yet
- Efektivitas Metode Peragaan Dan Metode Video PDFDocument7 pagesEfektivitas Metode Peragaan Dan Metode Video PDFMarianus BaniNo ratings yet
- Efektivitas Metode Peragaan Dan Metode Video PDFDocument7 pagesEfektivitas Metode Peragaan Dan Metode Video PDFMarianus BaniNo ratings yet
- ST-elevation Infark Miocard STEMIDocument2 pagesST-elevation Infark Miocard STEMImike apriliaNo ratings yet
- Abdul Wakhid PENERAPAN TERAPI LATIHAN KETRAMPILAN SOSIAL PADA KLIEN ISOL PDFDocument15 pagesAbdul Wakhid PENERAPAN TERAPI LATIHAN KETRAMPILAN SOSIAL PADA KLIEN ISOL PDFanang kurniawanNo ratings yet
- Aspikom PenyuluhDocument16 pagesAspikom PenyuluhWicaksono DamarNo ratings yet
- Press: Understanding Body ImagesDocument9 pagesPress: Understanding Body Imagesmike apriliaNo ratings yet
- Rudy SetiawanDocument9 pagesRudy Setiawanmike apriliaNo ratings yet
- USA, 1946 - Elements of The General HospitalDocument48 pagesUSA, 1946 - Elements of The General HospitalMari Julia SchmidtNo ratings yet
- Discharge PlanningDocument6 pagesDischarge PlanningHamdah GirlsNo ratings yet
- Ngwelezana Casebook in Emergency Surgery and TraumaDocument115 pagesNgwelezana Casebook in Emergency Surgery and TraumaAbeyna Latoya Charlotte JonesNo ratings yet
- Electrical Guide Health Facilities Review: Hospitals Skilled Nursing Facilities and ClinicsDocument58 pagesElectrical Guide Health Facilities Review: Hospitals Skilled Nursing Facilities and ClinicsLacides PadillaNo ratings yet
- Alumnus - Vol.44 #1Document4 pagesAlumnus - Vol.44 #1National University of Health SciencesNo ratings yet
- Directory of HospitalsDocument8 pagesDirectory of HospitalsShannen AndradeNo ratings yet
- Humidity Sample Policy: Appendix GDocument2 pagesHumidity Sample Policy: Appendix GsamsonNo ratings yet
- Kasus ToraksDocument31 pagesKasus ToraksAldhi Tri BudhiNo ratings yet
- The Street LawyerDocument5 pagesThe Street LawyerJulieta MuninNo ratings yet
- Chapter.1. Introduction To Insurance IndustryDocument64 pagesChapter.1. Introduction To Insurance IndustryKunal KaduNo ratings yet
- Bankurt RadiologyDocument22 pagesBankurt RadiologyVajja SwatiNo ratings yet
- Hospital and Dispensary Management.: (MavhDocument1 pageHospital and Dispensary Management.: (MavhAnonymous plTPAIjNo ratings yet
- Curriculum VitaeDocument7 pagesCurriculum VitaeRhea PunjabiNo ratings yet
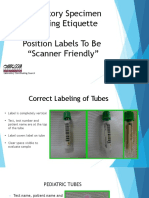
- Laboratory Specimen Labeling EtiquetteDocument42 pagesLaboratory Specimen Labeling EtiquettefaizNo ratings yet
- Medical GloveDocument3 pagesMedical GloveJyotiNo ratings yet
- PDSA Improvement Plan - Kingston General Hospital: Name Institution Course Professor DateDocument5 pagesPDSA Improvement Plan - Kingston General Hospital: Name Institution Course Professor DateNilanjana ChakrabortyNo ratings yet
- 81 Relative ClausesDocument24 pages81 Relative ClausesLeocádia Cardoso Ferreira100% (1)
- 1 - Understanding Medical TerminologyDocument27 pages1 - Understanding Medical TerminologySoina LarivaNo ratings yet
- Mid South Dermatology - General Consent Patient FormDocument1 pageMid South Dermatology - General Consent Patient FormjtdermNo ratings yet
- M.4 Unit 2 Past SimpleDocument217 pagesM.4 Unit 2 Past SimpleThanarath ChantarasakunNo ratings yet
- Earthquake Contingency Plan of Bogra Pourashava AreaDocument94 pagesEarthquake Contingency Plan of Bogra Pourashava AreaCDMP Bangladesh100% (3)
- JRDocument3 pagesJRlimbusNo ratings yet
- Spring 2022 Dean's List ValparaisoDocument2 pagesSpring 2022 Dean's List ValparaisoLeft SiderNo ratings yet
- Multitasking in NursingDocument6 pagesMultitasking in NursingFlorenciaAbudOyanederNo ratings yet
- Nursing Philosophy Relfection JournalDocument5 pagesNursing Philosophy Relfection Journalapi-569642906No ratings yet
- The Daily GrindDocument2 pagesThe Daily GrindRodrigo CarbajalNo ratings yet
- English Sample Essays SPM (I Do Not Own The Copyright)Document11 pagesEnglish Sample Essays SPM (I Do Not Own The Copyright)Siti Nahdatul NissaNo ratings yet
- Firefly Phototherapy BrochureDocument6 pagesFirefly Phototherapy BrochurePhạm ThịnhNo ratings yet