Professional Documents
Culture Documents
AJR Anatomy Report CTA
Uploaded by
Yohanes JonathanCopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
AJR Anatomy Report CTA
Uploaded by
Yohanes JonathanCopyright:
Available Formats
C a r d i o p u l m o n a r y I m a g i n g • R ev i ew
Sundaram et al.
Reporting of Cardiac MDCT
Cardiopulmonary Imaging
Review
Anatomy and Terminology
for the Interpretation and
Reporting of Cardiac MDCT:
Downloaded from www.ajronline.org by 114.124.201.237 on 07/09/19 from IP address 114.124.201.237. Copyright ARRS. For personal use only; all rights reserved
Part 1, Structured Report,
FOCUS ON:
Coronary Calcium Screening,
and Coronary Artery Anatomy
Baskaran Sundaram1 OBJECTIVE. In this part one of a two-part article, we aim to illustrate our understanding
Smita Patel of and approach to comprehensive cardiac CT reporting, cardiac CT technique, and coronary
Naama Bogot calcium scoring CT, as well as normal and anomalous coronary artery anatomy.
Ella A. Kazerooni CONCLUSION. Structured cardiac CT reporting is important to effectively commu-
nicate with referring clinicians. Knowledge of cardiac CT technique, cardiac anatomy, and
Sundaram B, Patel S, Bogot N, Kazerooni EA standard anatomic and physiologic terminology can assist the reader in creating a consistent
and comprehensive cardiac CT report.
C
ardiovascular disease has been Early experience on feasibility and usefulness
the leading cause of mortality in of coronary CTA using 320 detector rows has
the United States since 1958 [1]. been reported [28, 29]. Recently, the prognos-
Coronary artery disease (CAD) tic value of coronary CTA has also been re-
leads the group of cardiovascular diseases in ported in a large group of patients [30].
contributing to mortality. Many noninvasive To perform the coronary CTA examina-
tests are used to evaluate patients with sus- tion, interpret, and create a structured coro-
pected CAD, including the exercise treadmill nary CTA report of findings, it is important to
test, echocardiography, myocardial perfusion have a good understanding of the coronary
scintigraphy, and electron-beam CT (EBCT). CTA procedure, anatomy, pathology, and the
Invasive catheter coronary angiography with standard descriptions used in the reference
or without intravascular sonography is re- cardiac tests such as invasive catheter coro-
served for patients with a sufficiently high nary angiography and echocardiography. In
probability of disease to warrant this more in- the current climate of increasing utilization of
Keywords: cardiac CT, coronary CT angiography,
vasive and more expensive test with its associ- cross-sectional imaging for various indica-
CT reporting
ated risk of morbidity and mortality [2–4]. tions [31], multiple professional organizations,
DOI:10.2214/AJR.08.1177 Recent advances in CT technology allow non- including the American College of Radiology
invasive coronary CT angiography (CTA) and (ACR) and the American College of Cardiol-
Received May 7, 2008; accepted after revision left ventricular (LV) functional assessment. ogy (ACC), recently worked together to estab-
September 2, 2008.
Since its introduction, coronary CTA has be- lish appropriateness criteria for both cardiac
Gold Medal Exhibit Award for Education Exhibit at the come increasingly accepted as a quick and CT and MRI [6]. We recommend these crite-
2006 annual meeting of the American Roentgen Ray safe noninvasive coronary artery evaluation ria be used as a resource in practice for deter-
Society, Vancouver, BC, Canada. tool. Coronary artery stenosis detection, ac- mining the appropriateness of these examina-
1 curacy, and negative predictive value using tions. Recently, the ACR and the North
All authors: Division of Cardiothoracic Radiology,
Department of Radiology, University of Michigan Health coronary CTA are more impressively per- American Society for Cardiovascular Imag-
System, Cardiovascular Center, Rm. 5481, 1500 E Medical formed with 64-MDCT scanners than with ing (NASCI) together published a white paper
Center Dr., Ann Arbor, MI 48109-5868. Address 16- or 4-MDCT scanners [5, 6]. Further im- on the structured reporting of coronary CTA
correspondence to B. Sundaram (sundbask@umich.edu). provements are being explored in areas such [32]. Efforts from professional societies to
CME
as better CT resolution (both spatial and tem- standardize various facets of cardiac imaging
This article is available for CME credit. poral), dual-source CT [7–16], CT radiation continue to increase [33, 34].
See www.arrs.org for more information. dose reduction, and the feasibility of coronary
CTA in patients with suboptimal heart rates A Structured Cardiac CT Report
AJR 2009; 192:574–583
[17–19]. The usefulness of coronary CTA as a Our current comprehensive cardiac report
0361–803X/09/1923–574 comprehensive diagnostic tool has also been is composed of clinical indications for the
recently explored in the emergent manage- examination, a description of examination
© American Roentgen Ray Society ment of patients with acute chest pain [20–27]. technique and imaging findings, and a final
574 AJR:192, March 2009
Reporting of Cardiac MDCT
summary or impression that enumerates the grafts when scanning a CABG patient; this is cation (CAC) [35]. CAC is an established
salient coronary and noncoronary cardiac and less important if the scan range is confined to marker of atherosclerosis [36]. Amorphous
extracardiac findings. The reporting style that the native coronary arteries. hydroxyapatite deposits advance to differen-
we follow is shown in Appendices 1–3. The type of ECG gating is also specified, tiation of cells in the vessel wall to osteoblasts
In our reports, we aim to explicitly de- including prospective ECG triggering for the [37]. Although CAC is a specific indicator of
Downloaded from www.ajronline.org by 114.124.201.237 on 07/09/19 from IP address 114.124.201.237. Copyright ARRS. For personal use only; all rights reserved
scribe the cardiac CT protocol used. We pre- calcium score acquisition and either prospec- the presence of coronary artery atherosclero-
fer to document all pharmaceutical agents tive ECG triggering or retrospective gating sis, it represents only the calcified or healed
used for heart rate and rhythm control for coronary CTA. Radiation dose-reduction plaque, not the full burden of plaque. CAC is
(β-blockers, calcium blockers) and sublin- measures used, including tube current modu- estimated to represent approximately 10–20%
gual nitroglycerin used for temporary coro- lation techniques, are also mentioned in our of the total atherosclerotic plaque burden [38].
nary artery dilatation, including the dose, reports. Typically, in patients with a fixed R-R Patients who have CAC are more likely to
timing, and route of administration. We also interval, tube current modulation is used, with have noncalcified plaque that is prone to rup-
mention the heart rate and rhythm during the the mA being reduced at the phases of the R-R ture, leading to acute thrombosis, than pa-
acquisition because of their impact on the ac- interval that are generally not used for view- tients without CAC [38]. CAC is a predictor of
curacy of coronary CTA. ing the coronary arteries. In patients with a coronary events, myocardial infarction, and
Generally, for a typical coronary CTA ex- normal stable sinus rhythm and a heart rate of death [39]. Despite extensive research, the
amination, the prescribed scan range extends 65 beats per minute or lower, we acquire im- clinical indications and usefulness of calcium
from the angle of the carina to below the car- ages only at the LV end-diastole during the scoring have remained controversial.
diac apex; for patients with coronary artery cardiac cycle. This technique significantly re- CAC scoring was developed and used ini-
bypass grafts (CABGs) or who are having a duces the radiation dose without compromis- tially exclusively with EBCT scanners and
combined coronary artery and thoracic aorta ing image quality, but it sacrifices the dynam- validated with both radiologic–histopatho-
CT evaluation, the cranial extent of the scan ic cardiac functional data. LV end-diastole is logic correlation and multiple population-
zone is shifted superiorly to include the ori- when there is relatively little motion and the based studies [36, 40]. EBCT enabled ultra-
gins of the subclavian and internal mamma- greatest coronary artery blood flow, when the fast scanning of the heart using an electron
ry arteries. The method used to determine coronary arteries are usually the most opti- beam and a stationary tungsten target. Ex-
the scan delay time from the beginning of the mally visualized. LV end-systole is the second aminations were acquired at 50 or 100 milli-
IV contrast bolus is specified, whether it is a relatively motion-free part of the cardiac cycle seconds per slice, with nonoverlapping 3- to
region of interest (ROI)–based trigger or a and may be used when LV end-diastole is in- 5-mm slices, and a fixed mAs (≈ 60–65
timing bolus performed with an ROI placed sufficient, particularly for evaluation of the mAs) with prospective ECG triggering at
at the aortic root. vertical portions of the RCA and left circum- one selected point in the R-R interval—usu-
With respect to IV contrast administration, flex (LCX) coronary artery. ally end-diastole—to eliminate cardiac mo-
the type, concentration, quantity, rate, and The computer workstation and the soft- tion and blurring [38, 41]. Because EBCT
route of administration, as well as canula size, ware version used to review the images may scanners have limited clinical applications,
are usually included. In our reports, we also also be documented. If any specific quantifi- they are not widely used today. With advanc-
specify the format of the IV contrast bolus cation software is used to evaluate degree of es in MDCT technology, MDCT has become
used—specifically, whether a biphasic or a coronary artery stenosis and plaque charac- the primary CT platform for CT studies of
triphasic technique is used. A biphasic tech- terization, that may also be stated for the CAC [42].
nique uses saline as the second phase of the reader to understand the reliability of the re-
bolus, immediately after the contrast injec- sults. We mention the use of advanced image Calcium Scoring on MDCT
tion, to completely wash out contrast material postprocessing, such as creation of long- and Technique—MDCT scanners with 4 or
from the right heart chambers and to elimi- short-axis multiplanar reformations (MPRs), more detectors are recommended, with tem-
nate streak artifacts across the deep right curved MPRs, and volume-rendered images poral resolution of 500 milliseconds or less
atrioventricular groove in which the right cor- for coronary artery assessment. We also de- [35]. Examinations are performed in the
onary artery (RCA) sits. In a triphasic bolus, scribe quantitative and qualitative functional craniocaudal direction to cover the heart
contrast material is followed by a mixture of analysis of the LV using dynamic images in from the pulmonary trunk through the apex.
saline and contrast material, so that there is standard cardiac viewing planes, aortic valve The CT table is advanced in a steplike axial
some visualization of the morphology of the anatomy, and, if performed, measurements fashion. If a 16-MDCT scanner is used, scan
right heart chamber. For example, “80 mL of of the areas of aortic valve stenosis and re- duration is approximately 6–10 seconds; if
low-osmolar IV contrast material (370 mg I/ gurgitant orifices. all 16 detectors are used, collimation is ei-
mL of iodine concentration) was adminis- ther 0.5–0.75 mm width or 1.0–1.5 mm
tered at 5 mL/s via a 20-gauge canula placed CT Calcium Score width. The suggested mA is 100, which may
in the right antecubital fossa using a triphasic Background and Rationale be reduced to as little as 55 mA [43]. When
technique.” Right upper extremity venous ac- Calcium scoring with CT has been in use using 64-MDCT scanners, generally the
cess is preferred to avoid dense contrast mate- for more than 20 years. This noninvasive ac- gantry rotation time is 0.35 seconds, colli-
rial pooling in the left brachiocephalic vein quisition does not use IV contrast material mation is 64 × 0.625 mm, and reconstructed
and resulting in streak artifacts that could po- and is performed at a relatively low radiation slice thickness is set at 2.5 mm, although
tentially obscure aortic arch anatomy, great dose compared with coronary CTA. It is used there may be variations in technique depend-
vessel origins, and internal mammary artery to detect and quantify coronary artery calcifi- ing on the CT manufacturer. As with EBCT,
AJR:192, March 2009 575
Sundaram et al.
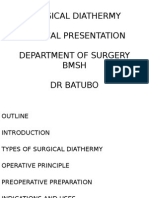
Fig. 1—55-year-old the percentile rank by sex, based on large co-
man with atypical chest
horts of asymptomatic individuals who have
pain had focal calcified
plaque (arrow) on this undergone CAC assessment. A calcium score
unenhanced coronary of 0 implies a low probability for significant
CT examination. After obstructive CAD and future cardiac events
manual identification of
Downloaded from www.ajronline.org by 114.124.201.237 on 07/09/19 from IP address 114.124.201.237. Copyright ARRS. For personal use only; all rights reserved
calcified plaque in mid [42]. However, it does not mean that a patient
portions of right coronary has no noncalcified or unstable plaque or that
artery, quantification the probability of a future coronary event is 0
software estimates
Agatston-Janowitz score
[57]. A positive calcium score correlates with
of 24 and volume score the amount of plaque and is an independent
of 18. predictor of obstructive CAD [58]. The high-
er the calcium score, the greater the amount
of plaque and the higher the relative risk for
cardiac events [59]. The presence of any
measurable calcium increases the risk of a
cardiac event in 3–5 years by nearly 4 times
[42]. Although a positive score is a specific
prospective ECG triggering is used, with a the mass method, pixel volume measuring marker for the presence of CAD and has a
radiation dose of approximately 1.5 mSv for 130 HU or more is multiplied by its attenua- high negative predictive value of 86–90% for
men and 1.8 mSv for women [44]. Few arti- tion in Hounsfield units, and the total calcu- obstructive coronary disease, it is not specif-
cles report coronary calcium scoring using lated value is divided by 100 [52]. The vol- ic for obstructive CAD [35].
the current 64-MDCT scanners [45–48]. ume and mass calcium scoring methods are
Postprocessing and calcium quantifica- less variable than the Agatston-Janowitz Normal Coronary Artery Anatomy
tion—The calcium score is generated using method [50]. Evaluation of the coronary arteries begins
software specifically designed for this pur- with an axial review of their origin and prox-
pose (Fig. 1). Semiquantitative scores are Clinical Indications and Implications of the CAC imal course. There are three sinuses of Val-
based on a section-by-section analysis of the Calcium scoring with CT has been exten- salva, the right sinus of Valsalva or the ante-
CT images [49]. There are three scoring sively tested for reliability and validity. A re- rior sinus, the left sinus of Valsalva or the
methods: the Agatston-Janowitz score, the cently published updated clinical expert con- posterior sinus, and the noncoronary sinus
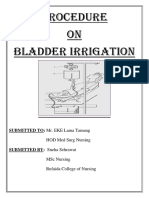
volume score, and the mass score. The Agat- sensus document by the ACC and the [60] (Fig. 2). The RCA and the left main cor-
ston-Janowitz score was the initial method American Heart Association (AHA) lists the onary artery (LM) arise from their respec-
for calcium quantification and is the most recommended clinical indications for calci- tive aortic sinuses of Valsalva. On axial im-
widely used. To be included in the Agatston- um scoring [42] (Appendix 4). Calcium scor- ages, the LM arises at a level that is cephalad
Janowitz score, CAC must reach a threshold ing is not recommended in asymptomatic pa- to the RCA.
of 130 HU and cover an area of at least 1 mm2; tients at high or low risk for CAD because it
calcifications that are lower in attenuation or does not affect medical management and de-
smaller in size are not included in the score. cision making [42]. Because the clinical out-
The score of each calcification is calculated come of plaque progression, its relationship
by multiplying the area of the CAC by an at- to quantifiable stenosis, and the effect of
tenuation-weighting factor based on the high- modifying therapy on plaque progression are
est HU value of the CAC, a score ranging unknown, plaque follow-up with calcium
from 1 to 4. A vessel score is the sum of all scoring is not recommended.
CAC scores of that vessel, and the total cal- Large focal calcifications significantly im-
cium score is the total of all CAC scores from pair evaluation of the underlying lumen in
all vessels [49]. This method has been in use coronary CTA, whereas diffusely scattered
the longest, and its prognostic implications small calcifications do not. Significant ob-
have been the most studied, but it has several structive coronary artery stenosis may be un-
limitations. First, it was developed for EBCT recognized in plaque having an Agatston-
and must be modified for MDCT. It is often Janowitz calcium score of 400 or more [53].
reported on MDCT as the Agatston score Few researchers have attempted to define the
equivalent. Second, the measurement is non- impact of coronary calcium on the accuracy
linear because of the attenuation-weighting of coronary CTA [54–56].
Fig. 2—48-year-old man with chest pain, elevated
factor. And third, there is high interscan vari- Calcium scoring quantifies the calcified cardiac enzymes, and normal ECG. Axial maximum-
ability because of partial volume averaging plaque alone. It does not directly visualize intensity-projection CT image of aortic root shows
effect and dependence on slice thickness and the vessel lumen, does not provide an esti- origin of right coronary artery (straight arrow) from
right coronary sinus and left main coronary artery
spacing [50]. In the volume score method, mate of coronary artery stenosis, and does
(curved arrow) from left coronary sinus. Arrowhead
the volume of all pixels with an identified not detect noncalcified plaque. The impor- indicates noncoronary sinus. RA = right atrium, LA =
ROI of 130 HU or more is included [51]. In tance of CAC to an individual is reported as left atrium, RVOT = right ventricular outflow tract.
576 AJR:192, March 2009
Reporting of Cardiac MDCT
ventricular groove, curving posteriorly at the the left anterior descending (LAD) and LCX
acute margin of the right ventricle (RV) and coronary arteries (Figs. 2 and 5A). The LM
bifurcating into the posterior descending ar- may be short or long, varying in length from 5
tery (PDA) and the posterolateral LV branch- to 20 mm [61]. Occasionally, the LM trifur-
es at the crux of the heart. The RCA supplies cates, with the middle branch known as the
Downloaded from www.ajronline.org by 114.124.201.237 on 07/09/19 from IP address 114.124.201.237. Copyright ARRS. For personal use only; all rights reserved
the RV free wall. The proximal branches of ramus intermedius (Fig. 5B). The LAD cours-
the RCA are the conus and sinoatrial branch- es anteriorly and inferiorly in the anterior in-
es. The conus branch arises from the RCA in terventricular groove to the apex of the heart,
half of the population and directly from the giving rise to septal perforators and diagonals.
aortic root in the other half. The sinoatrial The septal perforators run perpendicular to
nodal branch arises from the RCA in 60% of the LAD and supply the anterior two thirds of
people and from the LCX in 40%. The other the septum. The diagonals, of which there
branches of the RCA include the acute mar- may be up to six, are numbered sequentially
ginal branches and the atrioventricular nodal as they arise (D1, D2, and so forth). The diag-
branch. The PDA runs in the posterior inter- onals run on the epicardial surface of the heart
ventricular groove and supplies the posterior and supply the anterolateral portion of the LV.
third of the septum. The posterolateral LV The LAD has proximal, mid, and distal por-
branches supply the posterior surface of the tions. The proximal portion runs from the ori-
LV. The RCA is divided into proximal, mid, gin to the first septal perforator or first diago-
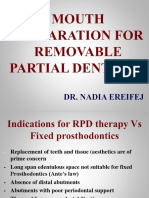
Fig. 3—47-year-old woman with hyperlipidemia and
and distal portions, with the proximal portion nal, the mid portion runs from there to the
hypertension. Volume-rendered image of right lateral extending from the origin to the acute margin- second diagonal, and the distal portion is dis-
view of heart created from IV contrast-enhanced al origin, the mid portion extending from the tal to the second diagonal origin.
ECG-gated coronary CT angiography image shows acute marginal origin to the horizontal por-
right coronary artery (curved arrow) coursing in right
atrioventricular groove. Right lateral surface of right tion in the posterior right atrioventricular Left Circumflex Artery
ventricle is perfused by acute marginal branches 1 groove, and the distal portion extending be- The LCX runs along the left atrioventricu-
(straight arrow) and 2 (arrowhead). yond that. lar groove and in 80–85% of the population
terminates at the obtuse margin of the heart
Right Coronary Artery Left Main and Left Anterior Descending after giving rise to the first obtuse marginal
The RCA (Figs. 2, 3, and 4A) courses ante- Coronary Arteries (OM1) branch (Figs. 4B and 5A). The LCX
riorly and laterally from its ostium at the right The LM arises from the left sinus of Val- supplies the lateral aspect of the LV. The pri-
sinus of Valsalva and runs in the right atrio- salva and divides into its two main branches, mary branches of the LCX are the OM arter-
A B C
Fig. 4—Volume-rendered images of posterior view of heart of three patients in whom posterior descending artery (PDA) (arrowhead) and posterolateral left ventricular
(LV) branches (straight arrows) define dominant patterns of coronary circulation.
A, Image in 52-year-old woman shows both PDA and posterolateral LV branches originate from distal right coronary artery (RCA) (curved arrow), suggesting right
coronary circulation dominance.
B, Image in 68-year-old man shows PDA and posterolateral LV branches arise from distal left circumflex coronary artery (LCX) (curved arrow), suggesting left coronary
circulation dominance.
C, Image in 50-year-old man shows PDA and posterolateral LV branches originate from RCA (curved arrow) and LCX, respectively, suggesting codominance (balanced
dominance) of coronary circulation.
AJR:192, March 2009 577
Sundaram et al.
Fig. 5—Volume-rendered images of anterior view
of heart in two patients in left anterior oblique
projection showing left coronary circulation.
A, Image in 58-year-old man with multiple cardiac
ischemic risk factors who presented with chest pain
shows left main artery (curved arrow), left anterior
descending (LAD) artery (arrowhead), and left
Downloaded from www.ajronline.org by 114.124.201.237 on 07/09/19 from IP address 114.124.201.237. Copyright ARRS. For personal use only; all rights reserved
circumflex artery (straight arrow). LAD also gives rise
to diagonal branches.
B, Image in 70-year-old woman shows ramus
intermedius branch (arrow).
A B
ies, numbered sequentially as they arise ion using the widely followed AHA coronary a coronary artery with an interarterial course
(OM1, OM2, and so forth). The LCX may artery segmentation model defining 15 seg- of the proximal segment between the aortic
also continue posteriorly to the crux of the ments in which the proximal, mid, and distal root and the RV outflow tract or pulmonary
heart; it gives rise to the PDA, the atrioven- portions of the RCA are respectively segments artery can be potentially fatal. Hence, an in-
tricular nodal branch, and the posterolateral 1–3; the PDA is segment 4; the LM is segment terarterial course is considered malignant,
LV branches. The LCX is divided into proxi- 5; the proximal, mid, and distal LAD are seg- whereas the retroaortic and prepulmonic
mal and distal portions in relation to the ma- ments 6–8; the D1 and D2 are segments 9 and courses are considered either benign or non-
jor OM branch origin. 10; the proximal and distal LCX are segments malignant. However, it is important to recog-
The dominance of the coronary circula- 11 and 13; the OM artery is segment 12; the nize the retroaortic course in patients who
tion is determined by the circulation that posterolateral LV branch is segment 14; and may potentially undergo surgery of the aortic
gives rise to the atrioventricular nodal artery, the PDA, if present as a branch of the LCX, is root or the ascending aorta (Figs. 6 and 7).
the PDA, and the posterolateral LV branches segment 15 [62]. Accurate diagnosis of a coronary artery
(Fig. 4). Eighty to 85% of the population anomaly is important, particularly in young
have right coronary circulation dominance, Anomalous Coronary Artery Anatomy athletes or in young military recruits, because
8–10% have left coronary dominance, and Anomalies of the coronary arteries are up to one third of cardiac-related deaths in
7–8% have codominance (balanced domi- rare, occurring in 0.3–5.6% of the popula- that age group are related to such anomalies
nance), in which the PDA and the postero- tion, and are often an incidental finding in [64]. For many years the diagnosis of coro-
lateral LV branches originate respectively asymptomatic patients [63]. Most coronary nary anomalies was made on invasive catheter
from the RCA and LCX (Fig. 4). anomalies do not have an adverse clinical coronary angiography or at autopsy. However,
On coronary CTA, coronary artery seg- outcome; however, the origin of a coronary the course of anomalous coronary arteries is
ments can be reported in a standardized fash- artery from the opposite sinus of Valsalva, or often difficult to determine at invasive cathe-
Fig. 6—Malignant course of coronary artery.
A, Oblique axial maximum-intensity-projection image
of aortic root in 14-year-old competitive male athlete
with exertional chest pain and palpitations shows
right coronary artery (curved arrow) arising from
left sinus of Valsalva (straight arrow) and coursing
in malignant fashion between right coronary sinus
(arrowhead) and right ventricular outflow tract
(RVOT). This anomalous coronary course was
surgically corrected.
B, Axial contrast-enhanced image at aortic root in
30-year-old woman shows left main coronary artery
(arrowhead) arising from right coronary sinus (arrow)
and coursing between RVOT and aortic root in
malignant fashion.
A B
578 AJR:192, March 2009
Reporting of Cardiac MDCT
Fig. 7—73-year-old man with suspected anomalous
coronary artery on catheter angiography. MPA = main
pulmonary artery.
A, Oblique axial maximum-intensity-projection image of
aortic root shows origin of left circumflex artery (curved
arrow) arising from right coronary sinus and coursing
between aortic root and left atrium (LA) in nonmalignant
Downloaded from www.ajronline.org by 114.124.201.237 on 07/09/19 from IP address 114.124.201.237. Copyright ARRS. For personal use only; all rights reserved
(retroaortic) course. Straight arrow indicates right
coronary artery; arrowhead, left anterior descending
artery.
B, Volume-rendered right anterior oblique image shows
left anterior descending artery (arrowhead) coursing
anterior to main pulmonary trunk in nonmalignant
(prepulmonic) course. Arrow indicates right coronary
artery.
A B
artery anomalies and their significance. In
part 2 of this article [71], we discuss coro-
nary artery atherosclerotic disease and car-
diac function assessment.
References
1. Hoyert DL, Heron MP, Murphy SL, Kung HC.
Deaths: final data for 2003. Natl Vital Stat Rep
2006; 54:1–120
2. Klinke WP, Kubac G, Talibi T, Lee SJ. Safety of
Fig. 8—44-year-old man with intermittent outpatient cardiac catheterizations. Am J Cardiol
nonspecific chest pain. Curved reformatted image 1985; 56:639–641
of mid left anterior descending artery shows 3. Papaconstantinou HD, Marshall AJ, Burrell CJ.
short segment of intramyocardial course (arrow)
Diagnostic cardiac catheterisation in a hospital
preceded and succeeded by extramyocardial course,
suggesting myocardial bridging. LV = left ventricle. without on-site cardiac surgery. Heart 1999;
81:465–469
ter coronary angiography. CT is now consid- correlate better with the depth than with the 4. Gersh BJ, Kronmal RA, Frye RL, et al. Coronary
ered the test of choice for evaluating the course length of the submyocardial segment [69]. arteriography and coronary artery bypass surgery:
of anomalous coronary arteries [65]. When Myocardial bridging may have a physiologic morbidity and mortality in patients ages 65 years
evaluating anomalous coronary arteries, it is limitation in coronary blood flow [70]; how- or older—a report from the Coronary Artery Sur-
important to define the origin and course. ever, its significance remains debatable [68]. gery Study. Circulation 1983; 67:483–491
Coronary anomalies can be due to variations 5. Stein PD, Beemath A, Kayali F, Skaf E, Sanchez
of origin, course, intrinsic coronary anatomy, Summary J, Olson RE. Multidetector computed tomography
and, rarely, termination [66, 67]. In conclusion, we have illustrated our for the diagnosis of coronary artery disease: a sys-
Coronary arteries are distributed along comprehensive approach to reporting coro- tematic review. Am J Med 2006; 119:203–216
the epicardial surface of the heart and are nary CTA findings that includes patient prep- 6. Hendel RC, Patel MR, Kramer CM, et al. ACCF/
surrounded by epicardial fat. When a coro- aration, acquisition technique, coronary cal- ACR/SCCT/SCMR/ASNC/NASCI/SCAI/SIR
nary artery segment tunnels through myo- cium scoring, and normal and anomalous 2006 appropriateness criteria for cardiac comput-
cardium, resulting in a submyocardial coro- coronary artery anatomy. This article may ed tomography and cardiac magnetic resonance
nary course that is preceded and succeeded provide fundamental information and im- imaging: a report of the American College of Car-
by an extramyocardial course, it is termed prove the understanding of coronary CTA diology Foundation Quality Strategic Directions
“myocardial bridging” [68] (Fig. 8). Myo- reporting pertaining to the background of Committee Appropriateness Criteria Working
cardial bridging is more readily identifiable CT coronary imaging, the calcium scoring Group, American College of Radiology, Society
on coronary CTA than on invasive catheter technique, clinical indications for and impli- of Cardiovascular Computed Tomography, Soci-
coronary angiography [69]. Systolic com- cations of calcium scoring, coronary artery ety for Cardiovascular Magnetic Resonance,
pression of myocardial bridging is found to anatomy, and an introduction to the coronary American Society of Nuclear Cardiology, North
AJR:192, March 2009 579
Sundaram et al.
American Society for Cardiac Imaging, Society 2005; 185:533–540 33. Weinreb JC, Larson PA, Woodard PK, et al. ACR
for Cardiovascular Angiography and Interven- 21. White C, Read K, Kuo D. Assessment of chest pain clinical statement on noninvasive cardiac imag-
tions, and Society of Interventional Radiology. J in the emergency room: what is the role of multide- ing. J Am Coll Radiol 2005; 2:471–477
Am Coll Cardiol 2006; 48:1475–1497 tector CT? Eur J Radiol 2006; 57:368–372 34. Budoff MJ, Cohen MC, Garcia MJ, et al. ACCF/
7. Pugliese F, Weustink AC, Van Mieghem C, et al. 22. Rubinshtein R, Halon DA, Gaspar T, et al. Impact AHA clinical competence statement on cardiac
Downloaded from www.ajronline.org by 114.124.201.237 on 07/09/19 from IP address 114.124.201.237. Copyright ARRS. For personal use only; all rights reserved
Dual-source coronary computed tomography an- of 64-slice cardiac computed tomographic angi- imaging with computed tomography and magnet-
giography for detecting in-stent restenosis. Heart ography on clinical decision-making in emergen- ic resonance: a report of the American College of
2008; 94:848–854 cy department patients with chest pain of possible Cardiology Foundation/American Heart Associa-
8. Stolzmann P, Scheffel H, Schertler T, et al. Radia- myocardial ischemic origin. Am J Cardiol 2007; tion/American College of Physicians Task Force
tion dose estimates in dual-source computed to- 100:1522–1526 on Clinical Competence and Training. J Am Coll
mography coronary angiography. Eur Radiol 23. Rubinshtein R, Halon DA, Gaspar T, et al. Useful- Cardiol 2005; 46:383–402
2008; 18:592–599 ness of 64-slice cardiac computed tomographic 35. Budoff MJ, Achenbach S, Blumenthal RS, et al. As-
9. Rixe J, Rolf A, Conradi G, et al. Image quality on angiography for diagnosing acute coronary syn- sessment of coronary artery disease by cardiac
dual-source computed-tomographic coronary an- dromes and predicting clinical outcome in emer- computed tomography: a scientific statement from
giography. Eur Radiol 2008; 18:1857–1862 gency department patients with chest pain of un- the American Heart Association Committee on
10. Brodoefel H, Burgstahler C, Tsiflikas I, et al. Du- certain origin. Circulation 2007; 115:1762–1768 Cardiovascular Imaging and Intervention, Council
al-source CT: effect of heart rate, heart rate vari- 24. Rubinshtein R, Gaspar T, Halon DA, Goldstein J, on Cardiovascular Radiology and Intervention, and
ability, and calcification on image quality and di- Peled N, Lewis BS. Prevalence and extent of ob- Committee on Cardiac Imaging, Council on Clini-
agnostic accuracy. Radiology 2008; 247:346–355 structive coronary artery disease in patients with cal Cardiology. Circulation 2006; 114:1761–1791
11. Bastarrika G, De Cecco CN, Arraiza M, et al. zero or low calcium score undergoing 64-slice 36. Wexler L, Brundage B, Crouse J, et al. Coronary
Dual-source CT coronary imaging in heart trans- cardiac multidetector computed tomography for artery calcification: pathophysiology, epidemiol-
plant recipients: image quality and optimal re- evaluation of a chest pain syndrome. Am J Cardiol ogy, imaging methods, and clinical implica-
construction interval. Eur Radiol 2008; 18:1791– 2007; 99:472–475 tions—a statement for health professionals from
1799 25. Rubinshtein R, Halon DA, Gaspar T, et al. Useful- the American Heart Association Writing Group.
12. Achenbach S, Anders K, Kalender WA. Dual- ness of 64-slice multidetector computed tomogra- Circulation 1996; 94:1175–1192
source cardiac computed tomography: image phy in diagnostic triage of patients with chest pain 37. Demer LL, Tintut Y. Mineral exploration: search
quality and dose considerations. Eur Radiol 2008; and negative or nondiagnostic exercise treadmill for the mechanism of vascular calcification and
18:1188–1198 test result. Am J Cardiol 2007; 99:925–929 beyond—the 2003 Jeffrey M. Hoeg Award lec-
13. Zhang ZH, Jin ZY, Zhang SY, et al. Coronary an- 26. Schussler JM, Smith ER. Sixty-four-slice com- ture. Arterioscler Thromb Vasc Biol 2003;
giography with dual source computed tomogra- puted tomographic coronary angiography: will 23:1739–1743
phy: initial experience. Chin Med Sci J 2007; the “triple rule out” change chest pain evaluation 38. Rumberger JA, Simons DB, Fitzpatrick LA,
22:205–210 in the ED? Am J Emerg Med 2007; 25:367–375 Sheedy PF, Schwartz RS. Coronary artery calci-
14. Seifarth H, Wienbeck S, Pusken M, et al. Optimal 27. Jeudy J, White CS. Evaluation of acute chest pain um area by electron-beam computed tomography
systolic and diastolic reconstruction windows for in the emergency department: utility of multide- and coronary atherosclerotic plaque area: a histo-
coronary CT angiography using dual-source CT. tector computed tomography. Semin Ultrasound pathologic correlative study. Circulation 1995;
AJR 2007; 189:1317–1323 CT MR 2007; 28:109–114 92:2157–2162
15. Ropers U, Ropers D, Pflederer T, et al. Influence 28. Dewey M, Zimmermann E, Laule M, Rutsch W, 39. Pletcher MJ, Tice JA, Pignone M, Browner WS.
of heart rate on the diagnostic accuracy of dual- Hamm B. Three-vessel coronary artery disease Using the coronary artery calcium score to predict
source computed tomography coronary angiogra- examined with 320-slice computed tomography coronary heart disease events: a systematic review
phy. J Am Coll Cardiol 2007; 50:2393–2398 coronary angiography. Eur Heart J 2008; 29:1669 and meta-analysis. Arch Intern Med 2004; 164:
16. Matt D, Scheffel H, Leschka S, et al. Dual-source 29. Rybicki FJ, Otero HJ, Steigner ML, et al. Initial 1285–1292
CT coronary angiography: image quality, mean evaluation of coronary images from 320-detector 40. Schoepf UJ, Becker CR, Ohnesorge BM, Yucel
heart rate, and heart rate variability. AJR 2007; row computed tomography. Int J Cardiovasc Im- EK. CT of coronary artery disease. Radiology
189:567–573 aging 2008; 24:535–546 2004; 232:18–37
17. Scheffel H, Alkadhi H, Plass A, et al. Accuracy of 30. Min JK, Shaw LJ, Devereux RB, et al. Prognostic 41. Mao S, Lu B, Oudiz RJ, Bakhsheshi H, Liu SC,
dual-source CT coronary angiography: first expe- value of multidetector coronary computed tomo- Budoff MJ. Coronary artery motion in electron
rience in a high pre-test probability population graphic angiography for prediction of all-cause beam tomography. J Comput Assist Tomogr 2000;
without heart rate control. Eur Radiol 2006; mortality. J Am Coll Cardiol 2007; 50:1161–1170 24:253–258
16:2739–2747 31. Broder J, Warshauer DM. Increasing utilization of 42. Greenland P, Bonow RO, Brundage BH, et al.
18. Johnson TR, Nikolaou K, Wintersperger BJ, et al. computed tomography in the adult emergency de- ACCF/AHA 2007 clinical expert consensus doc-
Dual-source CT cardiac imaging: initial experi- partment, 2000–2005. Emerg Radiol 2006; ument on coronary artery calcium scoring by
ence. Eur Radiol 2006; 16:1409–1415 13:25–30 computed tomography in global cardiovascular
19. Flohr TG, McCollough CH, Bruder H, et al. First 32. Stillman AE, Rubin GD, Teague SD, White RD, risk assessment and in evaluation of patients with
performance evaluation of a dual-source CT Woodard PK, Larson PA. Structured reporting: chest pain: a report of the American College of
(DSCT) system. Eur Radiol 2006; 16:256–268 coronary CT angiography—a white paper from Cardiology Foundation Clinical Expert Consen-
20. White CS, Kuo D, Kelemen M, et al. Chest pain the American College of Radiology and the North sus Task Force (ACCF/AHA Writing Committee
evaluation in the emergency department: can American Society for Cardiovascular Imaging. J to Update the 2000 Expert Consensus Document
MDCT provide a comprehensive evaluation? AJR Am Coll Radiol 2008; 5:796–800 on Electron Beam Computed Tomography). Cir-
580 AJR:192, March 2009
Reporting of Cardiac MDCT
culation 2007; 115:402–426 52. Detrano R, Tang W, Kang X, et al. Accurate coro- Little, Brown, 1984:xii, 430
43. Shemesh J, Evron R, Koren-Morag N, et al. Coro- nary calcium phosphate mass measurements 62. Austen WG, Edwards JE, Frye RL, et al. A report-
nary artery calcium measurement with multi-de- from electron beam computed tomograms. Am J ing system on patients evaluated for coronary ar-
tector row CT and low radiation dose: comparison Card Imaging 1995; 9:167–173 tery disease. Report of the Ad Hoc Committee for
between 55 and 165 mAs. Radiology 2005; 236: 53. Lau GT, Ridley LJ, Schieb MC, et al. Coronary Grading of Coronary Artery Disease, Council on
Downloaded from www.ajronline.org by 114.124.201.237 on 07/09/19 from IP address 114.124.201.237. Copyright ARRS. For personal use only; all rights reserved
810–814 artery stenoses: detection with calcium scoring, Cardiovascular Surgery, American Heart Associ-
44. Hunold P, Vogt FM, Schmermund A, et al. Radia- CT angiography, and both methods combined. ation. Circulation 1975; 51:5–40
tion exposure during cardiac CT: effective doses Radiology 2005; 235:415–422 63. Angelini P, Velasco JA, Flamm S. Coronary
at multi-detector row CT and electron-beam CT. 54. Brodoefel H, Reimann A, Burgstahler C, et al. anomalies: incidence, pathophysiology, and clini-
Radiology 2003; 226:145–152 Noninvasive coronary angiography using 64-slice cal relevance. Circulation 2002; 105:2449–2454
45. Scholte AJ, Schuijf JD, Kharagjitsingh AV, et al. spiral computed tomography in an unselected pa- 64. Eckart RE, Scoville SL, Campbell CL, et al. Sud-
Different manifestations of coronary artery dis- tient collective: effect of heart rate, heart rate den death in young adults: a 25-year review of
ease by stress SPECT myocardial perfusion im- variability and coronary calcifications on image autopsies in military recruits. Ann Intern Med
aging, coronary calcium scoring, and multislice quality and diagnostic accuracy. Eur J Radiol 2004; 141:829–834
CT coronary angiography in asymptomatic pa- 2008; 66:134–141 65. Schmitt R, Froehner S, Brunn J, et al. Congenital
tients with type 2 diabetes mellitus. J Nucl Car- 55. Heuschmid M, Kuettner A, Schroeder S, et al. anomalies of the coronary arteries: imaging with
diol 2008; 15:503–509 ECG-gated 16-MDCT of the coronary arteries: contrast-enhanced, multidetector computed to-
46. Schlosser T, Hunold P, Voigtlander T, Schmer- assessment of image quality and accuracy in de- mography. Eur Radiol 2005; 15:1110–1121
mund A, Barkhausen J. Coronary artery calcium tecting stenoses. AJR 2005; 184:1413–1419 66. Greenberg MA, Fish BG, Spindola-Franco H.
scoring: influence of reconstruction interval and 56. Ong TK, Chin SP, Liew CK, et al. Accuracy of Congenital anomalies of the coronary arteries:
reconstruction increment using 64-MDCT. AJR 64-row multidetector computed tomography in classification and significance. Radiol Clin North
2007; 188:1063–1068 detecting coronary artery disease in 134 symp- Am 1989; 27:1127–1146
47. Groen JM, Greuter MJ, Vliegenthart R, et al. Cal- tomatic patients: influence of calcification. Am 67. Kim SY, Seo JB, Do KH, et al. Coronary artery
cium scoring using 64-slice MDCT, dual source Heart J 2006; 151:1323; e1–e66 anomalies: classification and ECG-gated multi-
CT and EBT: a comparative phantom study. Int J 57. O’Rourke RA, Brundage BH, Froelicher VF, et al. detector row CT findings with angiographic cor-
Cardiovasc Imaging 2008; 24:547–556 American College of Cardiology/American Heart relation. RadioGraphics 2006; 26:317–333; dis-
48. Weininger M, Ritter CO, Beer M, Hahn D, Beis- Association Expert Consensus Document on elec- cussion 333–314
sert M. Evaluation of coronary calcifications with tron-beam computed tomography for the diagno- 68. Alegria JR, Herrmann J, Holmes DR Jr, Lerman
64-slice CT: variability of the scores and the influ- sis and prognosis of coronary artery disease. J Am A, Rihal CS. Myocardial bridging. Eur Heart J
ence of the reconstruction interval [in German]. Coll Cardiol 2000; 36:326–340 2005; 26:1159–1168
Rofo 2007; 179:938–944 58. Bielak LF, Rumberger JA, Sheedy PF 2nd, 69. Leschka S, Koepfli P, Husmann L, et al. Myocar-
49. Agatston AS, Janowitz WR, Hildner FJ, Zusmer Schwartz RS, Peyser PA. Probabilistic model for dial bridging: depiction rate and morphology at
NR, Viamonte M Jr, Detrano R. Quantification of prediction of angiographically defined obstructive CT coronary angiography—comparison with
coronary artery calcium using ultrafast computed coronary artery disease using electron beam com- conventional coronary angiography. Radiology
tomography. J Am Coll Cardiol 1990; 15:827– puted tomography calcium score strata. Circula- 2008; 246:754–762
832 tion 2000; 102:380–385 70. Schwarz ER, Klues HG, vom Dahl J, Klein I,
50. Yoon HC, Greaser LE 3rd, Mather R, Sinha S, 59. Keelan PC, Bielak LF, Ashai K, et al. Long-term Krebs W, Hanrath P. Functional characteristics of
McNitt-Gray MF, Goldin JG. Coronary artery prognostic value of coronary calcification detect- myocardial bridging: a combined angiographic
calcium: alternate methods for accurate and re- ed by electron-beam computed tomography in and intracoronary Doppler flow study. Eur Heart
producible quantitation. Acad Radiol 1997; patients undergoing coronary angiography. Circu- J 1997; 18:434–442
4:666–673 lation 2001; 104:412–417 71. Sundaram B, Patel S, Agarwal P, Kazerooni EA.
51. Kaufmann RB, Sheedy PF 2nd, Breen JF, et al. 60. Sevrukov A, Jelnin V, Kondos GT. Electron Anatomy and terminology for the interpretation
Detection of heart calcification with electron beam CT of the coronary arteries: cross-sec- and reporting of cardiac MDCT: part 2, CT angio
beam CT: interobserver and intraobserver reli- tional anatomy for calcium scoring. AJR 2001; graphy, cardiac function assessment, and non
ability for scoring quantification. Radiology 1994; 177:1437–1445 coronary and extracardiac findings. AJR 2009;
190:347–352 61. Miller SW. Cardiac angiography. Boston, MA: 192:584–598
Appendices follow on next page
AJR:192, March 2009 581
Sundaram et al.
APPENDIX 1: Our Structured Cardiac CT Report Template
CT Coronary Calcium Scoring:
• LMA = ( ), LAD = ( ), LCX = ( ), RCA = ( ), PDA = ( )
• Total calcium score = ( ) using the AJ-130 method and ( ) volume score
• ( ) percentile rank for age and gender, meaning that ( )% of patients of the same age and gender will have a higher score
Downloaded from www.ajronline.org by 114.124.201.237 on 07/09/19 from IP address 114.124.201.237. Copyright ARRS. For personal use only; all rights reserved
Coronary CT Angiography:
• Coronary arterial dominance (right, left, codominant)
• Left main, LAD and diagonals, LCX and obtuse marginal, RCA and posterior descending, ramus intermedius, and any anatomic
variants
• Quantification of stenoses (mild < 50%/mod 50–70%/severe > 70%)
Cardiac Structure, Morphology, and Function:
• Evaluation of short- and long-axis LV cines demonstrates (normal regional left ventricular wall motion) or (hypokinesis, akinesis, or
dyskinesis; specify wall or if global)
• LV functional parameters: end-diastolic volume, end-systolic volume, stroke volume, cardiac output, ejection fraction, LV mass
Summary:
1. Total coronary calcium score = ( ).
2. (Normal coronary arteries or specify abnormality).
3. (Normal or abnormal) left ventricular wall motion. LV ejection fraction = ( ).
4. (Normal or abnormal) cardiac chamber size.
Note—LMA = left main artery, LAD = left anterior descending artery, LCX = left circumflex artery, RCA = right coronary artery, PDA =
posterior descending artery, AJ-130 method = Agatston-Janowitz score of 130 HU, mod = moderate, LV = left ventricle.
APPENDIX 2: Coronary CT Angiography, Technical Details
• Pharmaceutical agents (quantity, route, rate of administration)
• Cardiac rate, rhythm, scan coverage zone
• Scan delay time method, biphasic/triphasic bolus technique
• IV contrast: name, concentration, quantity, rate, and route
• Prospective/retrospective ECG gating techniques
• Radiation dose-reduction measures
• Computer workstation viewing software
Appendices continue on next page
582 AJR:192, March 2009
Reporting of Cardiac MDCT
APPENDIX 3: Coronary CT Findings
Coronary Arteries:
• Calcium score with age/sex percentile rank
• Coronary artery origin, course, and dominance
• Atherosclerosis (plaque composition, luminal narrowing)
Downloaded from www.ajronline.org by 114.124.201.237 on 07/09/19 from IP address 114.124.201.237. Copyright ARRS. For personal use only; all rights reserved
Noncoronary Cardiovascular Structures:
• Quantitative evaluation of left ventricle (LV)
– Stroke volume (SV), ejection fraction (EF), cardiac output (CO), end-diastolic and end-systolic volumes (EDV and ESV)
• Qualitative evaluation of LV wall motion
• Cardiac chamber size and morphology (LV mass)
• Cardiac valve morphology
• Pericardium
• Other cardiovascular structures
– Aorta, pulmonary artery tree, and pulmonary veins
– Superior and inferior venae cavae
– Coronary veins
Noncardiovascular Structures:
• Lungs, pleura, airways
• Esophagus, mediastinal and hilar lymph nodes
• Diaphragm, body wall including osseous structures
• Upper abdominal contents (organs, bowel loops, mesentery)
APPENDIX 4: Recommended Use for Calcium Scoring CT
Asymptomatic Patients:
• Intermediate risk for coronary artery disease; total calcium score > 400 raises risk to high, justifying lifestyle modification
and pharmacological therapy maximization
Symptomatic Patients:
• A screeening tool before performing invasive procedures
• Functional testing (such as stress test) is not possible or is inconclusive
Note—Adapted from [42].
F O R YO U R I N F O R M AT I O N
• The reader’s attention is directed to part 2 of this article, titled “Anatomy and Terminology for the Interpretation
and Reporting of Cardiac MDCT: Part 2, CT Angiography, Cardiac Function Assessment, and Noncoronary and
Extracardiac Findings,” which appears on page 584.
• This article is available for CME credit. See www.arrs.org for more information.
AJR:192, March 2009 583
This article has been cited by:
1. Anil Attili, Ella A. Kazerooni. Structured Reporting for Cardiac CT 173-193. [Crossref]
2. Hamidreza Pouraliakbar. Cardiac Computed Tomography 131-158. [Crossref]
3. Christoph Gräni, Dominik C. Benz, Dominik A. Steffen, Andreas A. Giannopoulos, Michael Messerli, Aju P. Pazhenkottil,
Oliver Gaemperli, Cathérine Gebhard, Christian Schmied, Philipp A. Kaufmann, Ronny R. Buechel. 2018. Sports Behavior in
Downloaded from www.ajronline.org by 114.124.201.237 on 07/09/19 from IP address 114.124.201.237. Copyright ARRS. For personal use only; all rights reserved
Middle-Aged Individuals with Anomalous Coronary Artery from the Opposite Sinus of Valsalva. Cardiology 222-230. [Crossref]
4. Christoph Gräni, Ronny R. Buechel, Philipp A. Kaufmann, Raymond Y. Kwong. 2017. Multimodality Imaging in Individuals
With Anomalous Coronary Arteries. JACC: Cardiovascular Imaging 10:4, 471-481. [Crossref]
5. Christoph Gräni, Dominik C. Benz, Christian Schmied, Jan Vontobel, Fran Mikulicic, Mathias Possner, Olivier F. Clerc, Julia
Stehli, Tobias A. Fuchs, Aju P. Pazhenkottil, Oliver Gaemperli, Ronny R. Buechel, Philipp A. Kaufmann. 2017. Hybrid CCTA/
SPECT myocardial perfusion imaging findings in patients with anomalous origin of coronary arteries from the opposite sinus
and suspected concomitant coronary artery disease. Journal of Nuclear Cardiology 24:1, 226-234. [Crossref]
6. Leonardo P. Marcal, Patricia S. Fox, Douglas B. Evans, Jason B. Fleming, Gauri R. Varadhachary, Matthew H. Katz, Eric P.
Tamm. 2015. Analysis of free-form radiology dictations for completeness and clarity for pancreatic cancer staging. Abdominal
Imaging 40:7, 2391-2397. [Crossref]
7. Nuno Cardim, Maurizio Galderisi, Thor Edvardsen, Sven Plein, Bogdan A. Popescu, Antonello D'Andrea, Oliver Bruder,
Bernard Cosyns, Laurent Davin, Erwan Donal, Antonio Freitas, Gilbert Habib, Anastasia Kitsiou, Steffen E. Petersen, Stephen
Schroeder, Patrizio Lancellotti. 2015. Role of multimodality cardiac imaging in the management of patients with hypertrophic
cardiomyopathy: an expert consensus of the European Association of Cardiovascular Imaging Endorsed by the Saudi Heart
Association. European Heart Journal – Cardiovascular Imaging 16:3, 280-280. [Crossref]
8. Katarzyna Michaud, Silke Grabherr, Mohamed Faouzi, Jochen Grimm, Francesco Doenz, Patrice Mangin. 2015.
Pathomorphological and CT-angiographical characteristics of coronary atherosclerotic plaques in cases of sudden cardiac death.
International Journal of Legal Medicine 129:5, 1067. [Crossref]
9. Michele Porcu, Marco Francone, Giovanni Maria Argiolas, Giuseppe Cannavale, Mario Piga, Jasjit S. Suri, Iacopo Carbone,
Carlo Catalano, Luca Saba. CT Imaging of Coronary Arteries 29-60. [Crossref]
10. Andreas Wibmer, Hebert Alberto Vargas, Ramon Sosa, Junting Zheng, Chaya Moskowitz, Hedvig Hricak. 2014. Value of a
Standardized Lexicon for Reporting Levels of Diagnostic Certainty in Prostate MRI. American Journal of Roentgenology 203:6,
W651-W657. [Abstract] [Full Text] [PDF] [PDF Plus]
11. C. Erol, M. Seker. 2012. The prevalence of coronary artery variations on coronary computed tomography angiography. Acta
Radiologica 53:3, 278-284. [Crossref]
12. Minh Lu, Charles S. White. 2011. Cardiac CT Angiography: Protocols, Applications, and Limitations. PET Clinics 6:4,
441-452. [Crossref]
13. Chandra Katikireddy, Michael V. McConnell. Cardiac MRI and CT 303-325. [Crossref]
14. Bruce I. Reiner. 2009. The Challenges, Opportunities, and Imperative of Structured Reporting in Medical Imaging. Journal
of Digital Imaging 22:6, 562-568. [Crossref]
You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- MEDACS ReferenceDocument3 pagesMEDACS ReferencejahangirealamNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Eye OSPE Compiled and SolvedDocument41 pagesEye OSPE Compiled and SolvedHoney100% (2)
- Morse Fall ScaleDocument2 pagesMorse Fall ScaleFloryOrinDedDyJuliantNo ratings yet
- Fundamentals of Nursing1Document51 pagesFundamentals of Nursing1Charles Gerard B. BeluanNo ratings yet
- Home Visit & Bag Technique ChecklistDocument3 pagesHome Visit & Bag Technique ChecklistRALPH ELVIN MACANLALAYNo ratings yet
- Master How To Best Use Boger and Boenninghausen Repertory Contents Reading ExcerptDocument17 pagesMaster How To Best Use Boger and Boenninghausen Repertory Contents Reading Excerptdipgang7174100% (1)
- Surgical DiathermyDocument27 pagesSurgical DiathermyNimi Batubo100% (1)
- Rubrics NCP NCM 103 SL Funda VSDocument1 pageRubrics NCP NCM 103 SL Funda VSJohn TacordaJrNo ratings yet
- Poster Case Report Cesarean Scar PregnancyDocument1 pagePoster Case Report Cesarean Scar PregnancyAmanda Mustika Adi100% (1)
- Bladder Irrigation Procedure-1Document10 pagesBladder Irrigation Procedure-1Raja80% (5)
- MYCINDocument5 pagesMYCINsaurabh3112vermaNo ratings yet
- FeedbackDocument2 pagesFeedbackBerkeley ValeNo ratings yet
- GO5509 ResidenDocument4 pagesGO5509 ResidenBrunoNo ratings yet
- Incorporating The SALINE Process and Spiritual Care in Advanced Nursing PracticeDocument6 pagesIncorporating The SALINE Process and Spiritual Care in Advanced Nursing PracticeAdrian Fulton BrumfieldNo ratings yet
- Health Care Transparency Final PaperDocument19 pagesHealth Care Transparency Final Paperapi-242664158No ratings yet
- Journal of Psychiatry & Mental DisordersDocument2 pagesJournal of Psychiatry & Mental DisordersAustin Publishing GroupNo ratings yet
- Modern Healthcare - March 05 2018 PDFDocument44 pagesModern Healthcare - March 05 2018 PDFTan JayNo ratings yet
- Ib Psych Lesson Plan Week 12 f19 YlDocument2 pagesIb Psych Lesson Plan Week 12 f19 Ylapi-280368667No ratings yet
- Acute Renal Failure Lecture 1 Critical Care NursingDocument52 pagesAcute Renal Failure Lecture 1 Critical Care NursingDina Rasmita100% (2)
- Mouth Preparation For RPD Treatment-1-ModifiedDocument76 pagesMouth Preparation For RPD Treatment-1-ModifiedShemi SirajNo ratings yet
- A Report On Depression: Mental HealthDocument12 pagesA Report On Depression: Mental HealthArchiev KumarNo ratings yet
- CvsDocument35 pagesCvsVISS11No ratings yet
- What To Do, When Gbs PT Fails To Respond To TreatmentDocument4 pagesWhat To Do, When Gbs PT Fails To Respond To Treatmentidno1008No ratings yet
- Patient Information: Corp.: Bill To:: Doc. No: LPL/CLC/QF/2806Document1 pagePatient Information: Corp.: Bill To:: Doc. No: LPL/CLC/QF/2806TarunNo ratings yet
- Care PlanDocument3 pagesCare Plankatie2784No ratings yet
- Section 1: Epworth Sleepiness ScaleDocument3 pagesSection 1: Epworth Sleepiness ScaledwNo ratings yet
- Pharmacology II OutlineDocument52 pagesPharmacology II Outlinerjones53No ratings yet
- Understanding Oligodendroglioma - The Rarest of All Brain CancersDocument2 pagesUnderstanding Oligodendroglioma - The Rarest of All Brain CancersChris RyanNo ratings yet
- Hubungan Kadar Hemoglobin Dan Tercapainya Remisi Pada Anak Penderita Leukemia AkutDocument7 pagesHubungan Kadar Hemoglobin Dan Tercapainya Remisi Pada Anak Penderita Leukemia AkutRezky RahmadayantiNo ratings yet
- Ileus in Critical Illness Mechanisms And.11Document6 pagesIleus in Critical Illness Mechanisms And.11albimar239512No ratings yet