You might also like
- Hyper Calc Emi ADocument26 pagesHyper Calc Emi AAman Tayal0% (1)
- Hosp Ops II Week 2 Questions 1Document3 pagesHosp Ops II Week 2 Questions 1api-650133203No ratings yet
- RanolazineDocument20 pagesRanolazineashNo ratings yet
- Access Pathways To Queensland Health Adult Inpatient Beds For Patients With Eating DisordersDocument10 pagesAccess Pathways To Queensland Health Adult Inpatient Beds For Patients With Eating DisordersGrace McConnochieNo ratings yet
- SAAI Protocol KankerDocument4 pagesSAAI Protocol KankerSadha MahardhikaNo ratings yet
- New Zealand Data Sheet: Page 1 of 19Document19 pagesNew Zealand Data Sheet: Page 1 of 19Pharmacist Ehab HammadNo ratings yet
- Anticoagulation Protocol For PostDocument8 pagesAnticoagulation Protocol For PostMohammed IbrahimNo ratings yet
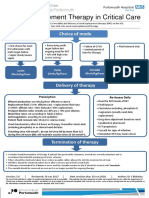
- Renal Replacement Therapy in Critical Care: Choice of ModeDocument15 pagesRenal Replacement Therapy in Critical Care: Choice of ModePeter AgabaNo ratings yet
- Activity # 7 Fluid and Electrolyte Balance (WITH NCP)Document15 pagesActivity # 7 Fluid and Electrolyte Balance (WITH NCP)Louise OpinaNo ratings yet
- Management of Potassium Disorders 17706 ArticleDocument4 pagesManagement of Potassium Disorders 17706 ArticlealeNo ratings yet
- Apixaban Eliquis MonographDocument14 pagesApixaban Eliquis MonographTran Minh NgocNo ratings yet
- Renal Impairment: Appendix-4Document9 pagesRenal Impairment: Appendix-4CLICK & WATCHNo ratings yet
- Hypoparathyroidism: DR Ranganath N Professor Department of OrthopaedicsDocument33 pagesHypoparathyroidism: DR Ranganath N Professor Department of Orthopaedicsnandhana s nairNo ratings yet
- HypercalcemiaDocument12 pagesHypercalcemiaAnam MirNo ratings yet
- Dokumen - Pub - Current Hospital Medicine Quick Guide For Management of Common Medical Conditions in Acute Care Setting 1stnbspedDocument54 pagesDokumen - Pub - Current Hospital Medicine Quick Guide For Management of Common Medical Conditions in Acute Care Setting 1stnbspedMahmoud FathyNo ratings yet
- Con 1420782810247Document7 pagesCon 1420782810247AsetonitrileNo ratings yet
- SFMH Mental Health AssessmentDocument24 pagesSFMH Mental Health AssessmentKholiwe Cassie MasekwaneNo ratings yet
- Jurding ACLSDocument30 pagesJurding ACLSmelvinNo ratings yet
- Hypercalcemia & MSCCDocument29 pagesHypercalcemia & MSCCSA NodeNo ratings yet
- Ascites, SBP, Encephlopathy 2Document78 pagesAscites, SBP, Encephlopathy 2Rida AkramNo ratings yet
- Brajac - ProtocolDocument13 pagesBrajac - Protocolthanh ngôNo ratings yet
- 15-Acute Kidney InjuryDocument18 pages15-Acute Kidney Injuryمصطفى محمد جواد كاظمNo ratings yet
- 2022-OXFORD-HANDBOOK-OF-ANAESTHESIA-Oxford-Press-5th-Edition ExportDocument4 pages2022-OXFORD-HANDBOOK-OF-ANAESTHESIA-Oxford-Press-5th-Edition ExportHany ElbarougyNo ratings yet
- AKI MBCHB VDocument64 pagesAKI MBCHB VSsenyonga DominicNo ratings yet
- Arritmias X HipercalemiaDocument9 pagesArritmias X Hipercalemiafh2301lrNo ratings yet
- Drugs & DialysisDocument34 pagesDrugs & DialysisZulfkar Latief QadrieNo ratings yet
- אלון קלציום חלק 3Document25 pagesאלון קלציום חלק 3Alon GoldfainerNo ratings yet
- Hemostan, Methergine CA Gluconate2Document4 pagesHemostan, Methergine CA Gluconate2Stacy MC PelitoNo ratings yet
- Potassium Chloride GuidelinesDocument25 pagesPotassium Chloride GuidelinesYasser Gebril86% (7)
- Agatha Christie - Craciunul Lui PoirotDocument14 pagesAgatha Christie - Craciunul Lui PoirotIokan DanNo ratings yet
- Oncologic EmergenciespaghubasanDocument10 pagesOncologic EmergenciespaghubasanRoyce Vincent TizonNo ratings yet
- Acute Kidney Injury:: A Brief OutlineDocument48 pagesAcute Kidney Injury:: A Brief OutlinehanaNo ratings yet
- Cardiotoxicology ToxicologyDocument41 pagesCardiotoxicology ToxicologyIncha MaayaloNo ratings yet
- Kidney Emergency: M. Syamsul BakhriDocument30 pagesKidney Emergency: M. Syamsul BakhrierahadeNo ratings yet
- Beyond Statins - NEW AHA/ACC Cholesterol Guidelines: Diane Osborn ARNP, CLSDocument54 pagesBeyond Statins - NEW AHA/ACC Cholesterol Guidelines: Diane Osborn ARNP, CLSDilan GalaryNo ratings yet
- Cardiovascular Blok 6.1 28 Feb 2018Document56 pagesCardiovascular Blok 6.1 28 Feb 2018widya vannesaNo ratings yet
- Gocxcrt ProtocolDocument3 pagesGocxcrt ProtocolNovrilia AtikaNo ratings yet
- Clozapine: Therapy, Side Effects, Monitoring RequirementsDocument24 pagesClozapine: Therapy, Side Effects, Monitoring RequirementsalinuxykNo ratings yet
- Acute Care Patient Case Example: CC: Hpi: Medical History: Medication History: Allergies: NKDADocument7 pagesAcute Care Patient Case Example: CC: Hpi: Medical History: Medication History: Allergies: NKDAخلودخلودNo ratings yet
- Protokol SarcomaDocument4 pagesProtokol SarcomaHep PutNo ratings yet
- Acute Kidney Injury (AKI) : Haerani Rasyid FK Unhas 2016Document46 pagesAcute Kidney Injury (AKI) : Haerani Rasyid FK Unhas 2016Ana Yusriana AzzahraNo ratings yet
- Group 2 Activity 4 and 5 Calcium and HCG DeterminationDocument8 pagesGroup 2 Activity 4 and 5 Calcium and HCG DeterminationRafael SaldivarNo ratings yet
- ACUTE KIDNEY INJURY (AutoRecovered)Document21 pagesACUTE KIDNEY INJURY (AutoRecovered)Axsa Alex100% (1)
- ACUTE KIDNEY INJURY by Dr. Monday Jacob ZaccheausDocument70 pagesACUTE KIDNEY INJURY by Dr. Monday Jacob ZaccheausDr. Amb. Monday ZaccheausNo ratings yet
- COVID-19 Protocol by EVMSDocument13 pagesCOVID-19 Protocol by EVMSKrishnamurthi CG100% (1)
- Sec1 Clinical2 (ARF)Document44 pagesSec1 Clinical2 (ARF)ahmedmohamed01153159469No ratings yet
- Atacor SPCDocument9 pagesAtacor SPCRannia1No ratings yet
- Prescribing Information Abiratred Abiraterone Acetate Tablets 250 MGDocument9 pagesPrescribing Information Abiratred Abiraterone Acetate Tablets 250 MGChrisNo ratings yet
- Annex III Summary of Product Characteristics and Package LeafletDocument13 pagesAnnex III Summary of Product Characteristics and Package LeafletJhanneth Jhovanna Chura PacoNo ratings yet
- Assessment and Concept Map Care Plan For Critical Care PatientDocument11 pagesAssessment and Concept Map Care Plan For Critical Care Patientapi-604551723No ratings yet
- Drugs Used in Cardiovascular SystemDocument57 pagesDrugs Used in Cardiovascular SystemSandeep ChaudharyNo ratings yet
- A I - E M: Drenal Nsufficiency Mergency AnagementDocument12 pagesA I - E M: Drenal Nsufficiency Mergency AnagementCaity YoungNo ratings yet
- SKILL STATION Management of Critically Ill Patient With Septic Shock Provider GuideDocument27 pagesSKILL STATION Management of Critically Ill Patient With Septic Shock Provider GuidesrinidhiNo ratings yet
- Integrated Therapeutics II: January 2020Document700 pagesIntegrated Therapeutics II: January 2020Seyoum Tumsa100% (1)
- Summary of Product CharacteristicsDocument9 pagesSummary of Product Characteristicsddandan_2No ratings yet
- Peritonitis in Peritoneal Dialysis Patients 1.0 PDFDocument12 pagesPeritonitis in Peritoneal Dialysis Patients 1.0 PDFIndo MahardikaNo ratings yet
- Zaroxolyn MetolazoneDocument1 pageZaroxolyn MetolazoneCassieNo ratings yet
- Carrick 2018Document7 pagesCarrick 2018Edwin AlvarezNo ratings yet
- TCA PoisoningDocument4 pagesTCA PoisoningaayceeNo ratings yet
- Impact of Foreign Direct Investment On Economic Growth in PakistanDocument6 pagesImpact of Foreign Direct Investment On Economic Growth in Pakistansuperiorsambrial examcellNo ratings yet
- Express VPN CodeDocument2 pagesExpress VPN Codesuperiorsambrial examcellNo ratings yet
- Audit Policies and Practices CommitteeDocument28 pagesAudit Policies and Practices Committeesuperiorsambrial examcellNo ratings yet
- Thesis Abhishek MishraDocument45 pagesThesis Abhishek Mishrasuperiorsambrial examcellNo ratings yet
- New Clinical Analysis and Device For Botox InjectionsDocument4 pagesNew Clinical Analysis and Device For Botox Injectionsleenatalia93No ratings yet
- Lesson 6 Thyroid and Antithyroid DrugsDocument28 pagesLesson 6 Thyroid and Antithyroid DrugstheintrovNo ratings yet
- Health Screenig ServicesDocument36 pagesHealth Screenig ServicesTarachand LalwaniNo ratings yet
- Solo Star in S Truc BrochureDocument8 pagesSolo Star in S Truc BrochurecnusistaNo ratings yet
- HR July 5 736pmDocument20 pagesHR July 5 736pmThomasNo ratings yet
- Richard LangDocument6 pagesRichard LangDanku MártonNo ratings yet
- 1 Octeto de DefronzoDocument23 pages1 Octeto de DefronzoLesli Rodriguez50% (2)
- Bio Electromagnetic Implications For Health and Healing - Valone 2010Document6 pagesBio Electromagnetic Implications For Health and Healing - Valone 2010Thomas Valone100% (2)
- FMGE Information BulletinDocument17 pagesFMGE Information Bulletinmahesh100% (4)
- Relining in RPD!Document33 pagesRelining in RPD!sarah50% (2)
- STG General HospitalDocument682 pagesSTG General HospitalhaalefomNo ratings yet
- Anti Anxiety MedicationsDocument2 pagesAnti Anxiety MedicationsjhgkhgkhgNo ratings yet
- DysphasiaDocument48 pagesDysphasiaredroseeeeee100% (1)
- Arch Forms 1-Ortho / Orthodontic Courses by Indian Dental AcademyDocument48 pagesArch Forms 1-Ortho / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- Gpat 2019Document51 pagesGpat 2019Nishabh KushwahaNo ratings yet
- Fractures of The Posterior Wall of The Acetabulum: Michael R. Baumgaertner, MDDocument12 pagesFractures of The Posterior Wall of The Acetabulum: Michael R. Baumgaertner, MDFaiz NazriNo ratings yet
- PneumothoraxDocument24 pagesPneumothoraxItharshan IndreswaranNo ratings yet
- Certificate Best PresenterDocument9 pagesCertificate Best PresenterRanie Livero O VillaminNo ratings yet
- Pricelist TreatmentDocument2 pagesPricelist TreatmentikaNo ratings yet
- ESCEO Algoritmo Manejo OADocument9 pagesESCEO Algoritmo Manejo OAMarco LenzNo ratings yet
- Ayurvedic Itihas Module - Final - 10-05-17Document7 pagesAyurvedic Itihas Module - Final - 10-05-17Vd Nisha ParmarNo ratings yet
- Sensory Imbalance of Patients in The Intensive Care UnitDocument3 pagesSensory Imbalance of Patients in The Intensive Care UnitkumfawandiNo ratings yet
- MEDraysintell Nuclear Medicine Edition 2017 - Summary and TOCDocument6 pagesMEDraysintell Nuclear Medicine Edition 2017 - Summary and TOCLadipo Temitope AyodejiNo ratings yet
- Diagnostic Dyspraxia and Apraxia in Nmda EncephalitisDocument2 pagesDiagnostic Dyspraxia and Apraxia in Nmda EncephalitisPriyanka SamalNo ratings yet
- AaaDocument313 pagesAaaDanesh RafaNo ratings yet
- Autism Resource GuideDocument22 pagesAutism Resource Guideapi-541216557No ratings yet
- Yan Xin QigongDocument4 pagesYan Xin QigongAruna Bandara100% (2)
- Analysis of A Phobia in A Five-Year-Old BoyDocument22 pagesAnalysis of A Phobia in A Five-Year-Old BoyLian Michael100% (1)
- The Maximization of Exposure TherapyDocument12 pagesThe Maximization of Exposure TherapyAuroraNo ratings yet
- Presentation On Hiatal HerniaDocument37 pagesPresentation On Hiatal HerniaRaju Shrestha100% (2)