You might also like
- Natacha-Full CutDocument96 pagesNatacha-Full CutMaru Apostolu88% (25)
- Plabverse AllDocument316 pagesPlabverse AllFahad IqbalNo ratings yet
- Basic EKG Review: Identify Rhythms & InterventionsDocument31 pagesBasic EKG Review: Identify Rhythms & Interventionsmeb100% (1)
- PALS Pre-course Self-Assessment GuideDocument20 pagesPALS Pre-course Self-Assessment GuideLawrence Gabriel80% (5)
- Renato Canova Development of Strengthy EnduranceDocument12 pagesRenato Canova Development of Strengthy EnduranceDarwins Mendoza100% (1)
- Handbook of AnesthesiologyDocument176 pagesHandbook of AnesthesiologyarmelzahfauziNo ratings yet
- Pha CPR Bls Acls Manual 2012 Edited (08 25 2012)Document30 pagesPha CPR Bls Acls Manual 2012 Edited (08 25 2012)Gene Alfonso BanawaNo ratings yet
- Renal Nutrition Management Protocol 2015 PDFDocument27 pagesRenal Nutrition Management Protocol 2015 PDFShefali RawatNo ratings yet
- 2nd Case Session ToT CPG HPTDocument127 pages2nd Case Session ToT CPG HPThakimahsNo ratings yet
- Intensive Care Unit (ICU) Manual 2020-21Document146 pagesIntensive Care Unit (ICU) Manual 2020-21anithaNo ratings yet
- Aki and CKD Therapy 2021Document46 pagesAki and CKD Therapy 2021Alfathri YunediNo ratings yet
- 205 Management of Hypo Kala Emi ADocument11 pages205 Management of Hypo Kala Emi AGresonNo ratings yet
- Hipertensi 2Document43 pagesHipertensi 2Sri AfniNo ratings yet
- Oleh: Bagian Ilmu Penyakit Dalam FK Universitas Sultan Agung Semarang 2012Document40 pagesOleh: Bagian Ilmu Penyakit Dalam FK Universitas Sultan Agung Semarang 2012Mbenk NjoeNo ratings yet
- Farmakoterapi Sistem Endokrin: Tim Dosen Farmasi KlinikDocument42 pagesFarmakoterapi Sistem Endokrin: Tim Dosen Farmasi KlinikAnonymous h76WT2cFdkNo ratings yet
- Sec1 Clinical2 (ARF)Document44 pagesSec1 Clinical2 (ARF)ahmedmohamed01153159469No ratings yet
- Pharmacological-Management-of-HypertensionDocument35 pagesPharmacological-Management-of-Hypertensiontf.almutairi88No ratings yet
- สำเนา draft1 - DKA 1Document42 pagesสำเนา draft1 - DKA 1teddypor100% (1)
- Saint Louis University College of Nursing Baguio CityDocument10 pagesSaint Louis University College of Nursing Baguio CityrenleanNo ratings yet
- Hypertension I: by Ph. Sarah T. OmranDocument34 pagesHypertension I: by Ph. Sarah T. OmranMoataz MansourNo ratings yet
- Management-APSGN 2Document2 pagesManagement-APSGN 2Fernando AnibanNo ratings yet
- Cad CommerDocument2 pagesCad CommerWhatDoYouSeriesNo ratings yet
- Secondary Prevention SlideDocument14 pagesSecondary Prevention Slideagungnugoho4247No ratings yet
- IRIS 2009 Treatment Recommendations SummaryDocument5 pagesIRIS 2009 Treatment Recommendations SummaryJessicaHernandezNo ratings yet
- Endocrinology - Review NotesDocument9 pagesEndocrinology - Review NotesRoa Al-SajjanNo ratings yet
- Case StudyDocument12 pagesCase StudyJerard VismanosNo ratings yet
- Farmakoterapi Terapan HipertensiDocument48 pagesFarmakoterapi Terapan HipertensiAini SavitriNo ratings yet
- CPT Group 5 Section DDocument83 pagesCPT Group 5 Section DLinus WerkeNo ratings yet
- Medical Check Up Standard Operating Procedure For Diagnosis 1. BMIDocument25 pagesMedical Check Up Standard Operating Procedure For Diagnosis 1. BMIlita agustinNo ratings yet
- CVD Prevention and Rehabilitation Programmes/TITLEDocument97 pagesCVD Prevention and Rehabilitation Programmes/TITLEMITHANo ratings yet
- Diabetic Ketoacidosis (Dka)Document16 pagesDiabetic Ketoacidosis (Dka)yazid100% (5)
- Admission and Discharge Criteria AccuDocument4 pagesAdmission and Discharge Criteria Accusanisani1020No ratings yet
- Prof - Dr.Medhat Ashmawy Professor of Cardiology, Tanta UniversityDocument104 pagesProf - Dr.Medhat Ashmawy Professor of Cardiology, Tanta UniversityThe department of cardiovascular medicineNo ratings yet
- Management of diabetic ketoacidosis: principles of management in the first hourDocument13 pagesManagement of diabetic ketoacidosis: principles of management in the first hourAzim Abd Razak100% (1)
- Case Study For HypertensionDocument9 pagesCase Study For HypertensionGabbii Cinco100% (1)
- Digoxin Drug CardDocument1 pageDigoxin Drug CardMahsa Ahmadzadeh100% (2)
- JNC 7 (Klasifikasi Hipertensi) PDFDocument2 pagesJNC 7 (Klasifikasi Hipertensi) PDFAbdur RahmanNo ratings yet
- Farmakologi 1 Antihypertension: NURUL HASANAH (1800085)Document31 pagesFarmakologi 1 Antihypertension: NURUL HASANAH (1800085)MutiaraBintangNo ratings yet
- 1 Pharmacology of hypertension and hypotensionDocument110 pages1 Pharmacology of hypertension and hypotensiongostrider0093sNo ratings yet
- Medication Hypertension OlaDocument13 pagesMedication Hypertension OlaNoor AliNo ratings yet
- 12 - Diabetic Emergencies-DKADocument13 pages12 - Diabetic Emergencies-DKABalqis AqisNo ratings yet
- Management of Diabetes Emergencies''Document85 pagesManagement of Diabetes Emergencies''Princewill SeiyefaNo ratings yet
- Nursing Management OF A Patient With HypertensionDocument39 pagesNursing Management OF A Patient With HypertensionJEEJANo ratings yet
- Case Report 1: Hypertension: School of Pharmaceutical SciencesDocument17 pagesCase Report 1: Hypertension: School of Pharmaceutical SciencesMuslihah RaffliNo ratings yet
- Hypertension: Silent KillerDocument28 pagesHypertension: Silent KilleribratiNo ratings yet
- Acute Hyperkalaemia in AdultsDocument12 pagesAcute Hyperkalaemia in AdultsMeilina FitrianiNo ratings yet
- MRCP Part 1Document38 pagesMRCP Part 1走过一些路No ratings yet
- Management of Heart Failure: OutlineDocument27 pagesManagement of Heart Failure: OutlineBoetik AlifiaNo ratings yet
- Acute Decompensated Heart FailureDocument31 pagesAcute Decompensated Heart Failure568563No ratings yet
- The Cardiovascular System: Classification of AntihypertensivesDocument57 pagesThe Cardiovascular System: Classification of AntihypertensivesDr. Hashibu SsekweyamaNo ratings yet
- Treatment of Lipid Disorders-SchubartDocument76 pagesTreatment of Lipid Disorders-SchubartOliver OwuorNo ratings yet
- Dr. Endah Dewati K.S. SPJPDocument41 pagesDr. Endah Dewati K.S. SPJPbudiantoNo ratings yet
- Hypertension: Pathophysiology, Diagnostic Test, Medical Management, and Nursing Care PlanDocument12 pagesHypertension: Pathophysiology, Diagnostic Test, Medical Management, and Nursing Care PlanMaulidyaFadilahNo ratings yet
- Type 2 Diabetes Mellitus Case StudyDocument9 pagesType 2 Diabetes Mellitus Case StudyMike CoolNo ratings yet
- UNSW Medicine GP Management Vivas: Lawson Ung UNSW VI 2015Document41 pagesUNSW Medicine GP Management Vivas: Lawson Ung UNSW VI 2015hernandez2812No ratings yet
- Primary Care Guidelines For The Treatment of Chronic Stable Angina PectorisDocument8 pagesPrimary Care Guidelines For The Treatment of Chronic Stable Angina PectoriserhaarahmiNo ratings yet
- Understanding the Causes and Treatment of HypokalemiaDocument40 pagesUnderstanding the Causes and Treatment of HypokalemiaNadila Putri100% (1)
- LithiumDocument4 pagesLithiumapi-3797941100% (1)
- Salisbury 1100 Harrison PDFDocument62 pagesSalisbury 1100 Harrison PDFDrNaveen Singh Rajpurohit KaduNo ratings yet
- Ketogenic Diet "Yes & No" Guide For BeginnersFrom EverandKetogenic Diet "Yes & No" Guide For BeginnersRating: 3 out of 5 stars3/5 (1)
- Diabetic Recipes for One and TwoFrom EverandDiabetic Recipes for One and TwoRating: 3 out of 5 stars3/5 (1)
- Discover The Best Exercises For Overall Health & Longevity - Based On The Teachings Of Dr. Andrew Huberman: The Ultimate Workout Guide For Lifelong Well-BeingFrom EverandDiscover The Best Exercises For Overall Health & Longevity - Based On The Teachings Of Dr. Andrew Huberman: The Ultimate Workout Guide For Lifelong Well-BeingNo ratings yet
- Exercise and Diabetes: A Clinician's Guide to Prescribing Physical ActivityFrom EverandExercise and Diabetes: A Clinician's Guide to Prescribing Physical ActivityNo ratings yet
- Healing Diabetes Type 2: Discover How To Achieve Remission With Healthy, Simple And Practical Changes In Your LifestyleFrom EverandHealing Diabetes Type 2: Discover How To Achieve Remission With Healthy, Simple And Practical Changes In Your LifestyleNo ratings yet
- 11 Books That Changed an Athlete's Life and PerformanceDocument4 pages11 Books That Changed an Athlete's Life and PerformanceGrace McConnochieNo ratings yet
- Two Years.: WWW - Legislation.gov - au/Series/F2011L02716Document2 pagesTwo Years.: WWW - Legislation.gov - au/Series/F2011L02716Grace McConnochieNo ratings yet
- The Female Athlete Triad: Detection, Treatment & PreventionDocument57 pagesThe Female Athlete Triad: Detection, Treatment & PreventionGrace McConnochieNo ratings yet
- Peak PerformanceDocument6 pagesPeak PerformanceGrace McConnochieNo ratings yet
- Strength RoutinesDocument3 pagesStrength RoutinesGrace McConnochieNo ratings yet
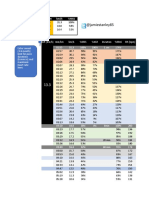
- @jamiestanley85: Duration Min/Km KM/H %mss 1 Sec Mss 6 Min Vvo2Peak/Mas 60 Min Vlt2 HrmaxDocument4 pages@jamiestanley85: Duration Min/Km KM/H %mss 1 Sec Mss 6 Min Vvo2Peak/Mas 60 Min Vlt2 HrmaxGrace McConnochieNo ratings yet
- Moses Mosop's 2:05:51 marathon debut at BostonDocument4 pagesMoses Mosop's 2:05:51 marathon debut at BostonGrace McConnochieNo ratings yet
- Chap22 PDFDocument9 pagesChap22 PDFSam CryshnaNo ratings yet
- Understanding Arrhythmias: Causes, Types, and TreatmentsDocument40 pagesUnderstanding Arrhythmias: Causes, Types, and TreatmentsYolanda SimamoraNo ratings yet
- 2021 - Elbokl - Severe Caffeine Intoxication Treated With HemodialysisDocument4 pages2021 - Elbokl - Severe Caffeine Intoxication Treated With Hemodialysisamanda lssNo ratings yet
- EKG Quick Reference ChartDocument4 pagesEKG Quick Reference ChartMildaNo ratings yet
- Manage arrhythmia with shared care agreementDocument3 pagesManage arrhythmia with shared care agreementNavojit ChowdhuryNo ratings yet
- EKG Nclex High YieldDocument13 pagesEKG Nclex High Yieldnene lewis100% (1)
- Manouver VagalDocument8 pagesManouver VagalAnna Andany100% (1)
- ACLS Written 2006 Precourse Self AssessmentDocument14 pagesACLS Written 2006 Precourse Self AssessmentmonickamsNo ratings yet
- Arritmias en El EmbarazoDocument10 pagesArritmias en El EmbarazoJuan Soto FarfanNo ratings yet
- What Is A Cardiac Dysrhythmia?Document6 pagesWhat Is A Cardiac Dysrhythmia?Megan N. ReyesNo ratings yet
- Approach To ACLS RhythmDocument150 pagesApproach To ACLS RhythmChristine Bernadette Rapal Bollong100% (2)
- DR Kupe - ECGDocument14 pagesDR Kupe - ECGIrfan ZiadNo ratings yet
- Ecg NotesDocument35 pagesEcg NotesDanielle100% (1)
- PDF Rigel PatSim 200Document5 pagesPDF Rigel PatSim 200Eliel VelasquezNo ratings yet
- (HeartSim 200 DfU) - 982Document86 pages(HeartSim 200 DfU) - 982edgargadoNo ratings yet
- Emergency Cardiovascular Life SupportDocument88 pagesEmergency Cardiovascular Life SupportMARK JOSHUA CRUZNo ratings yet
- Amiodarone IV Administration 1.0Document5 pagesAmiodarone IV Administration 1.0Ari BinkosimNo ratings yet
- POTS Mecanismos FisiopatologicosDocument16 pagesPOTS Mecanismos FisiopatologicosAlfredoNo ratings yet
- NCORT Book PDFDocument66 pagesNCORT Book PDFSintoun100% (2)
- Electrophysiology of the Heart and Arrhythmia TreatmentDocument42 pagesElectrophysiology of the Heart and Arrhythmia TreatmentKrakenzeN100% (1)
- Prof. Randa Cardiac ArrhythmiasDocument57 pagesProf. Randa Cardiac ArrhythmiasMohan MadhavanNo ratings yet
- EKG InterpretationDocument63 pagesEKG InterpretationMiriam Cindy MathullaNo ratings yet
- ECG For OsceDocument69 pagesECG For OsceElenaCNo ratings yet
- ECG Learning ModulesDocument150 pagesECG Learning ModulesdodiNo ratings yet
- Ecgs Made Easy 5th Edition Aehlert Test BankDocument14 pagesEcgs Made Easy 5th Edition Aehlert Test BankQuinn50% (2)