You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Ivt Form2Document2 pagesIvt Form2Ina Patricia ErjasNo ratings yet
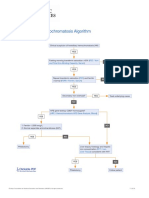
- Hereditary Hemochromatosis AlgorithmDocument1 pageHereditary Hemochromatosis AlgorithmS6b2No ratings yet
- Female Sterilisation: Presented by Group 4Document23 pagesFemale Sterilisation: Presented by Group 4IbrahimWagesNo ratings yet
- ExamView - Chapter - 33 PDFDocument8 pagesExamView - Chapter - 33 PDFChizua OkoyeNo ratings yet
- Chapter 14 Electrolyte Imbalances-1Document8 pagesChapter 14 Electrolyte Imbalances-1SITTIE JOBAISAH TOMINAMAN ALINo ratings yet
- CDI Physician Query For CHFDocument1 pageCDI Physician Query For CHFMuskegPressNo ratings yet
- Management of Patients With Special NeedsDocument4 pagesManagement of Patients With Special NeedsSophia MolinaNo ratings yet
- Gingivitis EnglishDocument4 pagesGingivitis EnglishverenNo ratings yet
- Health Education On DMDocument12 pagesHealth Education On DMAnand Bhawna100% (6)
- 2nd Patho Exam QDocument17 pages2nd Patho Exam QSaleh RazickNo ratings yet
- OET Reading - OsteoporosisDocument8 pagesOET Reading - OsteoporosisPradeep PaudelNo ratings yet
- Medications Commonly Prescribed After A Stroke - GoodRxDocument11 pagesMedications Commonly Prescribed After A Stroke - GoodRxAnonymous EAPbx6No ratings yet
- Nursing Quiz Topic GlaucomaDocument3 pagesNursing Quiz Topic GlaucomaChieChay Dub100% (1)
- Pedia+smiley Block7Document7 pagesPedia+smiley Block7tej0331No ratings yet
- Diagnosa DokterDocument1 pageDiagnosa Dokteranton nioNo ratings yet
- Imse Finals Reviewer - Pacate, Joyce C.Document9 pagesImse Finals Reviewer - Pacate, Joyce C.jcpacate1178qcNo ratings yet
- KEGIATAN SELESAI Secondary AdminCCADocument22 pagesKEGIATAN SELESAI Secondary AdminCCAAizawanda ReNo ratings yet
- Clinical Significance of Antinuclear Antibody Staining Patterns and Associated Autoantibodies - UpToDateDocument13 pagesClinical Significance of Antinuclear Antibody Staining Patterns and Associated Autoantibodies - UpToDateMelanie NgNo ratings yet
- Acute and Chronic Otitis MediaDocument32 pagesAcute and Chronic Otitis MediaAndrew KaumbaNo ratings yet
- Bmi Monitoring SheetDocument13 pagesBmi Monitoring SheetMaricel Ang BajeyoNo ratings yet
- Management of The Open Abdomen in Adults - UpToDateDocument30 pagesManagement of The Open Abdomen in Adults - UpToDatexcarlosfxNo ratings yet
- WFNS Neuroanatomy Committee 3rd WebinarDocument4 pagesWFNS Neuroanatomy Committee 3rd WebinarhalikalifhayaNo ratings yet
- Module 2 PE01Document17 pagesModule 2 PE01chingNo ratings yet
- Abortion - The Expulsion of A Fetus From The Uterus Before It Has Reached TheDocument2 pagesAbortion - The Expulsion of A Fetus From The Uterus Before It Has Reached TheRomelyn AngelNo ratings yet
- CPG - Pneumonia (2010 Update)Document55 pagesCPG - Pneumonia (2010 Update)Jade Kenneth Gonzales LomansocNo ratings yet
- Drug Study GalaponDocument4 pagesDrug Study GalaponSheryl DiazNo ratings yet
- Septicemia NewDocument3 pagesSepticemia NewkainatNo ratings yet
- MODULE 8A: IV Fluid Principles: Dengue Clinical ManagementDocument25 pagesMODULE 8A: IV Fluid Principles: Dengue Clinical Managemented seraficaNo ratings yet
- MAPEH 8 Third Periodical TestDocument3 pagesMAPEH 8 Third Periodical TestAntis VergelNo ratings yet
- Getahun Mengistu, MD, MSC, Internist, Neurologist & Specialist in Headache Medicine, Department of Neurology, AAU-MFDocument85 pagesGetahun Mengistu, MD, MSC, Internist, Neurologist & Specialist in Headache Medicine, Department of Neurology, AAU-MFashuNo ratings yet