You might also like
- DSM-IV ADHD Symptom Checklist-Child and Adolescent Version # 6177Document1 pageDSM-IV ADHD Symptom Checklist-Child and Adolescent Version # 6177Chris100% (2)
- Cestodes TableDocument3 pagesCestodes TableSuha AbdullahNo ratings yet
- Parasitology Guide Questions 1Document2 pagesParasitology Guide Questions 1Cess LacatangoNo ratings yet
- Sample Preservation - UrineDocument1 pageSample Preservation - UrinedewkmcNo ratings yet
- Best Practices For Sample Storage UrineDocument41 pagesBest Practices For Sample Storage UrinekinnusaraiNo ratings yet
- Swu Phinma, College of Pharmacy 2020: Wr/Urinalysis - Html#Ixzz6Zxlj RQKH /Product-Manual/3008 - 3B - UrinalysisDocument7 pagesSwu Phinma, College of Pharmacy 2020: Wr/Urinalysis - Html#Ixzz6Zxlj RQKH /Product-Manual/3008 - 3B - UrinalysisTrex MarciiiNo ratings yet
- Purf Brief 1Document61 pagesPurf Brief 1Prabhavathy KannappanNo ratings yet
- Enzyme Purification NotesDocument23 pagesEnzyme Purification NotesMadan Rajan100% (1)
- Cytology in Food Animal PracticeDocument37 pagesCytology in Food Animal PracticeborradorcitoNo ratings yet
- I. OBJECTIVE: To Learn The Correct Techniques of Collecting, Packing, and Preserving SpecimensDocument4 pagesI. OBJECTIVE: To Learn The Correct Techniques of Collecting, Packing, and Preserving SpecimensJR VALDEZNo ratings yet
- FMNH Disease-Based Sampling Suggestions-2Document9 pagesFMNH Disease-Based Sampling Suggestions-2api-258655506No ratings yet
- PMLS 2 Chapter Summary - YraudaDocument5 pagesPMLS 2 Chapter Summary - YraudaKeizzy YraudaNo ratings yet
- UrinalysisDocument172 pagesUrinalysisRonelene GatoNo ratings yet
- Macroscopic Urinalysis, Performed Manually Using Bayer MultistixDocument12 pagesMacroscopic Urinalysis, Performed Manually Using Bayer MultistixKevin TranNo ratings yet
- Collection of stool specimens for parasitology analysisDocument10 pagesCollection of stool specimens for parasitology analysisOmar ElabdNo ratings yet
- New Concepts in Daignosis and Therapy of Repeat BreedingDocument7 pagesNew Concepts in Daignosis and Therapy of Repeat BreedinggnpobsNo ratings yet
- Laboratory Assessment of Nutritional StatusDocument15 pagesLaboratory Assessment of Nutritional StatusAdar LázaroNo ratings yet
- Fetal Bovine Serum - Atlanta BiologicalsDocument4 pagesFetal Bovine Serum - Atlanta BiologicalsRavikiran GNo ratings yet
- (Osborn) Chapter 62: Learning Outcomes (Number and Title)Document23 pages(Osborn) Chapter 62: Learning Outcomes (Number and Title)KittiesNo ratings yet
- Lab 7 Non Blood Specimens Part 2Document43 pagesLab 7 Non Blood Specimens Part 2Mica BernardoNo ratings yet
- Cytogenetics Lecture Notes - SOPDocument23 pagesCytogenetics Lecture Notes - SOPNeo Mervyn Monaheng100% (1)
- PAA CellCultureMediaDocument20 pagesPAA CellCultureMediaNilabh Ranjan100% (1)
- Clinical Microscopy Technical ManualDocument10 pagesClinical Microscopy Technical ManualSharon ChuaNo ratings yet
- 2.TEACHERKidneyProblem7 23 09Document18 pages2.TEACHERKidneyProblem7 23 09Paijo SusenoNo ratings yet
- Tissue Culture ThesisDocument5 pagesTissue Culture ThesisBestPaperWritersKansasCity100% (2)
- Research Papers On Animal Tissue CultureDocument6 pagesResearch Papers On Animal Tissue Cultureqampxcwhf100% (1)
- Bence JonesDocument5 pagesBence JonesChristian Eduard de Dios100% (1)
- Principle:: Sample Considerations and Special ProceduresDocument97 pagesPrinciple:: Sample Considerations and Special Proceduresjustine anchetaNo ratings yet
- PROPER COLLECTION AND PRESERVATION OF STOOL SAMPLESDocument6 pagesPROPER COLLECTION AND PRESERVATION OF STOOL SAMPLESDavid SantosNo ratings yet
- Animal Cell CulturesDocument52 pagesAnimal Cell CulturesGanga RasanjaleeNo ratings yet
- Enm 32 18 PDFDocument5 pagesEnm 32 18 PDFSofia andrea MezaNo ratings yet
- PHD Thesis Cell CultureDocument5 pagesPHD Thesis Cell Culturefc4qgsp7100% (2)
- Understanding Anti-Müllerian Hormone (AMH) LevelsDocument47 pagesUnderstanding Anti-Müllerian Hormone (AMH) LevelsJerry TjoanatanNo ratings yet
- Impact of Oxygenation of Bioartificial Liver Using Perfluorocarbon Emulsion Perftoran On Metabolism of Human Hepatoma C3A CellsDocument11 pagesImpact of Oxygenation of Bioartificial Liver Using Perfluorocarbon Emulsion Perftoran On Metabolism of Human Hepatoma C3A CellsIstván PortörőNo ratings yet
- Stool Exam Methods - Detect Parasites with AccuracyTITLE Diagnosing Parasites in Stool - Laboratory Techniques Explained TITLE Parasite Detection in Stool - Proper Collection and Examination MethodsDocument27 pagesStool Exam Methods - Detect Parasites with AccuracyTITLE Diagnosing Parasites in Stool - Laboratory Techniques Explained TITLE Parasite Detection in Stool - Proper Collection and Examination MethodsAnastasiaNo ratings yet
- Marquez - Laboratory Research WorkDocument3 pagesMarquez - Laboratory Research WorkAyuhmi MarquezNo ratings yet
- Detect Pathogens and Parasites in StoolDocument8 pagesDetect Pathogens and Parasites in StoolPraveen KumarNo ratings yet
- Analisis Sampel Biologis Untuk Pengujian DopingDocument34 pagesAnalisis Sampel Biologis Untuk Pengujian DopingYuan Achda ArbineryNo ratings yet
- PRESENTATION BPDocument58 pagesPRESENTATION BPBishnupriya SahaNo ratings yet
- Protein extraction and quantification from various organisms using Bradford AssayDocument5 pagesProtein extraction and quantification from various organisms using Bradford AssayBrandon Lam100% (1)
- Proteinuria en Perros y GatosDocument16 pagesProteinuria en Perros y GatosKaren PMNo ratings yet
- Exercise 11: Fecal Occult Blood Test: Points: 20 ObjectivesDocument9 pagesExercise 11: Fecal Occult Blood Test: Points: 20 ObjectivesMarkNo ratings yet
- Body FluidsDocument52 pagesBody Fluidskwon hoshiNo ratings yet
- Routine UrinalysisDocument4 pagesRoutine UrinalysisEricka Zai FLORESNo ratings yet
- 1856-Cian - The Role of Cytology in Urinalysis of Dogs and CaDocument4 pages1856-Cian - The Role of Cytology in Urinalysis of Dogs and CaYaiza Garcia CasadoNo ratings yet
- Lovely Professional: Topic:Western BlottingDocument16 pagesLovely Professional: Topic:Western BlottingVikal RajputNo ratings yet
- Thesis On Single Cell ProteinDocument4 pagesThesis On Single Cell Proteinjessicatannershreveport100% (2)
- Macleod 1Document8 pagesMacleod 1rakibhossainNo ratings yet
- Wilson's Disease Case StudyDocument3 pagesWilson's Disease Case StudyKatrina CaveNo ratings yet
- Fecal Analysis (Stool Analysis) Nursing ResponsibilitiesDocument4 pagesFecal Analysis (Stool Analysis) Nursing ResponsibilitiesDonna IlarNo ratings yet
- Urinalysis 1: Mr. Arian Ray E. MalintadDocument55 pagesUrinalysis 1: Mr. Arian Ray E. MalintadAbraham DemeterioNo ratings yet
- Urine Analysis ExplainedDocument22 pagesUrine Analysis Explainedsvrlax60% (5)
- Assignment For Finals Forensic ChemDocument6 pagesAssignment For Finals Forensic ChemLopez Marc JaysonNo ratings yet
- Antibody Labeling Fluorescence Micros - Fluorescent Immunocytochemistry Fluorescent Immunohistochem - Indirect Immunocytochemistry ImmunostainingDocument6 pagesAntibody Labeling Fluorescence Micros - Fluorescent Immunocytochemistry Fluorescent Immunohistochem - Indirect Immunocytochemistry ImmunostainingDr. Salvador Muñoz BarriosNo ratings yet
- BiopharmingDocument2 pagesBiopharmingRonaldo ChachaNo ratings yet
- Animal Tissue Culture: Topic Landmark Inventions in The Field of Animal Biotechnology and Their ImportanceDocument12 pagesAnimal Tissue Culture: Topic Landmark Inventions in The Field of Animal Biotechnology and Their ImportanceAkshay MankotiaNo ratings yet
- Tissue Culture..Document26 pagesTissue Culture..Hari ShyamNo ratings yet
- Enzymes - Part 2 - Acid Phosphatase, Alkaline Phosphatase, Amylase and Angiotensin-Converting EnzymeDocument9 pagesEnzymes - Part 2 - Acid Phosphatase, Alkaline Phosphatase, Amylase and Angiotensin-Converting EnzymeReman A. AlingasaNo ratings yet
- TaskforceReport GCCP1 Hartung ATLA30Document8 pagesTaskforceReport GCCP1 Hartung ATLA30mia leeNo ratings yet
- Medical Technology - Cytology Section: Job Responsibilities and DutiesDocument2 pagesMedical Technology - Cytology Section: Job Responsibilities and DutiesJoseline SorianoNo ratings yet
- Diagnosis of Brucella: Prepared By: Bahaa Mostafa Kamel 415Document6 pagesDiagnosis of Brucella: Prepared By: Bahaa Mostafa Kamel 415Bahaa ShaabanNo ratings yet
- Cell Biology Assays: ProteinsFrom EverandCell Biology Assays: ProteinsFanny JaulinNo ratings yet
- Uterin InversionDocument8 pagesUterin InversionZahra AlSaif100% (1)
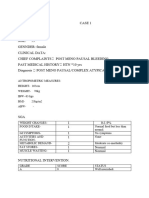
- Case 1Document7 pagesCase 1bsc.clinicalnutrition2018No ratings yet
- PHD Thesis in Prevalence of AsthmaDocument7 pagesPHD Thesis in Prevalence of Asthmabk3q07k5100% (1)
- Liu2011 PDFDocument6 pagesLiu2011 PDFAnonymous cUzAJWocPCNo ratings yet
- Quality of Life After Functional Endoscopic Sinus Surgery in Patients With Chronic RhinosinusitisDocument15 pagesQuality of Life After Functional Endoscopic Sinus Surgery in Patients With Chronic RhinosinusitisNarendraNo ratings yet
- Powders and GranulesDocument18 pagesPowders and GranulesAlaa Salymeh100% (1)
- Test Bank Fundamentals Nursing Care Skills 2nd Edition Ludwig BurtonDocument18 pagesTest Bank Fundamentals Nursing Care Skills 2nd Edition Ludwig Burtontammyshaffer12052000mfe100% (13)
- Unhealthy Vegetable OilsDocument6 pagesUnhealthy Vegetable Oilssmcmo100% (2)
- Durian Technology Package: Growing Guide & Pest ManagementDocument7 pagesDurian Technology Package: Growing Guide & Pest ManagementPutchong Sara100% (1)
- Plum ProductionDocument3 pagesPlum ProductionSharad BhutoriaNo ratings yet
- Avhad (2020), Comparison of Effectiveness of Chlorine Dioxide Mouthwash and Chlorhexidine Gluconate Mouthwash in Reduction of Oral Viral Load in Patients With COVID-19Document6 pagesAvhad (2020), Comparison of Effectiveness of Chlorine Dioxide Mouthwash and Chlorhexidine Gluconate Mouthwash in Reduction of Oral Viral Load in Patients With COVID-19Phuong ThaoNo ratings yet
- Cell - Unit of Life Notes+ EXEDocument95 pagesCell - Unit of Life Notes+ EXEheena lakhwaniNo ratings yet
- Therapeutic Apheresis: Inside The Black BoxDocument70 pagesTherapeutic Apheresis: Inside The Black BoxAhmad Ripani Musyaffa AhdanLabNo ratings yet
- Discuss Thoracic IncisionsDocument47 pagesDiscuss Thoracic IncisionsSucipto HartonoNo ratings yet
- Maintaining Homeostasis: The Coordinated Functions of the Nervous and Endocrine SystemsDocument15 pagesMaintaining Homeostasis: The Coordinated Functions of the Nervous and Endocrine SystemsZahra Alexä DavidsonNo ratings yet
- Nightingale PDFDocument7 pagesNightingale PDFtygitNo ratings yet
- Idiopathic Thrombocytopenic PurpuraDocument45 pagesIdiopathic Thrombocytopenic PurpuraOhnesan Medina PerezNo ratings yet
- TermoresistenciaDocument10 pagesTermoresistenciaIvan SanchezNo ratings yet
- Mini Case Study WeeblyDocument5 pagesMini Case Study Weeblyapi-270446591No ratings yet
- Pre-Intermediate/Intermediate Reading Text: LongevityDocument2 pagesPre-Intermediate/Intermediate Reading Text: LongevityMaria Vitória Carvalho100% (1)
- Medicinal PlantsDocument68 pagesMedicinal PlantsArvind RanganathanNo ratings yet
- Molar PregnancyDocument7 pagesMolar PregnancyFelix Valerian HalimNo ratings yet
- Conscious Sedation Guidelines for DentistsDocument18 pagesConscious Sedation Guidelines for DentistsAnna NgNo ratings yet
- Behavioral ActivationDocument7 pagesBehavioral Activationaastha jain100% (1)
- Toes Flexions Test To Recognize The Functional Status of The Foot Examples of Pathology Knowledge From 1971Document14 pagesToes Flexions Test To Recognize The Functional Status of The Foot Examples of Pathology Knowledge From 1971Athenaeum Scientific PublishersNo ratings yet
- Outpatient InformationDocument2 pagesOutpatient InformationBobdNo ratings yet
- C Difficile SporesDocument3 pagesC Difficile SporesEda SopNo ratings yet