You might also like
- Physician Assistant PANCE & PANRE: a QuickStudy Laminated Reference GuideFrom EverandPhysician Assistant PANCE & PANRE: a QuickStudy Laminated Reference GuideNo ratings yet
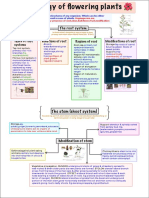
- Morphology of Flowering Plants Mind MapDocument4 pagesMorphology of Flowering Plants Mind MapAstha Agrawal89% (9)
- 4a's DETAILED LESSON PLAN IN SCIENCE 5, 3RD QUARTERDocument9 pages4a's DETAILED LESSON PLAN IN SCIENCE 5, 3RD QUARTERGwyneth Queen GalvadoresNo ratings yet
- (PART-TIME) SIKAP Medical Certificate TemplateDocument1 page(PART-TIME) SIKAP Medical Certificate TemplateIan PalmaNo ratings yet
- Medical School from High School: The College Applicant's Guide to Medical School Early Admission Programs 2Nd EditionFrom EverandMedical School from High School: The College Applicant's Guide to Medical School Early Admission Programs 2Nd EditionNo ratings yet
- Learning Standards Tests: Unit 1 TestDocument5 pagesLearning Standards Tests: Unit 1 TestCaulfield HoldenNo ratings yet
- Cot DressmakingDocument29 pagesCot DressmakingMistekee Maramag100% (1)
- Bond Student GTE Declaration 2019Document4 pagesBond Student GTE Declaration 2019Khawar Abbas BalochNo ratings yet
- PoopDocument2 pagesPoopligma ballzNo ratings yet
- Som-ApplicationDocument10 pagesSom-ApplicationMufti Abdul SohailNo ratings yet
- Application PDFDocument2 pagesApplication PDFBrandon BuchanNo ratings yet
- VF Physical Health DisordersDocument6 pagesVF Physical Health DisordersGuljana SaeedNo ratings yet
- Ien Forms RPT RneducationformDocument10 pagesIen Forms RPT RneducationformGuillermo PalaciosNo ratings yet
- 2) Fellowship Application Form (1) Mod Dr. IVa - For WEBDocument4 pages2) Fellowship Application Form (1) Mod Dr. IVa - For WEBMarisol MorenoNo ratings yet
- Application Receipt: Basic InformationDocument2 pagesApplication Receipt: Basic InformationRainbow Godess500No ratings yet
- Application For Johns Hopkins Clinical ElectiveDocument1 pageApplication For Johns Hopkins Clinical ElectiveOsamah ChoudhryNo ratings yet
- 2018 Immunization Requirements: Frequently Asked QuestionsDocument2 pages2018 Immunization Requirements: Frequently Asked Questionskarlosgwapo3No ratings yet
- Pediatrician Georgia SouthernDocument11 pagesPediatrician Georgia SoutherntiffjandraughnNo ratings yet
- 2023 KOICA - HGU - Masters Degree Program of ICT Policy - Application Form - Updated (230316)Document8 pages2023 KOICA - HGU - Masters Degree Program of ICT Policy - Application Form - Updated (230316)zuhair uddinNo ratings yet
- ResumDocument11 pagesResummmmmder7No ratings yet
- Health Forms Oct. 2019Document10 pagesHealth Forms Oct. 2019andy hanNo ratings yet
- SIKAP Medical Certificate Template Filled OutDocument1 pageSIKAP Medical Certificate Template Filled OutAllen Day100% (1)
- Medical FormDocument2 pagesMedical FormBrury BangetNo ratings yet
- FEDUNI Admission Form 2019Document4 pagesFEDUNI Admission Form 2019Vinicius KostriubaNo ratings yet
- Shabbir, Khadeja (15859782) Myeras ApplicationDocument13 pagesShabbir, Khadeja (15859782) Myeras Applicationmmmmder7No ratings yet
- PGPT Application FormDocument13 pagesPGPT Application FormJACKSON BISANDANo ratings yet
- TMP - 8864 FeeRemission 946582328Document4 pagesTMP - 8864 FeeRemission 946582328varunNo ratings yet
- SNDS Initial Intake FormDocument8 pagesSNDS Initial Intake FormInaam AhmadNo ratings yet
- Medical Fitness Certificate For YourDocument4 pagesMedical Fitness Certificate For Yourvivekkumar s0% (1)
- Application IMPH Program Israel 2012-2013Document6 pagesApplication IMPH Program Israel 2012-2013Habla GuateNo ratings yet
- Uerm MedicineDocument6 pagesUerm MedicineChaim HerreraNo ratings yet
- George Mason University Combined Applicant Declaration Form Dec 2020 - 38498Document3 pagesGeorge Mason University Combined Applicant Declaration Form Dec 2020 - 38498Antara LabibaNo ratings yet
- Application Form: For University Use OnlyDocument6 pagesApplication Form: For University Use OnlyCik IkoNo ratings yet
- Application For Visiting International StudentDocument3 pagesApplication For Visiting International StudentTavishi UsmleNo ratings yet
- Rma ApplicationDocument4 pagesRma ApplicationSanjoy MukherjeeNo ratings yet
- ApplicationDocument2 pagesApplicationbobo outsiderNo ratings yet
- Tsapp 2014Document2 pagesTsapp 2014api-290166419No ratings yet
- Application 2Document2 pagesApplication 2bobo outsiderNo ratings yet
- Training Enrolment FormDocument2 pagesTraining Enrolment Formapi-560204376No ratings yet
- Quaid-I-Azam University Office of The Students' Financial AsistanceDocument5 pagesQuaid-I-Azam University Office of The Students' Financial AsistancebookieNo ratings yet
- NT Intern Application 2011Document4 pagesNT Intern Application 2011Garet JaxNo ratings yet
- UERM - Application FormDocument7 pagesUERM - Application FormDen PabalanNo ratings yet
- APPLICATIONPediatric Radiology Fellowship071911RevisionpdfDocument3 pagesAPPLICATIONPediatric Radiology Fellowship071911RevisionpdfASIK1144No ratings yet
- Medical Certificate: Part-Time Study Under Sikap GrantDocument1 pageMedical Certificate: Part-Time Study Under Sikap GrantSittie Ainna A. UnteNo ratings yet
- Application Form: 1. General InformationDocument3 pagesApplication Form: 1. General InformationGeorge IfeanyichukwuNo ratings yet
- CounselorguideDocument2 pagesCounselorguideapi-230394574No ratings yet
- Observership Application ST - VincentsDocument2 pagesObservership Application ST - Vincentsসোমনাথ মহাপাত্রNo ratings yet
- Application Form - Campus HiringDocument5 pagesApplication Form - Campus HiringDhanu T ANo ratings yet
- Cie A2 Physics 9702 Theory v2 ZnotesDocument7 pagesCie A2 Physics 9702 Theory v2 ZnotesMaashirNo ratings yet
- SIKAP Medical Certificate TemplateDocument2 pagesSIKAP Medical Certificate TemplateRLMNo ratings yet
- Application FormDocument5 pagesApplication FormCambridge2017-2018 Cambridge PrimaryNo ratings yet
- Certification From School Registrar - U-Go ScholarshipDocument1 pageCertification From School Registrar - U-Go ScholarshipDatu DonnavieNo ratings yet
- Application PDFDocument2 pagesApplication PDFDeejay RockyNo ratings yet
- Volunteer Application Form Part 1: Personal DetailsDocument2 pagesVolunteer Application Form Part 1: Personal DetailsskelergrowNo ratings yet
- RSWM MedicalformDocument1 pageRSWM MedicalformAmivi O. TOUVORNo ratings yet
- Immunization Form For New Students: InstructionsDocument2 pagesImmunization Form For New Students: InstructionskamalNo ratings yet
- 1220 - 2009-12-03 CSA UpdateDocument33 pages1220 - 2009-12-03 CSA Updatejim20113No ratings yet
- Intl Medical Student Applicationform Research 07032013Document6 pagesIntl Medical Student Applicationform Research 07032013Mariam A. KarimNo ratings yet
- DVF MedicalDocument5 pagesDVF MedicalkmtateNo ratings yet
- ApplicationDocument2 pagesApplicationl33pageNo ratings yet
- Application Form - Campus HiringDocument5 pagesApplication Form - Campus Hiringpawan khattarNo ratings yet
- Everything You Need To Know About Intakes in USADocument1 pageEverything You Need To Know About Intakes in USAVaishnavi ShahNo ratings yet
- Tos Mapeh 10 1STQDocument3 pagesTos Mapeh 10 1STQDianne Mae DagaNo ratings yet
- Kohler'S Theory of LearningDocument14 pagesKohler'S Theory of LearningVikram RoyNo ratings yet
- UTS - 11555 Masters Architectural Design Thesis - Design, Architecture and Building, UTS HandbookDocument3 pagesUTS - 11555 Masters Architectural Design Thesis - Design, Architecture and Building, UTS HandbookteongNo ratings yet
- Outputs in Career Development: Submitted By: Dahl A. Paalisbo Grade 11-STEM MendelDocument23 pagesOutputs in Career Development: Submitted By: Dahl A. Paalisbo Grade 11-STEM MendelDahl xxNo ratings yet
- Qual Table 1 APADocument4 pagesQual Table 1 APAAlexis BelloNo ratings yet
- Sumera ResumeDocument3 pagesSumera ResumeNew Space EducationNo ratings yet
- English 20 - A Doll's House Final Project: OPTION #1: Marriage Counselor's ReportDocument2 pagesEnglish 20 - A Doll's House Final Project: OPTION #1: Marriage Counselor's ReportFaaz ZubairNo ratings yet
- Mental Illness EssayDocument3 pagesMental Illness EssaygraceNo ratings yet
- Performance Appraisal: The Importance of Rater Training: DSP Dev KumarDocument17 pagesPerformance Appraisal: The Importance of Rater Training: DSP Dev KumarTeddy McNo ratings yet
- University of Lagos Slides LG DesignLab in The MakingDocument32 pagesUniversity of Lagos Slides LG DesignLab in The MakingOmotayo FakinledeNo ratings yet
- Final Demo DLP For CheckingDocument6 pagesFinal Demo DLP For CheckingAimee Joy L HermosoraNo ratings yet
- MOVER V1 ListeningDocument4 pagesMOVER V1 ListeningGiovana RufiniNo ratings yet
- Walking and Jogging Formative AssessmentsDocument2 pagesWalking and Jogging Formative Assessmentsapi-321262957No ratings yet
- Passmore & Rowson - FINAL9Nov18Document18 pagesPassmore & Rowson - FINAL9Nov18Melangell Shirley Roe-Stevens SmithNo ratings yet
- G540 840 InstructionsDocument26 pagesG540 840 Instructions9ioNo ratings yet
- U3L4 Persuasive Essay Assignment 5Document4 pagesU3L4 Persuasive Essay Assignment 5Mili PatelNo ratings yet
- Capf BooklistDocument2 pagesCapf BooklistaniketNo ratings yet
- SAP Business One Is Now Localized in Romania and BulgariaDocument2 pagesSAP Business One Is Now Localized in Romania and Bulgariairinaoprea2No ratings yet
- A Software Reuse Measure Developed at MBA TechnologiesDocument9 pagesA Software Reuse Measure Developed at MBA TechnologiesAdisu JejawNo ratings yet
- Memonia 24357-Article Text-48635-1-10-20210701Document121 pagesMemonia 24357-Article Text-48635-1-10-20210701cosmetikoNo ratings yet
- Personal Business Letter W-EnvDocument2 pagesPersonal Business Letter W-EnvsaadthedamnNo ratings yet
- Bilal Ahmed: Vill& P.O Kuthiala Teh.. Smabrial Dist Sialkot Cell +92-3325767101Document3 pagesBilal Ahmed: Vill& P.O Kuthiala Teh.. Smabrial Dist Sialkot Cell +92-3325767101Rana Muhammad TalhaNo ratings yet
- Non Parametric Chapter 4Document5 pagesNon Parametric Chapter 4Roan Suanque MartirNo ratings yet
- Gujarat Technological UniversityDocument2 pagesGujarat Technological UniversityRahul SharmaNo ratings yet
- Importance of Evaluation in Teaching Learning ProcessDocument10 pagesImportance of Evaluation in Teaching Learning ProcessAnonymous CwJeBCAXpNo ratings yet