You might also like
- Enfermedad CardiovascularDocument7 pagesEnfermedad Cardiovascularvalentina cadena correaNo ratings yet
- Cardiomyopathy in Pregnancy: Jennifer Lewey, MD, and Jennifer Haythe, MDDocument11 pagesCardiomyopathy in Pregnancy: Jennifer Lewey, MD, and Jennifer Haythe, MDAlika MaharaniNo ratings yet
- Physiological Changes in PregnancyDocument7 pagesPhysiological Changes in PregnancyFarid DjafarNo ratings yet
- Pregnancy and Cardiovascular DiseaseDocument14 pagesPregnancy and Cardiovascular DiseaseDuy Nguyen CongNo ratings yet
- Resume Luar Negeri Dita FebriyantiDocument9 pagesResume Luar Negeri Dita FebriyantiDita FebriyantiNo ratings yet
- #Fisiologia CV de Gestante 14-9 PDFDocument7 pages#Fisiologia CV de Gestante 14-9 PDFElizabeth Roxana Canchari LazoNo ratings yet
- Cardiac Diastolic Function After Recovery From Pre-EclampsiaDocument6 pagesCardiac Diastolic Function After Recovery From Pre-EclampsiaLannydchandraNo ratings yet
- Zacharzewski 2019Document6 pagesZacharzewski 2019Ario DaniantoNo ratings yet
- Maternal Physiology and Complications of Multiple PregnancyDocument11 pagesMaternal Physiology and Complications of Multiple PregnancyFafaNo ratings yet
- BMJ Insuficiencia Mitral y Estenosis Ao en EmbarazoDocument4 pagesBMJ Insuficiencia Mitral y Estenosis Ao en EmbarazoSol LakosNo ratings yet
- Cambios Corazon EmbarazoDocument6 pagesCambios Corazon EmbarazoSalvador EsNuNo ratings yet
- Heart Disease and Pregnancy: A Review of Physiological Changes and ManagementDocument17 pagesHeart Disease and Pregnancy: A Review of Physiological Changes and ManagementDuy Nguyen CongNo ratings yet
- Article 10.1111/tog.12599Document8 pagesArticle 10.1111/tog.12599KeeranmayeeishraNo ratings yet
- Trastornos HIPERTENSIVOSDocument14 pagesTrastornos HIPERTENSIVOSIvan CastellanosNo ratings yet
- Physiology 212 Harrison AssignmentDocument3 pagesPhysiology 212 Harrison AssignmentHarrison RumeNo ratings yet
- Medical Resuscitation in Pregnancy: TC, S G, KP O'KDocument11 pagesMedical Resuscitation in Pregnancy: TC, S G, KP O'KEka Umi SuciptoNo ratings yet
- Pi Is 0002937820312837Document13 pagesPi Is 0002937820312837Manuel MagañaNo ratings yet
- Resuscitation in Pregnancy Cardiovascular ChangesDocument5 pagesResuscitation in Pregnancy Cardiovascular ChangesElle ReyesNo ratings yet
- Module 5 Assignment Pregnancy - Maternal ChangesDocument3 pagesModule 5 Assignment Pregnancy - Maternal ChangesAinaB ManaloNo ratings yet
- Reanimacion en La Paciente EmbarazadaDocument13 pagesReanimacion en La Paciente EmbarazadaJerry PowersNo ratings yet
- Maternal Cardiac Output Peaks by 20-24 Weeks and Declines Towards TermDocument9 pagesMaternal Cardiac Output Peaks by 20-24 Weeks and Declines Towards Termaudreynatalia777No ratings yet
- Cardiac output in preeclampsia associated with fetal growth restriction, not gestation onsetDocument12 pagesCardiac output in preeclampsia associated with fetal growth restriction, not gestation onsetHabib Budiman AgungNo ratings yet
- Phenotype-Directed Management of Hypertension in Pregnancy: Contemporary ReviewDocument18 pagesPhenotype-Directed Management of Hypertension in Pregnancy: Contemporary ReviewElmer MoscosoNo ratings yet
- Shock and PregnancyDocument11 pagesShock and Pregnancy101 Andi Dwi Fahria.RNo ratings yet
- Abstrak Makalah Bebas MedanDocument11 pagesAbstrak Makalah Bebas Medandr.raziNo ratings yet
- Chapter 3 - Cardiovascular Disorder and PregnancyDocument3 pagesChapter 3 - Cardiovascular Disorder and Pregnancyeugeniamaranan.06No ratings yet
- Physiology of PregnancyDocument5 pagesPhysiology of PregnancyAlejandra RequesensNo ratings yet
- Adaptacion Fisiologica Cardiorespiratoria Del Embarazo PDFDocument8 pagesAdaptacion Fisiologica Cardiorespiratoria Del Embarazo PDFSusan SuárezNo ratings yet
- TOG 2007 915-20 Review Cardiac Disease in Pregnancy Part 1 CongenitalDocument6 pagesTOG 2007 915-20 Review Cardiac Disease in Pregnancy Part 1 Congenitalsaeed hasan saeedNo ratings yet
- Pi Is 0002937821012175Document18 pagesPi Is 0002937821012175Leslie Tiscareno LaraNo ratings yet
- Cambios Fisiologicos EmbarazoDocument23 pagesCambios Fisiologicos EmbarazoajanethNo ratings yet
- Changes in PregnancyDocument9 pagesChanges in PregnancyFrankRodríguezLuisNo ratings yet
- Heart Disease in Pregnancy: Understanding RisksDocument2 pagesHeart Disease in Pregnancy: Understanding RisksChandra KusumaningtiasNo ratings yet
- PHYSIOLOGY CHANGES DURING PREGNANCYDocument5 pagesPHYSIOLOGY CHANGES DURING PREGNANCYBaiiqDelaYulianingtyasNo ratings yet
- Cardiac ArrestDocument6 pagesCardiac ArrestRhael Denielle SunioNo ratings yet
- Circimaging. 2021Document13 pagesCircimaging. 2021Alejandra PinillaNo ratings yet
- Pregnancy Issues in Women With Atrial Septal Defect: April 2012Document9 pagesPregnancy Issues in Women With Atrial Septal Defect: April 2012Dara Dasawulansari SyamsuriNo ratings yet
- Physiology of Pregnancy: Learning ObjectivesDocument3 pagesPhysiology of Pregnancy: Learning ObjectivesadiNo ratings yet
- Pregnancy as a Cardiac Stress Model: Insights into Physiological AdaptationDocument10 pagesPregnancy as a Cardiac Stress Model: Insights into Physiological AdaptationAlika MaharaniNo ratings yet
- Medical DisordersDocument225 pagesMedical DisordersWael GaberNo ratings yet
- Physiological Changes in Pregnancy: Candice K Silversides, Jack M ColmanDocument12 pagesPhysiological Changes in Pregnancy: Candice K Silversides, Jack M ColmanrinimeimeiNo ratings yet
- 1 s2.0 S2666668521001324 MainDocument5 pages1 s2.0 S2666668521001324 Mainmchojnacki81No ratings yet
- 12 - Jhasnu 19 007Document3 pages12 - Jhasnu 19 007Dila AuNo ratings yet
- Cardiac Disease in PregnancyDocument19 pagesCardiac Disease in PregnancyCarolina Orjuela Camargo0% (1)
- Odontologia EmbarazadaDocument5 pagesOdontologia EmbarazadaDavid Gomez100% (1)
- Hypertension During PregnancyDocument9 pagesHypertension During PregnancyNera MayaditaNo ratings yet
- Uterine and Fetal Placental Doppler Indices Are Associated With Maternal Cardiovascular FunctionDocument8 pagesUterine and Fetal Placental Doppler Indices Are Associated With Maternal Cardiovascular FunctionMuhammad Pebri Nilhakim ZavbmNo ratings yet
- Preeclampsia Maternal Cardiovascular Function and Op - 2022 - Early Human DevelDocument4 pagesPreeclampsia Maternal Cardiovascular Function and Op - 2022 - Early Human DevelJUAN HIMMEL ESPINOZA ANDIANo ratings yet
- Cardiac Disease in PreganacyDocument22 pagesCardiac Disease in PreganacyaberaNo ratings yet
- Cardiac Diseases in Pregnancy-A Review.: K. PushpalathaDocument6 pagesCardiac Diseases in Pregnancy-A Review.: K. PushpalathaBagus Wanda HabibullahNo ratings yet
- Physiology of Pregnancy 2ndDocument61 pagesPhysiology of Pregnancy 2ndLeo SSNo ratings yet
- OB I For 2nd YearDocument122 pagesOB I For 2nd YeardiribaNo ratings yet
- An Integrated Model of Preeclampsia: A Multifaceted Syndrome of The Maternal Cardiovascular-Placental-Fetal ArrayDocument10 pagesAn Integrated Model of Preeclampsia: A Multifaceted Syndrome of The Maternal Cardiovascular-Placental-Fetal Arrayfirman thamrinNo ratings yet
- Beers 2020 ACKD Kidney Physiology in PregnancyDocument6 pagesBeers 2020 ACKD Kidney Physiology in PregnancyBCR ABLNo ratings yet
- Cardiovascular Physiology of PregnancyDocument7 pagesCardiovascular Physiology of PregnancyLyra FebriandaNo ratings yet
- Physiology of PregnancyDocument5 pagesPhysiology of PregnancyLorena Garcia PatiñoNo ratings yet
- Hipertension en El EmbarazoDocument12 pagesHipertension en El EmbarazofsitoNo ratings yet
- Maternal LEC - Week 2 - TransesDocument19 pagesMaternal LEC - Week 2 - TransesEcka- EckaNo ratings yet
- Pre-eclampsia, (Pregnancy with Hypertension And Proteinuria) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandPre-eclampsia, (Pregnancy with Hypertension And Proteinuria) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Jiao 14 1 53 PDFDocument5 pagesJiao 14 1 53 PDFBaiiqDelaYulianingtyasNo ratings yet
- Ent June 2018 21-29 PDFDocument9 pagesEnt June 2018 21-29 PDFBaiiqDelaYulianingtyasNo ratings yet
- 3 - Prem Pal SinghDocument9 pages3 - Prem Pal SinghBaiiqDelaYulianingtyasNo ratings yet
- Referat OmskDocument51 pagesReferat OmskDefri RahmanNo ratings yet
- Ent June 2018 21-29 PDFDocument9 pagesEnt June 2018 21-29 PDFBaiiqDelaYulianingtyasNo ratings yet
- 3 - Prem Pal SinghDocument9 pages3 - Prem Pal SinghBaiiqDelaYulianingtyasNo ratings yet
- Jiao 14 1 53 PDFDocument5 pagesJiao 14 1 53 PDFBaiiqDelaYulianingtyasNo ratings yet
- ACG Guide Achalasia Am - J - Gastroenterol - 2013 - Aug - 108 (8) - 1238 PDFDocument12 pagesACG Guide Achalasia Am - J - Gastroenterol - 2013 - Aug - 108 (8) - 1238 PDFLuis PerazaNo ratings yet
- ACG Guide Achalasia Am - J - Gastroenterol - 2013 - Aug - 108 (8) - 1238 PDFDocument12 pagesACG Guide Achalasia Am - J - Gastroenterol - 2013 - Aug - 108 (8) - 1238 PDFLuis PerazaNo ratings yet
- Diaper RashDocument4 pagesDiaper RashBaiiqDelaYulianingtyasNo ratings yet
- Algo Tachycardia PDFDocument1 pageAlgo Tachycardia PDFYudhistira AdiNo ratings yet
- Algo Tachycardia PDFDocument1 pageAlgo Tachycardia PDFYudhistira AdiNo ratings yet
- PHYSIOLOGY CHANGES DURING PREGNANCYDocument5 pagesPHYSIOLOGY CHANGES DURING PREGNANCYBaiiqDelaYulianingtyasNo ratings yet
- Threatened Abortion A Risk Factor For Poor PregnanDocument8 pagesThreatened Abortion A Risk Factor For Poor PregnanBaiiqDelaYulianingtyasNo ratings yet
- Prevention of Vitamin K Deficiency Bleeding In.26 PDFDocument7 pagesPrevention of Vitamin K Deficiency Bleeding In.26 PDFBaiiqDelaYulianingtyasNo ratings yet
- Corneal Adherent Leukoma Associated With MeaslesDocument3 pagesCorneal Adherent Leukoma Associated With MeaslesBaiiqDelaYulianingtyasNo ratings yet
- 7-Sacrococcygeal Teratoma Management PDFDocument7 pages7-Sacrococcygeal Teratoma Management PDFDidi SudiyatmoNo ratings yet
- Pica and Micronutrient Deficiencies: A Meta-Analysis of the AssociationDocument21 pagesPica and Micronutrient Deficiencies: A Meta-Analysis of the Associationmusyawarah melalaNo ratings yet
- Determinants of Nutritional Anaemia in Children Less Than Five Years AgeDocument6 pagesDeterminants of Nutritional Anaemia in Children Less Than Five Years AgeBaiiqDelaYulianingtyasNo ratings yet
- EPISIOTOMYDocument17 pagesEPISIOTOMYKaye Arriane TenorioNo ratings yet
- GVB 1Document8 pagesGVB 1Aaron SylvestreNo ratings yet
- Characteristics and Guidelines of PublicspaceDocument3 pagesCharacteristics and Guidelines of PublicspaceJanani SurenderNo ratings yet
- OPHTHALDocument8 pagesOPHTHALVarun ChandiramaniNo ratings yet
- Medicinal PlantDocument13 pagesMedicinal PlantNeelum iqbalNo ratings yet
- Copy Resit APLC MiniAssignmentDocument5 pagesCopy Resit APLC MiniAssignmentChong yaoNo ratings yet
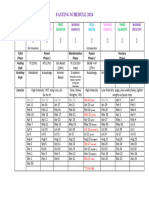
- Moon Fast Schedule 2024Document1 pageMoon Fast Schedule 2024mimiemendoza18No ratings yet
- Presentation 1Document20 pagesPresentation 1nikitakhanduja1304No ratings yet
- Why Islam Is The True Religion in Light of The Quran and SunnahDocument7 pagesWhy Islam Is The True Religion in Light of The Quran and SunnahAsmau DaboNo ratings yet
- Abbreviation Meaning Notes: Cibo ("With Food")Document4 pagesAbbreviation Meaning Notes: Cibo ("With Food")TantriNo ratings yet
- Building Primitive Traps & SnaresDocument101 pagesBuilding Primitive Traps & SnaresJoseph Madr90% (10)
- Serv7107 V05N01 TXT7Document32 pagesServ7107 V05N01 TXT7azry_alqadry100% (6)
- 4 TheEulerianFunctions - 000 PDFDocument16 pages4 TheEulerianFunctions - 000 PDFShorouk Al- IssaNo ratings yet
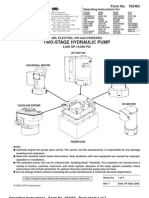
- Power Team PE55 ManualDocument13 pagesPower Team PE55 ManualTitanplyNo ratings yet
- Friction, Gravity and Energy TransformationsDocument12 pagesFriction, Gravity and Energy TransformationsDaiserie LlanezaNo ratings yet
- How Do I Prepare For Public Administration For IAS by Myself Without Any Coaching? Which Books Should I Follow?Document3 pagesHow Do I Prepare For Public Administration For IAS by Myself Without Any Coaching? Which Books Should I Follow?saiviswanath0990100% (1)
- Kltdensito2 PDFDocument6 pagesKltdensito2 PDFPutuWijayaKusumaNo ratings yet
- Astm D 664 - 07Document8 pagesAstm D 664 - 07Alfonso MartínezNo ratings yet
- Masterbatch Buyers Guide PDFDocument8 pagesMasterbatch Buyers Guide PDFgurver55No ratings yet
- Lesson Plan 2 Revised - Morgan LegrandDocument19 pagesLesson Plan 2 Revised - Morgan Legrandapi-540805523No ratings yet
- List of household items for relocationDocument4 pagesList of household items for relocationMADDYNo ratings yet
- Marulaberry Kicad EbookDocument23 pagesMarulaberry Kicad EbookPhan HaNo ratings yet
- Body Shaming Among School Going AdolesceDocument5 pagesBody Shaming Among School Going AdolesceClara Widya Mulya MNo ratings yet
- Airs-Lms - Math-10 - q3 - Week 3-4 Module 3 Rhonavi MasangkayDocument19 pagesAirs-Lms - Math-10 - q3 - Week 3-4 Module 3 Rhonavi MasangkayRamil J. Merculio100% (1)
- ElectricalDocument30 pagesElectricalketerNo ratings yet
- 13Document47 pages13Rohan TirmakheNo ratings yet
- PAPERBOARD QUALITYDocument8 pagesPAPERBOARD QUALITYaurelia carinaNo ratings yet
- Maths SolutionDocument10 pagesMaths SolutionAbhay KumarNo ratings yet
- Hanwha Engineering & Construction - Brochure - enDocument48 pagesHanwha Engineering & Construction - Brochure - enAnthony GeorgeNo ratings yet
- CURRICULUM AUDIT: GRADE 7 MATHEMATICSDocument5 pagesCURRICULUM AUDIT: GRADE 7 MATHEMATICSjohnalcuinNo ratings yet