You might also like
- Soa T TannouryDocument3 pagesSoa T TannourySoumabho DasNo ratings yet
- 2005 Self-Assessment Examination For Residents (Sae-R) : Abridged VersionDocument22 pages2005 Self-Assessment Examination For Residents (Sae-R) : Abridged VersionSoumabho DasNo ratings yet
- Abridged Version: 2002 Self-Assessment Examination For Residents (SAE-R) Answer Key and Commentary On Preferred ChoiceDocument13 pagesAbridged Version: 2002 Self-Assessment Examination For Residents (SAE-R) Answer Key and Commentary On Preferred ChoiceSoumabho DasNo ratings yet
- Co A Volpe 12 16 21Document6 pagesCo A Volpe 12 16 21Soumabho DasNo ratings yet
- EMG TestingDocument50 pagesEMG TestingSoumabho DasNo ratings yet
- 2001 Self-Assessment Examination For Residents (Sae-R) Multiple-Choice Questions Booklet Abridged VersionDocument23 pages2001 Self-Assessment Examination For Residents (Sae-R) Multiple-Choice Questions Booklet Abridged VersionSoumabho DasNo ratings yet
- 2004 SAEanswersDocument12 pages2004 SAEanswersSoumabho DasNo ratings yet
- 2007 AnswersDocument13 pages2007 AnswersSoumabho DasNo ratings yet
- 2002SAEquestions PDFDocument28 pages2002SAEquestions PDFSoumabho Das100% (1)
- Dilution Reconstitution Injection GuideDocument2 pagesDilution Reconstitution Injection GuideSoumabho DasNo ratings yet
- 2008 AnswersDocument16 pages2008 AnswersSoumabho DasNo ratings yet
- 08SAER AbridgedDocument22 pages08SAER AbridgedBabon BaboNo ratings yet
- 9 - Sacral Insufficiency Fracture Repair-SacroplastyDocument7 pages9 - Sacral Insufficiency Fracture Repair-SacroplastySoumabho DasNo ratings yet
- Abridged Version: 2002 Self-Assessment Examination For Residents (SAE-R) Answer Key and Commentary On Preferred ChoiceDocument13 pagesAbridged Version: 2002 Self-Assessment Examination For Residents (SAE-R) Answer Key and Commentary On Preferred ChoiceSoumabho DasNo ratings yet
- 2005 Self-Assessment Examination For Residents (SAE-R) Multiple-Choice Questions Answer Key and Commentary On Preferred ChoiceDocument11 pages2005 Self-Assessment Examination For Residents (SAE-R) Multiple-Choice Questions Answer Key and Commentary On Preferred ChoiceSoumabho DasNo ratings yet
- 2002SAEquestions PDFDocument28 pages2002SAEquestions PDFSoumabho Das100% (1)
- 2001 Self-Assessment Examination For Residents (SAE-R) Multiple-Choice Questions Answer Key and Commentary On Preferred ChoiceDocument11 pages2001 Self-Assessment Examination For Residents (SAE-R) Multiple-Choice Questions Answer Key and Commentary On Preferred ChoiceSoumabho DasNo ratings yet
- 7C - Caudal Epidural Steroid Injection - Ultrasound GuidanceDocument5 pages7C - Caudal Epidural Steroid Injection - Ultrasound GuidanceSoumabho DasNo ratings yet
- 9 - Sacral Insufficiency Fracture Repair-SacroplastyDocument7 pages9 - Sacral Insufficiency Fracture Repair-SacroplastySoumabho DasNo ratings yet
- 8 - Ganglion Impar InjectionDocument1 page8 - Ganglion Impar InjectionSoumabho DasNo ratings yet
- Capgras DelusionDocument1 pageCapgras DelusionSoumabho DasNo ratings yet
- Best Practices For Intrathecal Baclofen Therapy - Dosing and Long-Term ManagementDocument9 pagesBest Practices For Intrathecal Baclofen Therapy - Dosing and Long-Term ManagementSoumabho DasNo ratings yet
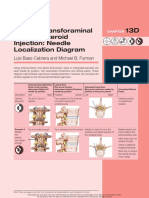
- Lumbar Transforaminal Epidural Steroid Injection: Needle Localization DiagramDocument2 pagesLumbar Transforaminal Epidural Steroid Injection: Needle Localization DiagramSoumabho DasNo ratings yet
- Intrathecal Baclofen PumpDocument19 pagesIntrathecal Baclofen PumpSoumabho DasNo ratings yet
- Best Practices For Intrathecal Baclofen Therapy - Screening TestDocument7 pagesBest Practices For Intrathecal Baclofen Therapy - Screening TestSoumabho DasNo ratings yet
- 2 - Needle TechniquesDocument8 pages2 - Needle TechniquesSoumabho DasNo ratings yet
- Atlas of Muscle Innervation Zones 2012 PDFDocument145 pagesAtlas of Muscle Innervation Zones 2012 PDFSoumabho DasNo ratings yet
- Pump Off Authorization FormDocument1 pagePump Off Authorization FormSoumabho DasNo ratings yet
- Sisters Study 2018Document9 pagesSisters Study 2018Soumabho DasNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Wound CareDocument5 pagesWound CareEdgar Garcia100% (1)
- Nutritional Disorders in Filipino ChildrenDocument9 pagesNutritional Disorders in Filipino ChildrenJill Sanchez-SadiaNo ratings yet
- ObwegeserDocument25 pagesObwegeserR KNo ratings yet
- Biomechanics of The ElbowDocument16 pagesBiomechanics of The ElbowAsmaa Ahmad SharawyNo ratings yet
- 990617 EUS教學 (12) 急診超音波在兒科急症之應用Document67 pages990617 EUS教學 (12) 急診超音波在兒科急症之應用juice119100% (1)
- SVMM Hospital ProjectDocument28 pagesSVMM Hospital ProjectHaindava KeralamNo ratings yet
- Uveitis & Retinal DetachmentDocument8 pagesUveitis & Retinal Detachmentjumi26No ratings yet
- Local Anesthesia in Pediatric DentistryDocument70 pagesLocal Anesthesia in Pediatric DentistryNicky Romeo100% (1)
- Hirschprung Associated EnterocolitisDocument9 pagesHirschprung Associated Enterocolitiskeyla_shineeeNo ratings yet
- ACOG Practice Bulletin No 200 Early Pregnancy.41Document11 pagesACOG Practice Bulletin No 200 Early Pregnancy.41Yty100% (1)
- Pulse OximeterDocument16 pagesPulse OximeterChing Wai Yong100% (1)
- Psycholinguistics ArticulationDocument5 pagesPsycholinguistics ArticulationYoga Permana0% (1)
- Pratice Questions For NCLEX PDFDocument413 pagesPratice Questions For NCLEX PDFEmily97% (29)
- Provider Orientation OnlineDocument72 pagesProvider Orientation OnlinetestNo ratings yet
- 2017 in Handbook Annexure K Form 63 1Document29 pages2017 in Handbook Annexure K Form 63 1K ValdesNo ratings yet
- Newsletter Jan2012Document7 pagesNewsletter Jan2012Slusom WebNo ratings yet
- Pterygium Excision With Free Conjunctival Limbal AutograftDocument7 pagesPterygium Excision With Free Conjunctival Limbal AutograftIOSRjournalNo ratings yet
- Spacers Vs Nebulizers in Children With Acute AsthmaDocument3 pagesSpacers Vs Nebulizers in Children With Acute AsthmaRichard ChandraNo ratings yet
- A To Z Orthodontics Vol 25 Orthodontic MCQDocument113 pagesA To Z Orthodontics Vol 25 Orthodontic MCQelie33% (3)
- 2018 - Voluson Expert BT19 - Probe Guide (July) - JB59717XX PDFDocument4 pages2018 - Voluson Expert BT19 - Probe Guide (July) - JB59717XX PDFBadr Ibrahim Al-QubatiNo ratings yet
- Aad Annualmeeting2011Document398 pagesAad Annualmeeting2011theadlerNo ratings yet
- Medical Act outlines requirements for medical practiceDocument13 pagesMedical Act outlines requirements for medical practiceCornelio AlfonsoNo ratings yet
- Good Practice Upper Intermediate Students Book Sample PagesDocument8 pagesGood Practice Upper Intermediate Students Book Sample PagesAntonio Henriques100% (1)
- Medical Student Elective Book Spring 2020: Updated 08/13/2020Document234 pagesMedical Student Elective Book Spring 2020: Updated 08/13/2020ayeshaNo ratings yet
- HankMed Clinic DramaDocument80 pagesHankMed Clinic Dramapirate85No ratings yet
- Valvular Heart DiseaseDocument32 pagesValvular Heart DiseasefallenczarNo ratings yet
- Carl Misch Workshop Guidelines For Immediate Loading PDFDocument6 pagesCarl Misch Workshop Guidelines For Immediate Loading PDFyogananth100% (1)
- J Neurol Neurosurg Psychiatry 1999 Catsman Berrevoets 755 7Document4 pagesJ Neurol Neurosurg Psychiatry 1999 Catsman Berrevoets 755 7Mihaela LitovcencoNo ratings yet
- Tumbuh Kembang 2013Document42 pagesTumbuh Kembang 2013Siti Fadhilla Tsabitha100% (1)
- Chin 2001Document13 pagesChin 2001zaheerbdsNo ratings yet