You might also like
- The Perfect Bundle For Raising an Explosive Child: Positive Parenting Strategies for Raising an ADHD Child and Teaching Them Life Skills for The Emotional World AheadFrom EverandThe Perfect Bundle For Raising an Explosive Child: Positive Parenting Strategies for Raising an ADHD Child and Teaching Them Life Skills for The Emotional World AheadNo ratings yet
- Handbook of Autism and Pervasive Developmental Disorders, Assessment, Interventions, and PolicyFrom EverandHandbook of Autism and Pervasive Developmental Disorders, Assessment, Interventions, and PolicyNo ratings yet
- CHECKLISTS ON MANIFESTATIONS LWDsDocument5 pagesCHECKLISTS ON MANIFESTATIONS LWDsROWENA MAE FANUNCIONo ratings yet
- LD Screening tool for Teachers: TnDCDocument65 pagesLD Screening tool for Teachers: TnDCDr.V.SivaprakasamNo ratings yet
- Oxford Handbooks Online: Intellectual DisabilitiesDocument20 pagesOxford Handbooks Online: Intellectual DisabilitiesCristina100% (1)
- Management of Childhood and Adolescent DisordersDocument26 pagesManagement of Childhood and Adolescent Disordersdurgesh yadav100% (1)
- 1 - What Is CounsellingDocument27 pages1 - What Is CounsellingveronicaNo ratings yet
- Psychologist Cover LetterDocument1 pagePsychologist Cover Letterapi-256196319No ratings yet
- Ahdh DSM5Document53 pagesAhdh DSM5Sara Araujo100% (1)
- About Case Studies of ADHD in Childre1Document6 pagesAbout Case Studies of ADHD in Childre1PearlCladelLapidezNo ratings yet
- Assessment 2Document8 pagesAssessment 2api-250923807No ratings yet
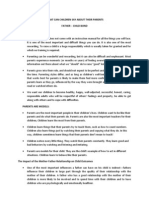
- Importance of the Father-Child Bond and Parental InfluenceTITLEWhat Children Learn from Parents - The Impact of FatherhoodDocument6 pagesImportance of the Father-Child Bond and Parental InfluenceTITLEWhat Children Learn from Parents - The Impact of FatherhoodMarianne Jubille CataquisNo ratings yet
- Conduct Disorder Fact Sheet - K. Elise Parker PDFDocument2 pagesConduct Disorder Fact Sheet - K. Elise Parker PDFepaka02No ratings yet
- Writing Clinical Documents: Objectives, SOAP Notes, and Documentation GuidelinesDocument13 pagesWriting Clinical Documents: Objectives, SOAP Notes, and Documentation GuidelineshotumaNo ratings yet
- Dyslexia BookletN PDFDocument33 pagesDyslexia BookletN PDFDr.V.Sivaprakasam100% (2)
- APA - DSM 5 Diagnoses For Children PDFDocument3 pagesAPA - DSM 5 Diagnoses For Children PDFharis pratamsNo ratings yet
- Initial Clinical Assessment FormDocument10 pagesInitial Clinical Assessment FormOchee De Guzman CorpusNo ratings yet
- Mental Retardation PDFDocument106 pagesMental Retardation PDFSutapa Pawar100% (1)
- Causes and Risk Factors For Attention-Deficit Hyperactivity DisorderDocument8 pagesCauses and Risk Factors For Attention-Deficit Hyperactivity DisorderFranthesa LayloNo ratings yet
- Good Touch-Bad TouchDocument22 pagesGood Touch-Bad Touchyogesh_funde100% (1)
- Referral Checklist for 6-Year-OldsDocument1 pageReferral Checklist for 6-Year-Oldsmarkus_danusantosoNo ratings yet
- Clinical PsychologistDocument3 pagesClinical PsychologisteduardpuiuNo ratings yet
- Pincus Otis Internship Manual 2008Document40 pagesPincus Otis Internship Manual 2008Thien VuNo ratings yet
- Clinical Intake SummaryDocument9 pagesClinical Intake Summaryvaz21No ratings yet
- ADHD Symptom Checklist for DiagnosisDocument1 pageADHD Symptom Checklist for DiagnosisYet Barreda BasbasNo ratings yet
- Aggression QuestionnaireDocument2 pagesAggression QuestionnaireMichelle LanguianNo ratings yet
- Growth and Development: Yarsi School of MedicineDocument32 pagesGrowth and Development: Yarsi School of MedicineLia Noor AnggrainiNo ratings yet
- Child Intake Form (Letter)Document11 pagesChild Intake Form (Letter)Jay Telan IINo ratings yet
- Developmental AssessmentDocument15 pagesDevelopmental AssessmentShailesh MehtaNo ratings yet
- CV For Dr. Keely KolmesDocument9 pagesCV For Dr. Keely KolmesdrkkolmesNo ratings yet
- ASC1Document17 pagesASC1AndyBrookeNo ratings yet
- Chapter 10 Basic Features of Clinical InterventionDocument3 pagesChapter 10 Basic Features of Clinical InterventionKathleenNicole De Castro EnfectanaNo ratings yet
- ASRS-ADHD-self-report-scale-2 2Document2 pagesASRS-ADHD-self-report-scale-2 2Alexys ArchieNo ratings yet
- Functional Behavioral Assessment: Date: - 3/25/20Document5 pagesFunctional Behavioral Assessment: Date: - 3/25/20api-535946620No ratings yet
- Psydclpsy PDFDocument55 pagesPsydclpsy PDFReeshabhdev GauttamNo ratings yet
- M Torres Neuropsychological Report 5Document12 pagesM Torres Neuropsychological Report 5Reyna De AlbaNo ratings yet
- SchizophreniaDocument2 pagesSchizophreniaIT’S ME HAYLA100% (1)
- Relationship Between Premorbid Functioning and Symptom Severity As Assessed at First Episode of PsychosisDocument6 pagesRelationship Between Premorbid Functioning and Symptom Severity As Assessed at First Episode of Psychosisaldrin19No ratings yet
- Case Study 1 Rhonda WilliamsDocument6 pagesCase Study 1 Rhonda Williamsapi-231978749No ratings yet
- Case Conceptualization 514Document4 pagesCase Conceptualization 514Kyle RossNo ratings yet
- Attention Deficit/ Hyperactivity Disorder: Changes To The DisorderDocument2 pagesAttention Deficit/ Hyperactivity Disorder: Changes To The DisorderGemanDuenasNo ratings yet
- Weiss Functional Impairment Rating Scale - Self Report (Wfirs-S)Document2 pagesWeiss Functional Impairment Rating Scale - Self Report (Wfirs-S)Mariana LópezNo ratings yet
- Issues Faced by TherapistDocument2 pagesIssues Faced by TherapistMarianne DalmacioNo ratings yet
- Adhd Symptom ChecklistDocument2 pagesAdhd Symptom Checklistapi-115513756No ratings yet
- Guidelines For Online Conduction of Practical in Ma Psychology Iind Year (Mpce 014/24/34)Document7 pagesGuidelines For Online Conduction of Practical in Ma Psychology Iind Year (Mpce 014/24/34)wonder net0% (1)
- Intake AssessmentDocument2 pagesIntake Assessmentyourzxtruly0% (1)
- ODD Quick Fact Sheet For Parents Guardians and Child Serving Professionals 2.24.14Document2 pagesODD Quick Fact Sheet For Parents Guardians and Child Serving Professionals 2.24.14narcis2009No ratings yet
- FBADocument9 pagesFBANNo ratings yet
- Group Counseling Informed Consent For ParentsDocument1 pageGroup Counseling Informed Consent For Parentsapi-239096806No ratings yet
- Medical report suggests autism diagnosisDocument6 pagesMedical report suggests autism diagnosisSudhansh KumarNo ratings yet
- Guidelines for Assistant PsychologistsDocument14 pagesGuidelines for Assistant Psychologistsricosadie1No ratings yet
- Why Cant Annie Listen and Finish Her WorkDocument8 pagesWhy Cant Annie Listen and Finish Her Workapi-531550324100% (1)
- PSY 3410 Autism Spectrum Disorders & Intellectual DisabilityDocument33 pagesPSY 3410 Autism Spectrum Disorders & Intellectual Disabilityncastro1319No ratings yet
- Psychological Report TemplateDocument11 pagesPsychological Report TemplateSwit AngelzNo ratings yet
- Attention Deficit Hyperactivity Disorder (Adhd)Document43 pagesAttention Deficit Hyperactivity Disorder (Adhd)Thevanath Gunasekaran100% (1)
- Treatment PlanDocument12 pagesTreatment PlanlawamandaNo ratings yet
- DPC Field Report CompletedDocument36 pagesDPC Field Report Completedraman_bhoomi9910No ratings yet
- Abdullah Afnan KanzaDocument3 pagesAbdullah Afnan KanzaKanza Waheed100% (1)
- Cognitive and Behavioral Interventions in the Schools: Integrating Theory and Research into PracticeFrom EverandCognitive and Behavioral Interventions in the Schools: Integrating Theory and Research into PracticeRosemary FlanaganNo ratings yet
- Healing Inside Out And Outside In: Finding Zen through Spriritual HealingFrom EverandHealing Inside Out And Outside In: Finding Zen through Spriritual HealingNo ratings yet
- Clanlands: Sam Heugh A N and GR Aham MctavishDocument27 pagesClanlands: Sam Heugh A N and GR Aham Mctavishnikhila91183% (6)
- Lesson Plan RecyclingDocument6 pagesLesson Plan RecyclingMayerli Janeth Caballero DiazNo ratings yet
- TeachHUB LP Simple Complex and Compound SentencesDocument2 pagesTeachHUB LP Simple Complex and Compound Sentencesnikhila911No ratings yet
- Role of RPD Act for Children with DisabilitiesDocument2 pagesRole of RPD Act for Children with Disabilitiesnikhila911No ratings yet
- Your Free Printable CVC Word Building Mat SetDocument9 pagesYour Free Printable CVC Word Building Mat Setnikhila911No ratings yet
- Art EducationDocument2 pagesArt Educationnikhila911No ratings yet
- The Beast Within - A Tale of Be - Serena Valentino - 2658 PDFDocument210 pagesThe Beast Within - A Tale of Be - Serena Valentino - 2658 PDFAdamNo ratings yet
- Lesson-Plan Volcanoes PDFDocument22 pagesLesson-Plan Volcanoes PDFWillyn Grace Sacasac PacanosNo ratings yet
- The Beast Within - A Tale of Be - Serena Valentino - 2658 PDFDocument210 pagesThe Beast Within - A Tale of Be - Serena Valentino - 2658 PDFAdamNo ratings yet
- t3 G 384 Tectonics A4 Display Poster English - Ver - 4Document1 paget3 G 384 Tectonics A4 Display Poster English - Ver - 4nikhila911No ratings yet
- Ability Grouping Version2Document11 pagesAbility Grouping Version2nikhila911No ratings yet
- Childhood and Growing UpDocument110 pagesChildhood and Growing Uppremkumar1991990No ratings yet
- Food Chain LessonDocument10 pagesFood Chain Lessonnikhila911No ratings yet
- Addition Single Digit NumbersDocument1 pageAddition Single Digit Numbersnikhila911No ratings yet
- D17 FinalDocument148 pagesD17 Finalnikhila911No ratings yet
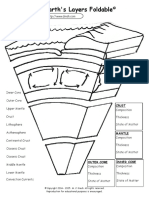
- Earths Layers Foldable 2Document2 pagesEarths Layers Foldable 2nikhila911No ratings yet
- Screening Questionnaire-1Document3 pagesScreening Questionnaire-1nikhila911No ratings yet
- EARLY CHILDHOOD LEARNING AND DEVELOPMENT FACTSDocument113 pagesEARLY CHILDHOOD LEARNING AND DEVELOPMENT FACTSNikhila Joseph100% (1)
- Screening Questionnaire-1Document3 pagesScreening Questionnaire-1nikhila911No ratings yet
- Presentation: The Power of TeamworkDocument14 pagesPresentation: The Power of TeamworkEnrique Sonsona Oliveros jrNo ratings yet
- Parts of Application LetterDocument11 pagesParts of Application LetterDeby Andika Dion HNo ratings yet
- RPH 26 AprilDocument7 pagesRPH 26 Aprilsyeida alliNo ratings yet
- IoT Marketing Partners With Maxwell Pierce Group, LLC For Midwest PSWN DevelopmentDocument2 pagesIoT Marketing Partners With Maxwell Pierce Group, LLC For Midwest PSWN DevelopmentPR.comNo ratings yet
- M1-M5 GuideDocument15 pagesM1-M5 GuideLance SobreviñasNo ratings yet
- Sample Planning DocumentsDocument5 pagesSample Planning Documentsmohitks01_89No ratings yet
- Perencanaan Jadwal KerjaDocument40 pagesPerencanaan Jadwal KerjaSandi Arif FirmansyahNo ratings yet
- Lesson Plan - TransportationsDocument3 pagesLesson Plan - TransportationsRadivan InzmNo ratings yet
- OUMH1403 Course GuideDocument7 pagesOUMH1403 Course GuideAnonymous aGb1BdYLANo ratings yet
- Complaint Text Spam (Unblockin)Document1 pageComplaint Text Spam (Unblockin)Dredd SolimanNo ratings yet
- Bijal Parmar CVDocument2 pagesBijal Parmar CVbijal parmarNo ratings yet
- UMG8900 Documentation GuideDocument34 pagesUMG8900 Documentation Guidegtspaulding100% (1)
- TOEFL Listening Comprehension TipsDocument11 pagesTOEFL Listening Comprehension TipsHusni HabibieNo ratings yet
- College of Accountancy, Business, Economics and International Hospitality Management Bachelor of Science in Business AdministrationDocument2 pagesCollege of Accountancy, Business, Economics and International Hospitality Management Bachelor of Science in Business AdministrationanneNo ratings yet
- Writing and Speaking SummaryDocument23 pagesWriting and Speaking SummaryMelina MohamedNo ratings yet
- Chapter 11Document19 pagesChapter 11THƯ LÊNo ratings yet
- The Relationship of Speech ProductionDocument11 pagesThe Relationship of Speech ProductionYouniverseNo ratings yet
- What Actions Should Yakka Tech Executives Take To Correct These ProblemsDocument3 pagesWhat Actions Should Yakka Tech Executives Take To Correct These ProblemsKhôi Lê VinhNo ratings yet
- Rubrics for Evaluating PresentationsDocument5 pagesRubrics for Evaluating PresentationsShineElefanteEstudilloNo ratings yet
- Jason Schneider Homework - Week 2Document4 pagesJason Schneider Homework - Week 2api-609402637No ratings yet
- Cone of ExperienceDocument42 pagesCone of Experiencekaren rodriguezNo ratings yet
- 2300 Dutch Word Exercises - Rosetta WilkinsonDocument274 pages2300 Dutch Word Exercises - Rosetta WilkinsonVohlaNo ratings yet
- Home TabDocument3 pagesHome TabLaong laanNo ratings yet
- "Retort" From The People, Yes: AnswersDocument2 pages"Retort" From The People, Yes: AnswersabunourNo ratings yet
- Plantilla Agile Team CharterDocument6 pagesPlantilla Agile Team CharterJeimi HerreraNo ratings yet
- Aef 3a 35 38 Can Could BeabletoDocument4 pagesAef 3a 35 38 Can Could BeabletoHugo NhoatoNo ratings yet
- Advertising and Sales PromotionDocument6 pagesAdvertising and Sales PromotionAhmad AlawaddinNo ratings yet
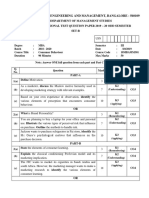
- IA-2 CB Internal QP-2Document2 pagesIA-2 CB Internal QP-2Pradeep BiradarNo ratings yet
- Jesuit Memorial College Mbodo Aluu Port Harcourt: First Continuous Assesment, Second Term 2018/2019 Academic SessionDocument4 pagesJesuit Memorial College Mbodo Aluu Port Harcourt: First Continuous Assesment, Second Term 2018/2019 Academic Sessionk3lvynNo ratings yet
- Imd Ds BrochureDocument2 pagesImd Ds BrochuredimtsekNo ratings yet