You might also like
- 7SanafinallayoutmaidenissueDocument16 pages7SanafinallayoutmaidenissueRannie Rodriguez EspantoNo ratings yet
- Exploring Faculty Preparedness and Capability For Interprofessional LearningDocument1 pageExploring Faculty Preparedness and Capability For Interprofessional LearningSadashiv RahaneNo ratings yet
- Final Report: Development of Clinical Learning Practice Standard For Nursing StudentsDocument10 pagesFinal Report: Development of Clinical Learning Practice Standard For Nursing Studentsbrigitta_bikaNo ratings yet
- Family Medicine Basic CurriculumDocument15 pagesFamily Medicine Basic CurriculumcrubioparraNo ratings yet
- Pilot study explores student perceptions of interprofessional education in the PhilippinesDocument8 pagesPilot study explores student perceptions of interprofessional education in the PhilippinesMada Pasalli SaludungNo ratings yet
- RSA IRR Handbook (28aug2014)Document24 pagesRSA IRR Handbook (28aug2014)oxfordghb123No ratings yet
- UP Manila Brochures 2019-National Teacher Training Center For The Health Professions PDFDocument8 pagesUP Manila Brochures 2019-National Teacher Training Center For The Health Professions PDFKei Sel ZolNo ratings yet
- Interprofessional Educationand CollaborationDocument7 pagesInterprofessional Educationand CollaborationnersrosdianaNo ratings yet
- Improving Assessment in Dental Education Through A Paradigm of Comprehensive Care: A Case ReportDocument13 pagesImproving Assessment in Dental Education Through A Paradigm of Comprehensive Care: A Case ReportfidelbustamiNo ratings yet
- Towards The Development of Core Competencies For Residency Training Coordinators of Family Medicine in The PhilippinesDocument23 pagesTowards The Development of Core Competencies For Residency Training Coordinators of Family Medicine in The PhilippinesTuhin DeyNo ratings yet
- Chapter IiDocument27 pagesChapter IiJohn ReyNo ratings yet
- Implementation Levels of A Life-Skill Based School Health Program in A Caribbean CountryDocument7 pagesImplementation Levels of A Life-Skill Based School Health Program in A Caribbean Countrykhianna dukeNo ratings yet
- Policy Brief Vol. 8 S. 3Document5 pagesPolicy Brief Vol. 8 S. 3Michael Loui SulitNo ratings yet
- Faculty Development CPDDocument6 pagesFaculty Development CPDAida TantriNo ratings yet
- Resource Unit in NHEDocument5 pagesResource Unit in NHEMaria Angelika BughaoNo ratings yet
- Rw-Omj-D-18-00175 (05C)Document6 pagesRw-Omj-D-18-00175 (05C)nersrosdianaNo ratings yet
- USPian Alumni Tracer on 20 Higher Education ProgramsDocument20 pagesUSPian Alumni Tracer on 20 Higher Education ProgramsRandy TabaogNo ratings yet
- The Bachelor of Physical Education Program in Higher Education Institutions Towards The Development of An Enhanced CurriculumDocument13 pagesThe Bachelor of Physical Education Program in Higher Education Institutions Towards The Development of An Enhanced CurriculumGlobal Research and Development Services100% (1)
- Chapter 2 Revice FordaDocument11 pagesChapter 2 Revice Fordajessa faboresNo ratings yet
- Journal ReviewDocument8 pagesJournal ReviewJeuz Yrl LlevaNo ratings yet
- Central Luzon College of Science and Technology Olongapo CityDocument17 pagesCentral Luzon College of Science and Technology Olongapo CityPrince Jhessie L. AbellaNo ratings yet
- ICF: A Hands-on Approach for Clinicians and FamiliesFrom EverandICF: A Hands-on Approach for Clinicians and FamiliesOlaf Kraus de CamargoNo ratings yet
- Outcomes-Based Education Framework for Tarlac State UniversityDocument54 pagesOutcomes-Based Education Framework for Tarlac State UniversityAriane Joyce Villafranca Gara100% (1)
- UA OMSE Med/Ed Enews v3 No. 01 (AUG 2014)Document10 pagesUA OMSE Med/Ed Enews v3 No. 01 (AUG 2014)KC Spear Ellinwood, former Director Instructional DevelopmentNo ratings yet
- Obe PDFDocument6 pagesObe PDFjaycee_evangelistaNo ratings yet
- Chapter 1. Introduction - BHW - Zielabeth M. Conde PDFDocument8 pagesChapter 1. Introduction - BHW - Zielabeth M. Conde PDFLize EdconNo ratings yet
- Document 1management of Nursing Educational InstitutionDocument13 pagesDocument 1management of Nursing Educational InstitutionHardeep Kaur100% (1)
- UA OMSE Med/Ed Enews v2 No. 02 (SEP 2013)Document6 pagesUA OMSE Med/Ed Enews v2 No. 02 (SEP 2013)KC Spear Ellinwood, former Director Instructional DevelopmentNo ratings yet
- MPH Curriculum KU NepalDocument50 pagesMPH Curriculum KU Nepalpreeti A0% (1)
- Manual and Guidelines-ThesisDocument33 pagesManual and Guidelines-ThesisBrd Emmanuel100% (1)
- 1 Legal Bases of EducationDocument12 pages1 Legal Bases of EducationJochris IriolaNo ratings yet
- RM HomeopatheyDocument20 pagesRM HomeopatheyriddhiNo ratings yet
- EDCOM Report by RM Villenes (Proj in EdM514)Document49 pagesEDCOM Report by RM Villenes (Proj in EdM514)Rej Ville88% (8)
- Mphilcp 09Document54 pagesMphilcp 09Noreen ChoudhriNo ratings yet
- Instituto Nacional de Salud Pu Blica: Innovations in Graduate Public Health Education: TheDocument4 pagesInstituto Nacional de Salud Pu Blica: Innovations in Graduate Public Health Education: TheForce MapuNo ratings yet
- CAHE JJ21 Jocelyn B. HiponaDocument11 pagesCAHE JJ21 Jocelyn B. HiponaMicah TuringanNo ratings yet
- AbstractDocument13 pagesAbstractDOH EAMC Healthcare Navigation and ReferralNo ratings yet
- What Is Preservice Education?Document9 pagesWhat Is Preservice Education?Mat GarciaNo ratings yet
- Literature Review On Curriculum DevelopmentDocument15 pagesLiterature Review On Curriculum DevelopmentAbel BucadNo ratings yet
- Curriculum Planning and Development EssentialsDocument106 pagesCurriculum Planning and Development EssentialsRtvc RoldanNo ratings yet
- DOT-syllabus 220130 163901Document19 pagesDOT-syllabus 220130 163901Angkasa LamaNo ratings yet
- Transforming Medical Education To Strengthen The HDocument11 pagesTransforming Medical Education To Strengthen The HsohailurologistNo ratings yet
- 6546 27022 1 PBDocument22 pages6546 27022 1 PBascarolineeNo ratings yet
- Education Assignmnt PERCEPTIVES OF NURSING EDUCATIONDocument13 pagesEducation Assignmnt PERCEPTIVES OF NURSING EDUCATIONSwati SharmaNo ratings yet
- Practices Within A Policy Context Occupational Therapy: Effective School-BasedDocument34 pagesPractices Within A Policy Context Occupational Therapy: Effective School-BasedLondhe AnandNo ratings yet
- Research and Development Management of The Department of Education of Region Iv-A CalabarzonDocument2 pagesResearch and Development Management of The Department of Education of Region Iv-A CalabarzonRico HerreroNo ratings yet
- Finding, Recommendation and Conclusion, Chapter VDocument11 pagesFinding, Recommendation and Conclusion, Chapter VP anditaNo ratings yet
- Tracer Study of PNU GraduatesDocument19 pagesTracer Study of PNU GraduatesMaorin SantosNo ratings yet
- 1 s2.0 S1807593222001119 MainDocument6 pages1 s2.0 S1807593222001119 MainNadiraNo ratings yet
- An Educational Intervention of Interprofessional Learning in Community Based Health Care in Indonesia What Did We Learn From The Pilot StudyDocument12 pagesAn Educational Intervention of Interprofessional Learning in Community Based Health Care in Indonesia What Did We Learn From The Pilot StudyDesvaManurungNo ratings yet
- English Profiency in Colleges Mainly URS in The PhilippinesDocument49 pagesEnglish Profiency in Colleges Mainly URS in The PhilippinesNew GenNo ratings yet
- The Practice of The NursingDocument3 pagesThe Practice of The NursingInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Introduction The National Institute of Child Health and Human DevelopmentDocument2 pagesIntroduction The National Institute of Child Health and Human Developmentshe laNo ratings yet
- A Career Exploration Assignment For First-Year Pharmacy StudentsDocument9 pagesA Career Exploration Assignment For First-Year Pharmacy StudentsYankanagoudaNo ratings yet
- EDITED CHAP 1 5 MAAM JOAN ALFARAS For FinalDocument185 pagesEDITED CHAP 1 5 MAAM JOAN ALFARAS For FinalJoan AlfarasNo ratings yet
- Training Professional Development ExecutiveSummaryDocument8 pagesTraining Professional Development ExecutiveSummaryBoldsuren BishkhorlooNo ratings yet
- Prespective of NSG Edu Global N NationalDocument10 pagesPrespective of NSG Edu Global N NationalAru VermaNo ratings yet
- Gloria Arroyo GalvanDocument10 pagesGloria Arroyo GalvanDee GrayNo ratings yet
- Activity 2 MIlca BSA 3 3Document6 pagesActivity 2 MIlca BSA 3 3kyrie IrvingNo ratings yet
- Pcomm First FinalDocument4 pagesPcomm First Finalkyrie IrvingNo ratings yet
- ER COVID19 Monitoring Form - As Per Labor Advisory 09 s.2020Document2 pagesER COVID19 Monitoring Form - As Per Labor Advisory 09 s.2020jadepatrick misaNo ratings yet
- Week 6 - Exporting in The PhilippinesDocument7 pagesWeek 6 - Exporting in The Philippineskyrie IrvingNo ratings yet
- Pcomm First FinalDocument4 pagesPcomm First Finalkyrie IrvingNo ratings yet
- Are Qualitative' and Quantitative' Useful Terms For Describing Research?Document16 pagesAre Qualitative' and Quantitative' Useful Terms For Describing Research?kyrie IrvingNo ratings yet
- Survey Questionnaire. in Order To Assess The Implementation of Paspas Permit in ValenzuelaDocument2 pagesSurvey Questionnaire. in Order To Assess The Implementation of Paspas Permit in Valenzuelakyrie IrvingNo ratings yet
- MAS Lecture Variable CostingDocument8 pagesMAS Lecture Variable CostingLhoel Delremedios100% (1)
- Course Syllabus AFAR 2 PDFDocument1 pageCourse Syllabus AFAR 2 PDFAmeseah Ross100% (1)
- Manual On Real Property Appraisal AndAssessment OperationsDocument279 pagesManual On Real Property Appraisal AndAssessment OperationsReihannah Paguital-Magno100% (3)
- ER COVID19 Monitoring Form - As Per Labor Advisory 09 s.2020Document2 pagesER COVID19 Monitoring Form - As Per Labor Advisory 09 s.2020jadepatrick misaNo ratings yet
- Pid Application FormDocument2 pagesPid Application FormMark PesiganNo ratings yet
- Pamantasan NG Lungsod NG Valenzuela: College of AccountancyDocument1 pagePamantasan NG Lungsod NG Valenzuela: College of Accountancykyrie IrvingNo ratings yet
- ER COVID19 Monitoring Form - As Per Labor Advisory 09 s.2020Document2 pagesER COVID19 Monitoring Form - As Per Labor Advisory 09 s.2020jadepatrick misaNo ratings yet
- Tariff and Custom CodeDocument12 pagesTariff and Custom CodeAmy Olaes Dulnuan100% (1)
- PNVC's History of Bread RollsDocument19 pagesPNVC's History of Bread Rollskyrie IrvingNo ratings yet
- Local Taxes, Preferential Taxation, DTADocument7 pagesLocal Taxes, Preferential Taxation, DTAkyrie IrvingNo ratings yet
- Tax Remedies of The GovernmentDocument16 pagesTax Remedies of The GovernmentrmsenyoritaNo ratings yet
- Taxation: 8. Special Economic Zone ActDocument6 pagesTaxation: 8. Special Economic Zone ActJustin Robert RoqueNo ratings yet
- MAS Lecture Variable CostingDocument8 pagesMAS Lecture Variable CostingLhoel Delremedios100% (1)
- Taxation: Far Eastern University - ManilaDocument4 pagesTaxation: Far Eastern University - ManilacamilleNo ratings yet
- Double Taxation AgreementDocument9 pagesDouble Taxation AgreementAmy Olaes Dulnuan100% (1)
- Application For Registration: Combong Julius Paolo Noot PaoloDocument1 pageApplication For Registration: Combong Julius Paolo Noot PaoloJulius Noot CombongNo ratings yet
- TeamHandballstudyguide 2Document7 pagesTeamHandballstudyguide 2kyrie IrvingNo ratings yet
- Dokumen - Tips Branch Accounting TestbankDocument5 pagesDokumen - Tips Branch Accounting TestbankJessa Mae DuhaylongsodNo ratings yet
- Auditing Theory CabreraDocument26 pagesAuditing Theory CabrerarexNo ratings yet
- Taxation and Investment Code SummaryDocument10 pagesTaxation and Investment Code SummaryJustin Robert RoqueNo ratings yet
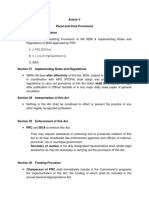
- Article VDocument4 pagesArticle Vkyrie IrvingNo ratings yet
- Ias34 en PDFDocument9 pagesIas34 en PDFAgnieszka KsnNo ratings yet
- BEng (Hons) Software Engineering - 12 Months (Top-Up Degree) - Delivered Online by LSBR, UKDocument19 pagesBEng (Hons) Software Engineering - 12 Months (Top-Up Degree) - Delivered Online by LSBR, UKLSBRNo ratings yet
- AeU Student Handbook PDFDocument96 pagesAeU Student Handbook PDFFatin ZainNo ratings yet
- Ananthapuramu Ap Gov inDocument9 pagesAnanthapuramu Ap Gov inEsther RaniNo ratings yet
- MBA - NSUT - 26.9.2020 FinalDocument27 pagesMBA - NSUT - 26.9.2020 FinalshubNo ratings yet
- Mia Faculty ProfileDocument2 pagesMia Faculty ProfileYuri BoykaNo ratings yet
- IIT BOMBAY PhDDocument86 pagesIIT BOMBAY PhDShubham Raj SinghNo ratings yet
- Regulate Guidance Counseling ProfessionDocument8 pagesRegulate Guidance Counseling ProfessionLorey May ArbasNo ratings yet
- Challenges in Oral Presentations for PUP StudentsDocument13 pagesChallenges in Oral Presentations for PUP StudentsNikki OlivaNo ratings yet
- Applicant Faqs: Joint Japan / World Bank Graduate Scholarship Program (JJ/WBGSP)Document8 pagesApplicant Faqs: Joint Japan / World Bank Graduate Scholarship Program (JJ/WBGSP)Fatma TotaNo ratings yet
- Sai Chandra Surakka CQU SOP Master of Project ManagementDocument8 pagesSai Chandra Surakka CQU SOP Master of Project ManagementAdithyaSirikondaNo ratings yet
- Human Resource Development HandbookDocument53 pagesHuman Resource Development HandbookLegend Anbu75% (4)
- Health Information Management Profession: Real-World Case 1.1Document8 pagesHealth Information Management Profession: Real-World Case 1.1Yusra MehmoodNo ratings yet
- Syllabus For Architecture and Planning (AR)Document5 pagesSyllabus For Architecture and Planning (AR)anusha8204No ratings yet
- Student Guide Book EnglishDocument104 pagesStudent Guide Book EnglishIT Hub SLNo ratings yet
- Ra 9966Document9 pagesRa 9966Nina L. Dela CruzNo ratings yet
- Ukm Coursework MasterDocument5 pagesUkm Coursework Masterbcrbcw6a100% (1)
- Egkjk"V! 'Kklu JKT Lkekbzd Izos'K Ijh (KK D (K) Egkjk"V! JKT ) EqacbzDocument36 pagesEgkjk"V! 'Kklu JKT Lkekbzd Izos'K Ijh (KK D (K) Egkjk"V! JKT ) EqacbzankurNo ratings yet
- Special Articles Pharmacy Education in Vietnam: A, B B, C A D D B, C B, CDocument12 pagesSpecial Articles Pharmacy Education in Vietnam: A, B B, C A D D B, C B, Cronahaniifah11No ratings yet
- Designing A Personal Lifelong Learning Plan: Its Definition and StepsDocument27 pagesDesigning A Personal Lifelong Learning Plan: Its Definition and Stepsintermaze100% (1)
- Republic of The Philippines Congress of The Philippines Metro Manila Sixteenth Congress Third Regular SessionDocument5 pagesRepublic of The Philippines Congress of The Philippines Metro Manila Sixteenth Congress Third Regular SessionBea SerranoNo ratings yet
- Official Website of the Department of Homeland Security STEM OPT ExtensionDocument1 pageOfficial Website of the Department of Homeland Security STEM OPT ExtensionTanishq SankaNo ratings yet
- Mepco Schlenk Engineering College (Autonomous), Sivakasi Affiliated To Anna University, Chennai Institute Vision Institute MissionDocument20 pagesMepco Schlenk Engineering College (Autonomous), Sivakasi Affiliated To Anna University, Chennai Institute Vision Institute MissionsuganyaNo ratings yet
- Introduction To SLO AssessmentDocument20 pagesIntroduction To SLO AssessmentLo RaNo ratings yet
- Denmark Medical Residency Database - MRDDocument18 pagesDenmark Medical Residency Database - MRDIbn SinaNo ratings yet
- 14 - CHED Memorandum Order No.46, s.2012Document41 pages14 - CHED Memorandum Order No.46, s.2012Brittaney BatoNo ratings yet
- ProspectusDocument21 pagesProspectusSarmishtha DeNo ratings yet
- Life After High School - A Post Secondary Students Guide To Success by Shawna NarayanDocument92 pagesLife After High School - A Post Secondary Students Guide To Success by Shawna Narayanapi-344973256No ratings yet
- Waqar AssignmentDocument50 pagesWaqar AssignmentMohammad WaqarNo ratings yet
- A Term Paper On Environmentalgeotechnics in NigeriaDocument9 pagesA Term Paper On Environmentalgeotechnics in NigeriaENGR. Damilare S.O (MNSE)(R.ENGR)No ratings yet
- Factors Affecting Students' Plans to Take the CPA ExamDocument9 pagesFactors Affecting Students' Plans to Take the CPA ExamMisshtaCNo ratings yet