You might also like
- ACORN TrialDocument11 pagesACORN TrialsaramabulolaNo ratings yet
- Hypertensive Emergencies in The Emergency DepartmentDocument13 pagesHypertensive Emergencies in The Emergency DepartmentLuis Lopez RevelesNo ratings yet
- Krisis HipertensiDocument12 pagesKrisis HipertensiDani NurseNo ratings yet
- Drug Treatment For Hypertensive Emergencies: New Concepts and Emerging Technologies For Emergency PhysiciansDocument0 pagesDrug Treatment For Hypertensive Emergencies: New Concepts and Emerging Technologies For Emergency PhysiciansRajihah JihahNo ratings yet
- Secondary Arterial Hypertension: When, Who, and How To Screen?Document12 pagesSecondary Arterial Hypertension: When, Who, and How To Screen?MelissaHuayapaANo ratings yet
- Assessment of bleeding Shock in a Politraumatized PatientFrom EverandAssessment of bleeding Shock in a Politraumatized PatientNo ratings yet
- Apasi Yg Ga Buat NisaDocument20 pagesApasi Yg Ga Buat Nisamuhammad iqbal mahfuzhNo ratings yet
- W1L1 - Initial Assessment For Trauma - 2Document44 pagesW1L1 - Initial Assessment For Trauma - 2Baihaqi SaharunNo ratings yet
- Primary Trauma CareDocument48 pagesPrimary Trauma CareKABERA RENENo ratings yet
- Hypertension, Hypertensive Crisis, and Hypertensive Emergency: Approaches To Emergency Department CareDocument11 pagesHypertension, Hypertensive Crisis, and Hypertensive Emergency: Approaches To Emergency Department CarePebrian SyahNo ratings yet
- 4th Problem Emergency Medicine Group 1Document82 pages4th Problem Emergency Medicine Group 1Jonathan TandajuNo ratings yet
- 7 Steps Patient SafetyDocument58 pages7 Steps Patient SafetyDanissa Fidia PuteriNo ratings yet
- 10.08.07 Cardiac Tamponade HaagDocument16 pages10.08.07 Cardiac Tamponade HaagfoetorNo ratings yet
- Hypertensive CrisisDocument1 pageHypertensive Crisisapi-495201002No ratings yet
- Management of Multiple Traumatised PatientDocument4 pagesManagement of Multiple Traumatised PatientOmar MohammedNo ratings yet
- Blood Pressure Management in Patients With Diabetes: Clinical Trial Evidence For BP ControlDocument8 pagesBlood Pressure Management in Patients With Diabetes: Clinical Trial Evidence For BP ControlNovita WulandariNo ratings yet
- Early Warning Score & Rapid Response TeamDocument26 pagesEarly Warning Score & Rapid Response TeamAsim IdreesNo ratings yet
- Care of The Patient in The Perioperative PeriodDocument20 pagesCare of The Patient in The Perioperative PeriodMohammed FaragNo ratings yet
- Reducing Medical Error and Increasing Patient Safety: Richard Smith Editor, BMJDocument29 pagesReducing Medical Error and Increasing Patient Safety: Richard Smith Editor, BMJNOORAIMAH MURAHNo ratings yet
- Managemant Copd CPG MsiaDocument67 pagesManagemant Copd CPG MsiaNur Anis ZarimeNo ratings yet
- Obgyn Guidelines HypertensionDocument20 pagesObgyn Guidelines HypertensionGladys AilingNo ratings yet
- ABCs of Thoracic TraumaDocument5 pagesABCs of Thoracic TraumaAlice S ChangNo ratings yet
- Hospital Discharge Education For CHFDocument18 pagesHospital Discharge Education For CHFarafathusein29No ratings yet
- Cardiac TamponadeDocument29 pagesCardiac Tamponadeanimesh pandaNo ratings yet
- CDR Ankle Card PDFDocument2 pagesCDR Ankle Card PDFSalsa_Picante_BabyNo ratings yet
- The New Rapid ResponderDocument3 pagesThe New Rapid RespondersarahNo ratings yet
- Australian Triage Process ReviewDocument203 pagesAustralian Triage Process ReviewDeni WahyudiNo ratings yet
- Initial Assessment AND ManagementDocument30 pagesInitial Assessment AND ManagementSikaNo ratings yet
- Postpartum Hemorrhage With A Standardized Massive Transfusion ProtocolDocument9 pagesPostpartum Hemorrhage With A Standardized Massive Transfusion Protocolmedicinaun74100% (2)
- Overview of Fetal AssessmentDocument3 pagesOverview of Fetal AssessmentAde Yonata100% (1)
- Burman Thyroid Disorders and Diseases PDFDocument242 pagesBurman Thyroid Disorders and Diseases PDFxguerratNo ratings yet
- Evaluation of Headache in AdultsDocument21 pagesEvaluation of Headache in AdultsMaicon RamosNo ratings yet
- Revisions To The Canadian Emergency Department Triage and Acuity Scale Implementation GuidelinesDocument8 pagesRevisions To The Canadian Emergency Department Triage and Acuity Scale Implementation GuidelinesTiti Multi SaariNo ratings yet
- Trauma and Emergency NursingDocument9 pagesTrauma and Emergency Nursingchinthaka18389021No ratings yet
- Approach To A Dermatologic PatientDocument3 pagesApproach To A Dermatologic PatientJessica Febrina WuisanNo ratings yet
- Initial Assessment and ManagementDocument8 pagesInitial Assessment and ManagementAlvin De LunaNo ratings yet
- How To Treat: Septic ShockDocument6 pagesHow To Treat: Septic ShockmeeandsoeNo ratings yet
- Liver Trauma: DR Tarik El Batrawy Specialist General SurgeryDocument50 pagesLiver Trauma: DR Tarik El Batrawy Specialist General Surgerykata61No ratings yet
- VTE Prophylaxis GuidelinesDocument1 pageVTE Prophylaxis GuidelinesSylvia Ruth Alisa Nababan100% (1)
- Data Collection Form - Pressure InjuryDocument3 pagesData Collection Form - Pressure InjuryErwin Dela GanaNo ratings yet
- Critical CareDocument9 pagesCritical CareGalaleldin AliNo ratings yet
- Pre Hos TraumaDocument11 pagesPre Hos TraumaGel OmugtongNo ratings yet
- Results Driven For Medical Writing and PharmacovigilanceDocument3 pagesResults Driven For Medical Writing and PharmacovigilancelisiwangNo ratings yet
- Torso TraumaDocument58 pagesTorso TraumaAbidisHereNo ratings yet
- Stroke Clinical PathwayDocument1 pageStroke Clinical PathwayKanoknun PisitpatcaragulNo ratings yet
- Nursing in EmergenciesDocument5 pagesNursing in EmergenciesAvisheel KalsiNo ratings yet
- Kuwait Institute For Medical Specialization: Membership of Specialty in Emergency MedicineDocument57 pagesKuwait Institute For Medical Specialization: Membership of Specialty in Emergency MedicinepynproNo ratings yet
- Using The ACLS Primary Survey For A Patient in Respiratory ArrestDocument34 pagesUsing The ACLS Primary Survey For A Patient in Respiratory Arrest강기연100% (1)
- EDJobDescriptionDocument18 pagesEDJobDescriptionAnonymous YqCxXQ6wF5No ratings yet
- INITIAL PRENATAL ASSESSMENT ProcedureDocument17 pagesINITIAL PRENATAL ASSESSMENT ProcedureCyndryl SampotonNo ratings yet
- Assessment - Critical CareDocument1 pageAssessment - Critical CareMartini ListrikNo ratings yet
- Policy For Community First Responders V3.0Document14 pagesPolicy For Community First Responders V3.0f4phixerukNo ratings yet
- Hanson Infectious Diseases - Anamneza I StatusDocument33 pagesHanson Infectious Diseases - Anamneza I StatusSilvia KesegNo ratings yet
- Paediatric Notes - Moodle/Text: Paediatric Emergencies (Textbook Ch.5)Document6 pagesPaediatric Notes - Moodle/Text: Paediatric Emergencies (Textbook Ch.5)Jana AldourNo ratings yet
- 5 12 Components of Wound Assessment and Documentation-2Document3 pages5 12 Components of Wound Assessment and Documentation-2Jing CruzNo ratings yet
- Certified Family Nurse Practitioner in West Palm Beach FL Resume Pamela ValleDocument3 pagesCertified Family Nurse Practitioner in West Palm Beach FL Resume Pamela VallePamelaValleNo ratings yet
- Trauma Assessment: Aims of The Initial Evaluation of Trauma PatientsDocument6 pagesTrauma Assessment: Aims of The Initial Evaluation of Trauma Patientsece142No ratings yet
- Isolation Guidelines PDFDocument209 pagesIsolation Guidelines PDFlimiya varghese100% (1)
- ThrombophlebitisDocument3 pagesThrombophlebitismirrejNo ratings yet
- The Mood Disorder QuestionnaireDocument2 pagesThe Mood Disorder QuestionnaireRonaldo CordeiroNo ratings yet
- Drug Study Case PresentationDocument5 pagesDrug Study Case PresentationRobert MedinaNo ratings yet
- The Affect of Social Media On Mental HealthDocument12 pagesThe Affect of Social Media On Mental Healthapi-466264512No ratings yet
- Alcoholism: Alcoholism Is The Most Serious Form of ProblemDocument12 pagesAlcoholism: Alcoholism Is The Most Serious Form of ProblemfrajvalNo ratings yet
- Business ProposalDocument5 pagesBusiness Proposalapi-299665237No ratings yet
- The Road Not TakenDocument6 pagesThe Road Not Takencaren santosNo ratings yet
- Histrionic Personality DisorderDocument3 pagesHistrionic Personality DisorderDr. Celeste Fabrie100% (3)
- Exampleof ThesisDocument23 pagesExampleof ThesisMeyrielle C. DuclayanNo ratings yet
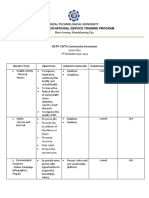
- Rizal Technological University Center For National Service Training ProgramDocument2 pagesRizal Technological University Center For National Service Training ProgramAbegail CatindigNo ratings yet
- Dapus ImsDocument3 pagesDapus ImsKhalila IzdiharNo ratings yet
- Gateway B1 - Workbook Answer Key Gatewayonline - Marwel1Document1 pageGateway B1 - Workbook Answer Key Gatewayonline - Marwel1Đức Anh vũNo ratings yet
- Herniation Flash CardDocument4 pagesHerniation Flash CardAin GhazaliNo ratings yet
- Sample Nursing Assessment Form: Section 4Document24 pagesSample Nursing Assessment Form: Section 4silviaNo ratings yet
- Test Bank For Goulds Pathophysiology For The Health Professions 5 Edition Karin C VanmeterDocument10 pagesTest Bank For Goulds Pathophysiology For The Health Professions 5 Edition Karin C VanmeterKip Field100% (31)
- 2503 6018 1 PBDocument10 pages2503 6018 1 PBFedericó SchëlzerNo ratings yet
- Nur 151 Coa P2Document9 pagesNur 151 Coa P2Zymer Lee Abasolo100% (1)
- BCCA AB in Febrile Neutropenia GuidelinesDocument2 pagesBCCA AB in Febrile Neutropenia GuidelinesAlvy SyukrieNo ratings yet
- Food For Your Ears - Boost Your Hearing Health - EarGuru - inDocument23 pagesFood For Your Ears - Boost Your Hearing Health - EarGuru - inAmrik SinghNo ratings yet
- NYCTALOPIADocument16 pagesNYCTALOPIAAroob YaseenNo ratings yet
- Pre-NEET Obstetrics and Gynaecology (Sakshi Arora)Document321 pagesPre-NEET Obstetrics and Gynaecology (Sakshi Arora)Vinay Reddy100% (10)
- AIC CHAS Brochure English - DN4 - NCDocument2 pagesAIC CHAS Brochure English - DN4 - NCvelangniNo ratings yet
- The Basics About Panic AttacksDocument30 pagesThe Basics About Panic AttacksKonstantinos SmixiotisNo ratings yet
- 8899 804580458674 1 SMDocument12 pages8899 804580458674 1 SMIkra 77721No ratings yet
- PamphletDocument1 pagePamphletAldenn MinotaurNo ratings yet
- Vergara v. HammoniaDocument5 pagesVergara v. HammoniaAngelette BulacanNo ratings yet
- Written Report "Osteoarthritis": Catanduanes State University College of Health Sciences Department of NursingDocument4 pagesWritten Report "Osteoarthritis": Catanduanes State University College of Health Sciences Department of NursingMezil NazarenoNo ratings yet
- Newborn CarePlanDocument8 pagesNewborn CarePlanXtin Buendia Cordero0% (1)
- Bacteriological Analysis of Selected Borehole Water With in Ilishan - Remo Community Ogun State NigeriaDocument13 pagesBacteriological Analysis of Selected Borehole Water With in Ilishan - Remo Community Ogun State NigeriaInternational Journal of Innovative Science and Research Technology100% (1)
- Neurological AssessmentDocument13 pagesNeurological AssessmentLorenz Jude CańeteNo ratings yet
- Clinical Characteristics, Laboratory Abnormalities and Outcome of Covid-19 Positive Patients Admitted in Tertiary Care Hospital of KarachiDocument8 pagesClinical Characteristics, Laboratory Abnormalities and Outcome of Covid-19 Positive Patients Admitted in Tertiary Care Hospital of KarachiIJAR JOURNALNo ratings yet