You might also like
- Clin Physio Funct Imaging - 2013 - Munkholm - Mucociliary Clearance Pathophysiological AspectsDocument7 pagesClin Physio Funct Imaging - 2013 - Munkholm - Mucociliary Clearance Pathophysiological AspectsIkon ikonicNo ratings yet
- Early Hemodynamic Management of Critically Ill Burn PatientsDocument7 pagesEarly Hemodynamic Management of Critically Ill Burn PatientsItzel TextaNo ratings yet
- Ox InflammationDocument15 pagesOx Inflammationcc vereNo ratings yet
- Lymphatic SystemDocument28 pagesLymphatic SystemRozi Reviana PratiwiNo ratings yet
- Dimitrova Et Al-2012-Principles of Osteoarthritis - Its Definition, Character, Derivation And...Document28 pagesDimitrova Et Al-2012-Principles of Osteoarthritis - Its Definition, Character, Derivation And...STAF OSCENo ratings yet
- NbikjnlkDocument10 pagesNbikjnlkKELAS 10ANo ratings yet
- Fluid Management in Perioperative and Critically Ill Patients - Acute and Critical Care PDFDocument11 pagesFluid Management in Perioperative and Critically Ill Patients - Acute and Critical Care PDFMaria Siachoque JaraNo ratings yet
- Cannabinoids and Inflammations of The Gut-Lung-Skin BarrierDocument26 pagesCannabinoids and Inflammations of The Gut-Lung-Skin BarrierYusuf ElmaNo ratings yet
- From Inflammation To Sickness Historical PerspectiveDocument5 pagesFrom Inflammation To Sickness Historical PerspectiveВладимир ДружининNo ratings yet
- Fphys 15 1374627Document17 pagesFphys 15 1374627jakkj205No ratings yet
- Biomimetic Channel Modeling Local Vascular Dynamics of Pro-Inflammatory Endothelial ChangesDocument19 pagesBiomimetic Channel Modeling Local Vascular Dynamics of Pro-Inflammatory Endothelial Changesrehena mojammelNo ratings yet
- Hypovolemia With Peripheral Edema: What Is Wrong?Document10 pagesHypovolemia With Peripheral Edema: What Is Wrong?BernaHerediaNo ratings yet
- Wiig 2012Document56 pagesWiig 2012SDNKSJNDJKNo ratings yet
- The Lymphatic Fluid: Laura SantambrogioDocument23 pagesThe Lymphatic Fluid: Laura SantambrogioktorooNo ratings yet
- Best-Jabaley2019 Article FluidManagementInSepticShockARDocument7 pagesBest-Jabaley2019 Article FluidManagementInSepticShockARKrish RendonNo ratings yet
- Fluids in ARDS: More Pros Than Cons: Review Open AccessDocument11 pagesFluids in ARDS: More Pros Than Cons: Review Open AccessPaulHerreraNo ratings yet
- Intraoperative Fluids: How Much Is Too Much?: Editor's Key PointsDocument11 pagesIntraoperative Fluids: How Much Is Too Much?: Editor's Key PointsRicardoNo ratings yet
- Biochimica Et Biophysica Acta: Paul F. Mercer, Rachel C. ChambersDocument10 pagesBiochimica Et Biophysica Acta: Paul F. Mercer, Rachel C. ChambersMonnierNo ratings yet
- Temporomandibular Joint Pain and Synovial Fluid Analysis: A Review of The LiteratureDocument8 pagesTemporomandibular Joint Pain and Synovial Fluid Analysis: A Review of The Literaturedavidcosmin186832No ratings yet
- Angiogenesis 1Document18 pagesAngiogenesis 1Tausif AlamNo ratings yet
- The Cough Re Ex: The Janus of Respiratory Medicine: Frontiers in Physiology June 2021Document9 pagesThe Cough Re Ex: The Janus of Respiratory Medicine: Frontiers in Physiology June 2021stellacharlesNo ratings yet
- Hypertonic Stress in The Kidney: A Necessary Evil: Min Seong Kwon, Sun Woo Lim and H. Moo KwonDocument7 pagesHypertonic Stress in The Kidney: A Necessary Evil: Min Seong Kwon, Sun Woo Lim and H. Moo Kwoncrina1980No ratings yet
- Bickler 2016Document11 pagesBickler 2016Manoela Leticia Oliveira CarolinoNo ratings yet
- Hyperbaric Oxygen Therapy. Part 2Document9 pagesHyperbaric Oxygen Therapy. Part 2Yun AkbarNo ratings yet
- WCM2018 ABSTRACTS Microcirculation JournalDocument97 pagesWCM2018 ABSTRACTS Microcirculation JournalalbertwolandNo ratings yet
- Laryngeal Inflammation: Annals of Otolaryngology and RhinologyDocument8 pagesLaryngeal Inflammation: Annals of Otolaryngology and RhinologyMarlina ElvianaNo ratings yet
- Flare Ups in Endodontics - 1 Etiological FactorsDocument6 pagesFlare Ups in Endodontics - 1 Etiological FactorsdrshravyaNo ratings yet
- Addisu TGF BetadermatologyDocument7 pagesAddisu TGF Betadermatologyطارق المتوليNo ratings yet
- Bonanno 2001Document8 pagesBonanno 2001soranydNo ratings yet
- The Role of Cytokines in Pulp Inflammation PDFDocument18 pagesThe Role of Cytokines in Pulp Inflammation PDFDiana Fitri MuslimahNo ratings yet
- Badaut Zhang Preface2019 ADocument5 pagesBadaut Zhang Preface2019 AGonzalo AltamiranoNo ratings yet
- The Pathophysiology of Peritonitis: Review ArticleDocument20 pagesThe Pathophysiology of Peritonitis: Review ArticlepogichannyNo ratings yet
- Biomedicines 12 00664Document16 pagesBiomedicines 12 00664jamel-shamsNo ratings yet
- 2013 Journal of Surgical ResearchDocument8 pages2013 Journal of Surgical ResearchFernando ZanoniNo ratings yet
- Eosinophils in Vasculitis Characteristics - Khoury-Nrrheum.2014.98Document11 pagesEosinophils in Vasculitis Characteristics - Khoury-Nrrheum.2014.98Francisco Baca DejoNo ratings yet
- Perioperative Uid Therapy For Anaesthetists and IntensivistsDocument4 pagesPerioperative Uid Therapy For Anaesthetists and IntensivistsDanitza Pari TiconaNo ratings yet
- Effects of Honokiol On Sepsis-Induced Acute Kidney Injury in An Experimental Model of Sepsis in RatsDocument9 pagesEffects of Honokiol On Sepsis-Induced Acute Kidney Injury in An Experimental Model of Sepsis in RatsMuhammad Bayu Zohari HutagalungNo ratings yet
- AR Flare UpDocument7 pagesAR Flare UpCARLA PATRICIA JORDAN SALAZARNo ratings yet
- Resuscitation Fluid Choices To Preserve The Endothelial GlycocalyxDocument11 pagesResuscitation Fluid Choices To Preserve The Endothelial GlycocalyxDanang Bagus UntoroNo ratings yet
- Acute Fluid Management of Large Burns Pathophysiology, Monitoring, and ResuscitationDocument9 pagesAcute Fluid Management of Large Burns Pathophysiology, Monitoring, and ResuscitationEduardo Espin LanzNo ratings yet
- Judul ReferatDocument13 pagesJudul ReferatsyongebobNo ratings yet
- Contemporary Reviews in Cardiovascular Medicine: Endothelial Function and DysfunctionDocument11 pagesContemporary Reviews in Cardiovascular Medicine: Endothelial Function and DysfunctionBelia Bima NafisaNo ratings yet
- Hypoxia and InflammationDocument10 pagesHypoxia and InflammationAbel Espinoza MedallaNo ratings yet
- 14 PDFDocument12 pages14 PDFeliasNo ratings yet
- High Acuity Fluid and Electrolytes Chapter 25Document19 pagesHigh Acuity Fluid and Electrolytes Chapter 25AANo ratings yet
- Rose 1Document7 pagesRose 1isa mahendraNo ratings yet
- Lymphatic Fluid: Exchange Mechanisms and Regulation: Virginia H. Huxley and Joshua ScallanDocument9 pagesLymphatic Fluid: Exchange Mechanisms and Regulation: Virginia H. Huxley and Joshua ScallanFaisal RuhiatnaNo ratings yet
- Species Variation in Biology and Physiology of The Ciliary Epithelium Similarities and DifferencesDocument10 pagesSpecies Variation in Biology and Physiology of The Ciliary Epithelium Similarities and DifferencesShashi kant ChaudharyNo ratings yet
- Nasal Polyposis: Current TrendsDocument6 pagesNasal Polyposis: Current TrendsClodeyaRizolaNo ratings yet
- Endothelial Barrier Dysfunction in Septic Shock: ReviewDocument17 pagesEndothelial Barrier Dysfunction in Septic Shock: ReviewSola SacraNo ratings yet
- Biological Markers For Pulpal Inflammation: A Systematic ReviewDocument24 pagesBiological Markers For Pulpal Inflammation: A Systematic ReviewMohab HegazyNo ratings yet
- Occurrence of Tendon Pathologies in MetabolicDocument10 pagesOccurrence of Tendon Pathologies in MetabolicSebastián Jiménez GaticaNo ratings yet
- Interaction of Endothelial Cells With Macrophages - Linking Molecular and Metabolic SignalingDocument11 pagesInteraction of Endothelial Cells With Macrophages - Linking Molecular and Metabolic SignalingSergeat18BNo ratings yet
- Oxygen in Wound Healing Nutrient, Antibiotic, Signaling Molecule, and Therapeutic Agent PDFDocument22 pagesOxygen in Wound Healing Nutrient, Antibiotic, Signaling Molecule, and Therapeutic Agent PDFIsabela MagriniNo ratings yet
- Implications Pathogenesis: GingivalDocument30 pagesImplications Pathogenesis: GingivalI Gede MahardikaNo ratings yet
- Leg Edema Assessment and Management - ArticleDocument11 pagesLeg Edema Assessment and Management - ArticleRafan AddisNo ratings yet
- Oral Physiology: Proceedings of the International Symposium Held in Wenner-Gren Center, Stockholm, August 1971From EverandOral Physiology: Proceedings of the International Symposium Held in Wenner-Gren Center, Stockholm, August 1971Nils EmmelinNo ratings yet
- Profound Gene Expression Changes in The Epithelial Monolayer of Active Ulcerative Colitis and Crohn's DiseaseDocument23 pagesProfound Gene Expression Changes in The Epithelial Monolayer of Active Ulcerative Colitis and Crohn's DiseaseYaumil ChoiriNo ratings yet
- The Physiological Regulation of Thirst and Fluid Intake: ArticlesDocument6 pagesThe Physiological Regulation of Thirst and Fluid Intake: ArticlesCony GSNo ratings yet
- Enfermedades Pleurales NEJM 2018Document12 pagesEnfermedades Pleurales NEJM 2018rene.javier.96No ratings yet
- Tourville - Guenther 2013 Actualizacion DIVA Model PDFDocument27 pagesTourville - Guenther 2013 Actualizacion DIVA Model PDFDaniel Gaete OsorioNo ratings yet
- 3 Placenta Previa Nursing Care PlansDocument7 pages3 Placenta Previa Nursing Care PlansAjay RajpootNo ratings yet
- Toxoplasmosis of Animals and Humans, 3rd EditionDocument566 pagesToxoplasmosis of Animals and Humans, 3rd EditionAlexNo ratings yet
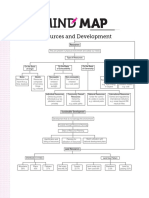
- MindmapDocument1 pageMindmapSwapnil Tak25% (4)
- The Physic Body MechanicsDocument8 pagesThe Physic Body MechanicsNur RasyiqahNo ratings yet
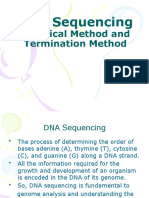
- DNA Sequencing-Powerpoint Presentation-Professor'sDocument24 pagesDNA Sequencing-Powerpoint Presentation-Professor'sNabaratna BiswalNo ratings yet
- Practice Final ExamDocument29 pagesPractice Final ExamMonessa Kaye GomezNo ratings yet
- Alma Ata Conference 1978 ReportDocument77 pagesAlma Ata Conference 1978 ReportRegine Lorenzana Mey-AngNo ratings yet
- Edwards - Categories Are For Talking T&P 1991Document26 pagesEdwards - Categories Are For Talking T&P 1991txthedxNo ratings yet
- 2023 - Hoa Ninh Et Al - Vietnamophryne AurantifuscaDocument14 pages2023 - Hoa Ninh Et Al - Vietnamophryne AurantifuscaHạt Vừng LépNo ratings yet
- BMB Technical Bulletin No 2016-10 Outline of Cave Wetland Management PlanDocument4 pagesBMB Technical Bulletin No 2016-10 Outline of Cave Wetland Management PlanAnonymous dtceNuyIFI100% (1)
- Economics 11Document2 pagesEconomics 11KevinB CaigasNo ratings yet
- Exercise-1: History, Variation, MendelismDocument41 pagesExercise-1: History, Variation, MendelismAhxhsNo ratings yet
- Child Development GROUP SOPHIEDocument30 pagesChild Development GROUP SOPHIESyazwani ZainalNo ratings yet
- FRCEM ExamPrep GITDocument30 pagesFRCEM ExamPrep GITsk100% (1)
- College of Medical Laboratory Science Our Lady of Fatima University-VelenzuelaDocument33 pagesCollege of Medical Laboratory Science Our Lady of Fatima University-VelenzuelaClaire GonoNo ratings yet
- Production Options For Psilocybin Making of The MagicDocument7 pagesProduction Options For Psilocybin Making of The MagicYingjie ZhouNo ratings yet
- Detailed Lesson Plan in Science 7 Biodiversity The Learners Will Be Able ToDocument7 pagesDetailed Lesson Plan in Science 7 Biodiversity The Learners Will Be Able ToCristan Turdil BugtongNo ratings yet
- Photosynthesis - WikipediaDocument22 pagesPhotosynthesis - Wikipediaمحمد جانNo ratings yet
- A Compilation of Philippine Environmental LawsDocument39 pagesA Compilation of Philippine Environmental LawsRussel Sirot100% (3)
- ALS Reversals Demographics Disease Characteristics Treatments and Co MorbiditiesDocument6 pagesALS Reversals Demographics Disease Characteristics Treatments and Co MorbiditiesJoseaneNo ratings yet
- Chapter 13 - Genetic EngineeringDocument23 pagesChapter 13 - Genetic EngineeringDanielle TurnerNo ratings yet
- Phylogeny and EvolutionDocument12 pagesPhylogeny and EvolutionKathryn Palmerton0% (1)
- Science Form 3 Chapter 3: Name: Class: DateDocument6 pagesScience Form 3 Chapter 3: Name: Class: DateTeng Pei ErNo ratings yet
- Atlas of Oculoplastic and Orbital SurgeryDocument336 pagesAtlas of Oculoplastic and Orbital Surgerymelati100% (3)
- Physiology Su00Document42 pagesPhysiology Su00Mahad Ahmed HilowleNo ratings yet
- Essay GENETICALLY MODIFIED FOODDocument7 pagesEssay GENETICALLY MODIFIED FOODSandro BomfimNo ratings yet
- Precipath HDL - LDL-C.11818171001.V10.en PDFDocument2 pagesPrecipath HDL - LDL-C.11818171001.V10.en PDFARIF AHAMMED PNo ratings yet
- An Open Letter To My Daughter: Rebecca L. FisherDocument2 pagesAn Open Letter To My Daughter: Rebecca L. Fisherrfisher284_164995324No ratings yet
- Septal Extension Graft ArticlesDocument7 pagesSeptal Extension Graft Articlesjose orlando sturla pelleranoNo ratings yet