You might also like
- Aspectos Clinicos NmoDocument11 pagesAspectos Clinicos NmoOlga Manco GuzmánNo ratings yet
- 1 s2.0 S152550500500185X MainDocument10 pages1 s2.0 S152550500500185X MainmarleneNo ratings yet
- The Clinical Syndrome Cerebral MalariaDocument14 pagesThe Clinical Syndrome Cerebral Malaria1130120017 ALI ANTONO TANNo ratings yet
- Camargo 2018 (Pathology, Pathophysio, Diagnosis, Symptomps, Treatment)Document6 pagesCamargo 2018 (Pathology, Pathophysio, Diagnosis, Symptomps, Treatment)Rizki Muhammad RanandaNo ratings yet
- Neuropathology Autopsy Practice Post Mortem Examination in Cerebrovascular Disease StrokeDocument15 pagesNeuropathology Autopsy Practice Post Mortem Examination in Cerebrovascular Disease Strokelisboa_rodriNo ratings yet
- Posterior Circulation Stroke: Advances in Understanding and ManagementFrom EverandPosterior Circulation Stroke: Advances in Understanding and ManagementJong S. KimNo ratings yet
- Cerebellar MutismDocument4 pagesCerebellar MutismDwi Puja SetiawanNo ratings yet
- Status Epilepticus in Critically Ill PatientsDocument11 pagesStatus Epilepticus in Critically Ill PatientsAkbal Nur KarimNo ratings yet
- Handbook of Medical Neuropsychology: Applications of Cognitive NeuroscienceFrom EverandHandbook of Medical Neuropsychology: Applications of Cognitive NeuroscienceNo ratings yet
- An Algorithm For The Evaluation of Peripheral Neuropathy - American Family PhysicianDocument9 pagesAn Algorithm For The Evaluation of Peripheral Neuropathy - American Family PhysicianAnonymous vnv6QFNo ratings yet
- Sturge Weber SyndromeDocument14 pagesSturge Weber SyndromeAnumeha JindalNo ratings yet
- Empty Sella Syndrome: Continuing Education ActivityDocument8 pagesEmpty Sella Syndrome: Continuing Education Activityn2763288No ratings yet
- Malaria and StrokeDocument3 pagesMalaria and StrokeRia Septi HarmiaNo ratings yet
- Neuromyelitis Optica: Mark J. Morrow, MD, Dean Wingerchuk, MD, MSC, FRCP (C)Document13 pagesNeuromyelitis Optica: Mark J. Morrow, MD, Dean Wingerchuk, MD, MSC, FRCP (C)sidogra100% (1)
- Heart Valve Disease: State of the ArtFrom EverandHeart Valve Disease: State of the ArtJose ZamoranoNo ratings yet
- Aicardi Goutieres SyndromeDocument7 pagesAicardi Goutieres Syndromezloncar3No ratings yet
- 2022 Masingue P.Latour Rev Neurol Genetic Analysis in HereditaryDocument20 pages2022 Masingue P.Latour Rev Neurol Genetic Analysis in HereditaryLéo VidoniNo ratings yet
- Clinical and Genetic Basis of Familial Amyotrophic Lateral Sclerosis (Revisión)Document12 pagesClinical and Genetic Basis of Familial Amyotrophic Lateral Sclerosis (Revisión)Francisco Ahumada MéndezNo ratings yet
- Highlights in Neuro OphthalmologyDocument2 pagesHighlights in Neuro OphthalmologyShruthi VMNo ratings yet
- Semiology of Insular Lobe Seizures: SciencedirectDocument6 pagesSemiology of Insular Lobe Seizures: SciencedirectViviana Torres BallesterosNo ratings yet
- Semiology of Insular Lobe Seizures: SciencedirectDocument6 pagesSemiology of Insular Lobe Seizures: SciencedirectViviana Torres BallesterosNo ratings yet
- CNS Diseases and UveitisDocument25 pagesCNS Diseases and UveitisHabib G. Moutran BarrosoNo ratings yet
- E RefdDocument13 pagesE RefdGabriella TjondroNo ratings yet
- Pseudo 1Document20 pagesPseudo 1giant nitaNo ratings yet
- Investigatory Project inDocument31 pagesInvestigatory Project inrchandralega2205100% (1)
- Wernicke Korsakoff SyndromeDocument19 pagesWernicke Korsakoff Syndrometerry2wa100% (4)
- Motor Neuron DiseaseDocument7 pagesMotor Neuron DiseasegeraldineongNo ratings yet
- What Can Mimic Multiple Sclerosis?Document29 pagesWhat Can Mimic Multiple Sclerosis?Ankita ShahNo ratings yet
- The Expanded Spectrum of Neuromyelitis oDocument7 pagesThe Expanded Spectrum of Neuromyelitis oFlavia ChNo ratings yet
- Tolosa HuntDocument10 pagesTolosa HuntRoxana StanciuNo ratings yet
- Facomatosis Pubmed PDFDocument8 pagesFacomatosis Pubmed PDFKevin ChaucaNo ratings yet
- Neurological Assessment of ComaDocument5 pagesNeurological Assessment of Comapanda7100No ratings yet
- Central Ocular Motor Disorders, Including Gaze Palsy and NystagmusDocument17 pagesCentral Ocular Motor Disorders, Including Gaze Palsy and NystagmusAnonymous vnv6QFNo ratings yet
- Orofacial Reflex Myocloni. Definition, Relation To Epilepsy Syndromes, Nosological and Prognosis Significance. A Focused ReviewDocument5 pagesOrofacial Reflex Myocloni. Definition, Relation To Epilepsy Syndromes, Nosological and Prognosis Significance. A Focused ReviewJuliana AparcanaNo ratings yet
- JURNALDocument10 pagesJURNALLuses Shantia HaryantoNo ratings yet
- Multiple Sclerosis - The Disease and Its ManifestationsDocument8 pagesMultiple Sclerosis - The Disease and Its ManifestationsCecilia FRNo ratings yet
- Infantile Spasms: Review of The Literature and Personal ExperienceDocument10 pagesInfantile Spasms: Review of The Literature and Personal ExperienceDianMuliasariNo ratings yet
- 3rd Taccone MSDocument18 pages3rd Taccone MSDouglasNo ratings yet
- Focal Epilepsy Causes and Clinical Features - UpToDateDocument44 pagesFocal Epilepsy Causes and Clinical Features - UpToDateBenjamínGalvanNo ratings yet
- Espectro Neuromielitis Óptica 2022 NejmDocument9 pagesEspectro Neuromielitis Óptica 2022 NejmOscar BushNo ratings yet
- FS007v1 RasmussensDocument4 pagesFS007v1 Rasmussensbilly2107No ratings yet
- Finding (Neurology)Document12 pagesFinding (Neurology)Ayu NoviantiNo ratings yet
- Encefalite Herpética 4 Casos Rev Neurol 2002Document6 pagesEncefalite Herpética 4 Casos Rev Neurol 2002Ana SopaNo ratings yet
- 10.1007@s00381 020 04746 9Document12 pages10.1007@s00381 020 04746 9Alvaro Perez HenriquezNo ratings yet
- Status Epilepticus in ChildrenDocument73 pagesStatus Epilepticus in ChildrenvelasquezcamposmaximoNo ratings yet
- Seizure and EpilepsyDocument9 pagesSeizure and EpilepsyAien LeeNo ratings yet
- Pathogenesis of Opsoclonus MyoclonusDocument2 pagesPathogenesis of Opsoclonus MyoclonusIRENA GENINo ratings yet
- Facial Nerve Palsy: Dr. Saud AlromaihDocument74 pagesFacial Nerve Palsy: Dr. Saud AlromaihChandra ManapaNo ratings yet
- Nejmra 1904655Document9 pagesNejmra 1904655silviaNo ratings yet
- Acute Dizziness, Vertigo, and Unsteadiness 2021 NCDocument17 pagesAcute Dizziness, Vertigo, and Unsteadiness 2021 NCLaura A M MNo ratings yet
- Differential Diagnosis of Cardiogenic Syncope and Seizure DisordersDocument6 pagesDifferential Diagnosis of Cardiogenic Syncope and Seizure DisordersganangahimsaNo ratings yet
- Si Gede Teguh Surya Negara 011.06.0043: 28/08/2017 1 FK Unizar Mataram 2017Document50 pagesSi Gede Teguh Surya Negara 011.06.0043: 28/08/2017 1 FK Unizar Mataram 2017'aac' JujuuNo ratings yet
- Central Vertigo PDFDocument6 pagesCentral Vertigo PDFarlinieNo ratings yet
- Multiple SclerosisDocument4 pagesMultiple SclerosisMarwan M.No ratings yet
- Current Concept of Neuromyelitis Optica (NMO) and NMO Spectrum DisordersDocument10 pagesCurrent Concept of Neuromyelitis Optica (NMO) and NMO Spectrum DisordersGabriella TjondroNo ratings yet
- C R C S: Urrent Eview in Linical CienceDocument7 pagesC R C S: Urrent Eview in Linical CienceAdriel Chandra AngNo ratings yet
- Central Pontine Myelinolysis and The Osmotic Demyelination 2021Document10 pagesCentral Pontine Myelinolysis and The Osmotic Demyelination 2021Nicolas RodriguezNo ratings yet
- Non Breathing Related Sleep Disorders Following StrokeDocument6 pagesNon Breathing Related Sleep Disorders Following StrokeRizqan Fahlevvi AkbarNo ratings yet
- Posterior Reversible Encephalopathy SyndDocument7 pagesPosterior Reversible Encephalopathy SyndasasakopNo ratings yet
- Brachii - Google SearchDocument1 pageBrachii - Google SearchdzhzrnNo ratings yet
- Disc & Motivators Report For: Diaz SetiadiDocument14 pagesDisc & Motivators Report For: Diaz SetiadidzhzrnNo ratings yet
- Spotify Top Track Generator: Last 6 MonthsDocument1 pageSpotify Top Track Generator: Last 6 MonthsdzhzrnNo ratings yet
- Significantly Increased Risk of All-Cause Mortality Among Cardiac Patients Feeling LonelyDocument7 pagesSignificantly Increased Risk of All-Cause Mortality Among Cardiac Patients Feeling LonelydzhzrnNo ratings yet
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Sturge-Weber Syndrome. Study of 55 PatientsDocument7 pagesSturge-Weber Syndrome. Study of 55 PatientsdzhzrnNo ratings yet
- The Pathogenesis of Port Wine Stain and Sturge Weber Syndrome: Complex Interactions Between Genetic Alterations and Aberrant MAPK and PI3K ActivationDocument17 pagesThe Pathogenesis of Port Wine Stain and Sturge Weber Syndrome: Complex Interactions Between Genetic Alterations and Aberrant MAPK and PI3K ActivationdzhzrnNo ratings yet
- Sturge Weber SyndromeDocument6 pagesSturge Weber SyndromedzhzrnNo ratings yet
- The "Reptilian" - Triune Brain - The Origins of A Misguided Idea - Emotion & Cognition and The Brain, by Luiz PessoaDocument6 pagesThe "Reptilian" - Triune Brain - The Origins of A Misguided Idea - Emotion & Cognition and The Brain, by Luiz PessoaJ. Félix Angulo RascoNo ratings yet
- Migraine Aura - Pathophysiology, Mimics, and TratamentDocument10 pagesMigraine Aura - Pathophysiology, Mimics, and Tratamentrafael rocha novaes100% (1)
- Psy 03 Biopsychology-Ch. 8 Sensorimotor SystemDocument1 pagePsy 03 Biopsychology-Ch. 8 Sensorimotor SystemMitch Shyrelle BaclaoNo ratings yet
- Music and Brain Circuitry Strategies For StrengtheningDocument10 pagesMusic and Brain Circuitry Strategies For Strengtheningbiahonda15No ratings yet
- K8a Anatomi Sistem Saraf PusatDocument87 pagesK8a Anatomi Sistem Saraf Pusathartinissa vaniaNo ratings yet
- Human Physiology From Cells To Systems 9th Edition Sherwood Solutions ManualDocument12 pagesHuman Physiology From Cells To Systems 9th Edition Sherwood Solutions ManualSamanthaStuartijgt100% (40)
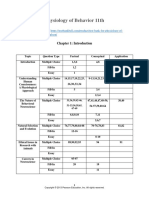
- Test Bank For Physiology of Behavior 11th Edition by CarlsonDocument45 pagesTest Bank For Physiology of Behavior 11th Edition by CarlsonThomas White100% (26)
- Fuster 2001Document15 pagesFuster 2001Jane SmithNo ratings yet
- 5 - The Visual System and Mechanisms of PerceptionDocument13 pages5 - The Visual System and Mechanisms of PerceptionElmer SalazarNo ratings yet
- Emotion, Memory and The BrainDocument9 pagesEmotion, Memory and The Brainbarrylyndon1967No ratings yet
- Biological Basis of BehaviorDocument6 pagesBiological Basis of BehaviorLyanna MormontNo ratings yet
- General NosologyDocument13 pagesGeneral Nosologyyasingada100% (1)
- Brain StudyDocument57 pagesBrain StudyJoeNo ratings yet
- Beta-Oscillations Reflect Recovery in Subacute Stroke NNR 20200511Document13 pagesBeta-Oscillations Reflect Recovery in Subacute Stroke NNR 20200511yafangNo ratings yet
- Brainsci 09 00068 v2Document20 pagesBrainsci 09 00068 v2RobertoVargasPérezNo ratings yet
- Nano BotsDocument31 pagesNano Botspradeepagarwal62No ratings yet
- Functional Areas of Cerebral CortexDocument3 pagesFunctional Areas of Cerebral CortexMatet MonjeNo ratings yet
- Adonis Quintero Linguistic DictionaryDocument20 pagesAdonis Quintero Linguistic DictionaryMax No MeloNo ratings yet
- Brain AnatomyDocument2 pagesBrain AnatomyÖzge ŞenNo ratings yet
- Need Motivates The Behaviour of A Person.: Human Needs TheoryDocument8 pagesNeed Motivates The Behaviour of A Person.: Human Needs TheoryDan Ataniel EnsaladaNo ratings yet
- Visual PathwayDocument24 pagesVisual PathwayAkshara Eye FoundationNo ratings yet
- 100 Days of Sunlight by Abbie EmmonsDocument315 pages100 Days of Sunlight by Abbie EmmonsJessie Ann Aquino100% (11)
- Motor PlanningDocument30 pagesMotor PlanningkalbaliNo ratings yet
- Identify The Part of The BrainDocument2 pagesIdentify The Part of The BrainClement Mar ClimacoNo ratings yet
- EEG-Based Emotion RecognitionDocument17 pagesEEG-Based Emotion RecognitionbmakworoNo ratings yet
- Neurological Considerations 1966 PDFDocument1 pageNeurological Considerations 1966 PDFWahyuni SusantiNo ratings yet
- Solutions Manual Ch. 11 and 12 - Test BankDocument9 pagesSolutions Manual Ch. 11 and 12 - Test BankSally RiverNo ratings yet
- N - I. A - P: Eurotransmisores DEL Sistema Límbico Mígdala Rimera ParteDocument6 pagesN - I. A - P: Eurotransmisores DEL Sistema Límbico Mígdala Rimera ParteghgfchmNo ratings yet
- Neuromodulation by Means of Electrical Brain Stimulation: AbstractsDocument5 pagesNeuromodulation by Means of Electrical Brain Stimulation: AbstractsmoiNo ratings yet
- Central Vestibular PathwayDocument22 pagesCentral Vestibular PathwayPutri Noursyarief Maharanny NasutionNo ratings yet