You might also like
- Understanding Non-Hodgkin Lymphoma. A Guide for Patients, Survivors, and Loved Ones. April 2021From EverandUnderstanding Non-Hodgkin Lymphoma. A Guide for Patients, Survivors, and Loved Ones. April 2021No ratings yet
- Migraine Case StudyDocument15 pagesMigraine Case StudyJean LaiNo ratings yet
- List of Essential Medicine For Adult in Rwanda PDFDocument60 pagesList of Essential Medicine For Adult in Rwanda PDFShandy B100% (1)
- Gribben, 2011 AlemtDocument7 pagesGribben, 2011 AlemtveraffulNo ratings yet
- LNH T PerifericoDocument10 pagesLNH T PerifericopasqualijNo ratings yet
- Novel Therapies For Chronic Leukaemia Blood Rev 2004Document12 pagesNovel Therapies For Chronic Leukaemia Blood Rev 2004Alexis May UcNo ratings yet
- CLL Treatment Advances with Chemoimmunotherapy & Targeted AgentsDocument8 pagesCLL Treatment Advances with Chemoimmunotherapy & Targeted AgentsSri IriantiNo ratings yet
- HITCLLDocument9 pagesHITCLLapi-26302710No ratings yet
- Acute Myeloid Leukemia...Document20 pagesAcute Myeloid Leukemia...hemendre0% (1)
- Current and Emerging Therapies For Acute Myeloid LeukemiaDocument22 pagesCurrent and Emerging Therapies For Acute Myeloid LeukemiaRutuja KuhikarNo ratings yet
- Monoclonal Antibodies New Chance in The Management of B Cell Acute Lymphoblastic LeukemiaDocument12 pagesMonoclonal Antibodies New Chance in The Management of B Cell Acute Lymphoblastic LeukemiaMayra AlejandraNo ratings yet
- Acute Leukemia ThesisDocument8 pagesAcute Leukemia Thesisafcnftqep100% (2)
- Wall 2016Document15 pagesWall 2016Jose AbadiaNo ratings yet
- The Risk Factors For CLL, Including The Relevance of Monoclonal B Cell Lymphocytosis (MBL)Document7 pagesThe Risk Factors For CLL, Including The Relevance of Monoclonal B Cell Lymphocytosis (MBL)Fahim MahmudNo ratings yet
- How I Treat Acute Myeloid LeukemiaDocument10 pagesHow I Treat Acute Myeloid LeukemiaSutiara Prihatining TyasNo ratings yet
- 1) Explain The Risk Factors For CLL, Including The Relevance of Monoclonal B Cell Lymphocytosis (MBL)Document6 pages1) Explain The Risk Factors For CLL, Including The Relevance of Monoclonal B Cell Lymphocytosis (MBL)Fahim MahmudNo ratings yet
- Cancer - February 1974 - Knospe - Bi Weekly Chlorambucil Treatment of Chronic Lymphocytic LeukemiaDocument8 pagesCancer - February 1974 - Knospe - Bi Weekly Chlorambucil Treatment of Chronic Lymphocytic LeukemiaJohn chuksNo ratings yet
- Cancer - 2006 - Tsimberidou - Outcomes in Patients With Splenic Marginal Zone Lymphoma and Marginal Zone Lymphoma TreatedDocument11 pagesCancer - 2006 - Tsimberidou - Outcomes in Patients With Splenic Marginal Zone Lymphoma and Marginal Zone Lymphoma TreatedAvinash TaleleNo ratings yet
- How I Treat Newly Diagnosed Chronic Phase CMLDocument9 pagesHow I Treat Newly Diagnosed Chronic Phase CMLDenisse SarabiaNo ratings yet
- Acute Lymphoblastic Leukemia Research PaperDocument6 pagesAcute Lymphoblastic Leukemia Research Paperafeavbrpd100% (1)
- Biology Investigatory Project on Chronic Myeloid LeukemiaDocument16 pagesBiology Investigatory Project on Chronic Myeloid LeukemiaABHISHEK AjithkumarNo ratings yet
- Mantle Cell Lymphoma ThesisDocument7 pagesMantle Cell Lymphoma Thesisgjdpj4jq100% (1)
- SinopsisDocument7 pagesSinopsisbee yournitaNo ratings yet
- Acute Myeloid Leukemia ThesisDocument5 pagesAcute Myeloid Leukemia ThesisBuyCheapEssayOmaha100% (2)
- ZH 800210000187Document11 pagesZH 800210000187Francieudo SampaioNo ratings yet
- Relapsed Acute Myeloid Leukemia in Children and Adolescents: Current Treatment Options and Future StrategiesDocument10 pagesRelapsed Acute Myeloid Leukemia in Children and Adolescents: Current Treatment Options and Future StrategiesYo MeNo ratings yet
- Extracellular Nucleic Acids and Cancer: Michael - Fleischhacker@uk-Halle - de Bernd - Schmidt@uk-Halle - deDocument55 pagesExtracellular Nucleic Acids and Cancer: Michael - Fleischhacker@uk-Halle - de Bernd - Schmidt@uk-Halle - deAirin LeonieNo ratings yet
- Reviews: Chronic Lymphocytic Leukaemia: From Genetics To TreatmentDocument18 pagesReviews: Chronic Lymphocytic Leukaemia: From Genetics To Treatmentlengers poworNo ratings yet
- Chronic lymphocytic leukaemia genetics and treatment insightsDocument18 pagesChronic lymphocytic leukaemia genetics and treatment insightslengers poworNo ratings yet
- Prognostic Factors For Chronic Lymphocytic LeukemiaDocument6 pagesPrognostic Factors For Chronic Lymphocytic LeukemiaJose AbadiaNo ratings yet
- 1857 FullDocument6 pages1857 FullTahniat AishaNo ratings yet
- Central Nervous Disease in Pediatric Patients LLADocument5 pagesCentral Nervous Disease in Pediatric Patients LLAlaura rangelNo ratings yet
- 4048 FullDocument6 pages4048 FullIlincaNo ratings yet
- Cells 11 02257Document17 pagesCells 11 02257IraBautyDwiOctaviaNo ratings yet
- Personalized Cancer Care B. Wilson, UsydDocument13 pagesPersonalized Cancer Care B. Wilson, UsydJacob BrownNo ratings yet
- JCM 08 01175 v2 PDFDocument28 pagesJCM 08 01175 v2 PDFAs'har AnwarNo ratings yet
- MR 25Document9 pagesMR 25Riko JumattullahNo ratings yet
- TH LeukemiaDocument8 pagesTH Leukemiaأحمد علي حبيبNo ratings yet
- Review ArticleDocument9 pagesReview ArticleJeronim H'gharNo ratings yet
- Tmp9a87 TMPDocument3 pagesTmp9a87 TMPFrontiersNo ratings yet
- A Critical History of Chromic Myeloid LeukemiaDocument3 pagesA Critical History of Chromic Myeloid LeukemiaRiko JumattullahNo ratings yet
- Dissertation LeukemiaDocument4 pagesDissertation LeukemiaCustomPapersOnlineSaltLakeCity100% (1)
- Tratamento HodgkinDocument15 pagesTratamento HodgkinIsabella Claudino FernandesNo ratings yet
- Managing Cancer Therapy and Supportive CareDocument2 pagesManaging Cancer Therapy and Supportive CareOlive ThereseNo ratings yet
- Adoptive Transfer of Natural Killer Cells in Combination With Chemotherapy Improves Outcomes of Patients With Locally Advanced Colon Carcinoma.Document15 pagesAdoptive Transfer of Natural Killer Cells in Combination With Chemotherapy Improves Outcomes of Patients With Locally Advanced Colon Carcinoma.Andrew ChenNo ratings yet
- 10 1016@j Hoc 2019 03 006-2Document12 pages10 1016@j Hoc 2019 03 006-2Bruna AngeloNo ratings yet
- 368 FTP PDFDocument9 pages368 FTP PDFlPiNGUSlNo ratings yet
- Detection of Minimal Residual Disease in AcuteLeukemia by Flow CytometryDocument15 pagesDetection of Minimal Residual Disease in AcuteLeukemia by Flow Cytometrymilica cucuzNo ratings yet
- Thesis Statement On Leukemia CancerDocument5 pagesThesis Statement On Leukemia Cancerjuliemooreknoxville100% (2)
- Chronic Myeloid Leukemia Dissertation ThesisDocument7 pagesChronic Myeloid Leukemia Dissertation Thesiswendyboydsaintpetersburg100% (2)
- 5446.full 2Document12 pages5446.full 2malik003No ratings yet
- Crohn ReviewDocument39 pagesCrohn Reviewdrkoral751No ratings yet
- Diagnostic Workup and Pathophysiology of Pre-B-Cell Acute Lymphoblastic LeukemiaDocument3 pagesDiagnostic Workup and Pathophysiology of Pre-B-Cell Acute Lymphoblastic LeukemiaNitin KumarNo ratings yet
- Chronic Leukemia Treatment and Diagnosis GuideDocument12 pagesChronic Leukemia Treatment and Diagnosis GuideJuan RamirezNo ratings yet
- Drug Repurposing For The Treatment of Acute Myeloid LeukemiaDocument11 pagesDrug Repurposing For The Treatment of Acute Myeloid LeukemiaMini Bekti NingsihNo ratings yet
- Drugs Used in CancerDocument46 pagesDrugs Used in CancerRENTI NOVITANo ratings yet
- Vivia BiotechDocument10 pagesVivia Biotech11 11No ratings yet
- LLC 2006Document11 pagesLLC 2006claudia8a_ulamedNo ratings yet
- In Vitro Drug Sensitivity Testing for CLL TreatmentsDocument17 pagesIn Vitro Drug Sensitivity Testing for CLL Treatmentskj185No ratings yet
- Avances en Leucemias AgudasDocument20 pagesAvances en Leucemias AgudasMayra Alejandra Prada SerranoNo ratings yet
- Prognostic Factors in Non-Hodgkin LymphomaDocument8 pagesPrognostic Factors in Non-Hodgkin Lymphomaraio interionfashionNo ratings yet
- Understanding Non-Hodgkin Lymphoma. A Guide for Patients, Survivors, and Loved Ones. September 2015From EverandUnderstanding Non-Hodgkin Lymphoma. A Guide for Patients, Survivors, and Loved Ones. September 2015No ratings yet
- Problemes Biomol Sessi 1Document5 pagesProblemes Biomol Sessi 1Jose Angel AbadíaNo ratings yet
- Leucemia Linfoide CrónicaDocument17 pagesLeucemia Linfoide CrónicaJose AbadiaNo ratings yet
- Mono 114Document511 pagesMono 114Jose Angel AbadíaNo ratings yet
- Tees 2016Document39 pagesTees 2016Jose Angel AbadíaNo ratings yet
- The Endocrine SystemDocument45 pagesThe Endocrine SystemJose Angel AbadíaNo ratings yet
- Luczynska 2013Document12 pagesLuczynska 2013Jose Angel AbadíaNo ratings yet
- Red and Processed Meat Consumption Increases Risk For Non-Hodgkin LymphomaDocument11 pagesRed and Processed Meat Consumption Increases Risk For Non-Hodgkin LymphomaJose AbadiaNo ratings yet
- Chronic Lymphocytic Leukemia (CLL) - Then and Now: Critical ReviewDocument11 pagesChronic Lymphocytic Leukemia (CLL) - Then and Now: Critical ReviewJose Angel AbadíaNo ratings yet
- Ni Hms 609492Document19 pagesNi Hms 609492Jose AbadiaNo ratings yet
- Obesidad y LinfomasDocument10 pagesObesidad y LinfomasJose Angel AbadíaNo ratings yet
- Chronic lymphocytic leukemia overview and treatment advancesDocument53 pagesChronic lymphocytic leukemia overview and treatment advancesJose Angel AbadíaNo ratings yet
- Rodrguez Vicente 2013Document14 pagesRodrguez Vicente 2013Jose AbadiaNo ratings yet
- Maly 2016Document9 pagesMaly 2016Jose Angel AbadíaNo ratings yet
- APJCP Volume 15 Issue 23 Pages 10421-10425Document5 pagesAPJCP Volume 15 Issue 23 Pages 10421-10425Jose AbadiaNo ratings yet
- Nut 14201074Document7 pagesNut 14201074Jose AbadiaNo ratings yet
- Kemp in 2013Document12 pagesKemp in 2013Jose Angel AbadíaNo ratings yet
- Daniel 2012Document7 pagesDaniel 2012Jose Angel AbadíaNo ratings yet
- Research: Diet and Non-Hodgkin's Lymphoma RiskDocument12 pagesResearch: Diet and Non-Hodgkin's Lymphoma RiskJose AbadiaNo ratings yet
- Fruta y VegetalesDocument28 pagesFruta y VegetalesJose Angel AbadíaNo ratings yet
- Dieta y CancerDocument11 pagesDieta y CancerJose Angel AbadíaNo ratings yet
- Parik H 2016Document35 pagesParik H 2016Jose Angel AbadíaNo ratings yet
- Phytanic Acid and The Risk of Non-Hodgkin LymphomaDocument6 pagesPhytanic Acid and The Risk of Non-Hodgkin LymphomaJose Angel AbadíaNo ratings yet
- Dietary Factors and Risk of Non-Hodgkin Lymphoma in Men and WomenDocument10 pagesDietary Factors and Risk of Non-Hodgkin Lymphoma in Men and WomenJose Angel AbadíaNo ratings yet
- Intakes of Fruits, Vegetables, and Related Nutrients and The Risk of Non-Hodgkin's Lymphoma Among WomenDocument10 pagesIntakes of Fruits, Vegetables, and Related Nutrients and The Risk of Non-Hodgkin's Lymphoma Among WomenJose Angel AbadíaNo ratings yet
- Rows Well Turner 2017Document5 pagesRows Well Turner 2017Jose AbadiaNo ratings yet
- Dietary Factors of One-Carbon Metabolism in Relation To Non-Hodgkin Lymphoma and Multiple Myeloma in A Cohort of Male SmokersDocument7 pagesDietary Factors of One-Carbon Metabolism in Relation To Non-Hodgkin Lymphoma and Multiple Myeloma in A Cohort of Male SmokersJose AbadiaNo ratings yet
- Fruta y LinfomaDocument15 pagesFruta y LinfomaJose Angel AbadíaNo ratings yet
- Tees 2016Document39 pagesTees 2016Jose Angel AbadíaNo ratings yet
- Etiologic Heterogeneity Among Non-Hodgkin Lymphoma Subtypes: The Interlymph Non-Hodgkin Lymphoma Subtypes ProjectDocument15 pagesEtiologic Heterogeneity Among Non-Hodgkin Lymphoma Subtypes: The Interlymph Non-Hodgkin Lymphoma Subtypes ProjectJose AbadiaNo ratings yet
- NIH Public Access: Author ManuscriptDocument9 pagesNIH Public Access: Author ManuscriptJose Angel AbadíaNo ratings yet
- Endotracheal Intubation GuideDocument4 pagesEndotracheal Intubation Guiderupali gahalianNo ratings yet
- Deal 22 03 21Document45 pagesDeal 22 03 21serinyaNo ratings yet
- Orange BookDocument70 pagesOrange BookAIMANIBRAHIM82No ratings yet
- Essential Medicines ListDocument12 pagesEssential Medicines ListAZGH HOSPITAL /Cyberdyne PhilippinesNo ratings yet
- Stenorol® Crypto - OS - Brochure - EN - v01 - 1020Document2 pagesStenorol® Crypto - OS - Brochure - EN - v01 - 1020DrivailaNo ratings yet
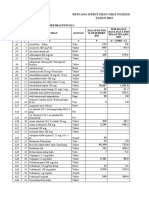
- Rencana Kebutuhan Obat Puskesmas Tahun 2023Document33 pagesRencana Kebutuhan Obat Puskesmas Tahun 2023Putu LitariNo ratings yet
- The Rolle of Surgery in Oncology: Surgery Departement Medical Faculty Ukrida UniversityDocument25 pagesThe Rolle of Surgery in Oncology: Surgery Departement Medical Faculty Ukrida UniversityGian Alodia RisamasuNo ratings yet
- Acupuncture in India:: As Defined by The National Institutes of HealthDocument3 pagesAcupuncture in India:: As Defined by The National Institutes of Healthmanikandan16No ratings yet
- 1968 Long-Term Total Parenteral Nutrition With Growth, Development, and Positive Nitrogen Balance. SURGERYDocument4 pages1968 Long-Term Total Parenteral Nutrition With Growth, Development, and Positive Nitrogen Balance. SURGERYChristine ChambersNo ratings yet
- PPPL Rejected Expiry 10 - Sep - 2019Document34 pagesPPPL Rejected Expiry 10 - Sep - 2019ANANTHA BABU ANo ratings yet
- TabletDocument29 pagesTabletmelawatiNo ratings yet
- Annotated BibliographyDocument6 pagesAnnotated Bibliographyapi-355989353No ratings yet
- Module-Intradermal Etool PDFDocument7 pagesModule-Intradermal Etool PDFErika Danalle ArceoNo ratings yet
- Production of Affordable ChemotherapyDocument27 pagesProduction of Affordable ChemotherapyIndonesian Journal of CancerNo ratings yet
- Spotlight On Cardiac DrugsDocument2 pagesSpotlight On Cardiac Drugspauerish100% (2)
- Hormonal TherapiesDocument39 pagesHormonal TherapiesJalal EltabibNo ratings yet
- Pharmacology '' Routes of Administration #Local RouteDocument13 pagesPharmacology '' Routes of Administration #Local RouteNitin NawaleNo ratings yet
- Understanding Spirometry: Diagnosing and Monitoring Lung DiseaseDocument68 pagesUnderstanding Spirometry: Diagnosing and Monitoring Lung Diseasex22xNo ratings yet
- Historical Perspective of CDDSDocument3 pagesHistorical Perspective of CDDSHemant BhattNo ratings yet
- LAPAROSCOPIC SURGERyDocument37 pagesLAPAROSCOPIC SURGERyabraham winartoNo ratings yet
- The Laboratory of Pharmacokinetics, Dept. of Pharmacy, University of PatrasDocument1 pageThe Laboratory of Pharmacokinetics, Dept. of Pharmacy, University of PatrasnosfarNo ratings yet
- Psychopharmacology Is The Study of Drug-Induced Changes in Mood, Sensation, ThinkingDocument5 pagesPsychopharmacology Is The Study of Drug-Induced Changes in Mood, Sensation, Thinking0921pyNo ratings yet
- Insulin Lecture For RHUDocument13 pagesInsulin Lecture For RHUCJ BunoanNo ratings yet
- Kajian Hukum Peran Apoteker Dalam Saintifikasi JamuDocument6 pagesKajian Hukum Peran Apoteker Dalam Saintifikasi JamuNavisa HaifaNo ratings yet
- FDA Safety AlertsDocument166 pagesFDA Safety AlertsChris HartoyoNo ratings yet
- SHC ABX Dosing GuideDocument6 pagesSHC ABX Dosing GuideMinhNo ratings yet
- Skrining ResepDocument8 pagesSkrining ResephanifakhNo ratings yet
- Pharmaceutical Jurisprudence & Ethics Answer Key-RED PACOPDocument20 pagesPharmaceutical Jurisprudence & Ethics Answer Key-RED PACOPMelbhon Fabro RamosNo ratings yet