You might also like
- Concise Clinical Review: Chronic Bronchitis and Chronic Obstructive Pulmonary DiseaseDocument10 pagesConcise Clinical Review: Chronic Bronchitis and Chronic Obstructive Pulmonary DiseaseMuhammad FakhruriNo ratings yet
- Choudhury 2014Document30 pagesChoudhury 2014Andry Wahyudi AgusNo ratings yet
- Coagulation Dysfunction in Patients With AECOPD and ItsDocument6 pagesCoagulation Dysfunction in Patients With AECOPD and ItsAndreea MoalesNo ratings yet
- Copd and CVD Pulmonology JournalDocument9 pagesCopd and CVD Pulmonology JournalKessi VikaneswariNo ratings yet
- Chronic Bronchitis and COPDDocument11 pagesChronic Bronchitis and COPDRodli AkbarNo ratings yet
- Copd and Cardiovascular Disease: Original ArticleDocument9 pagesCopd and Cardiovascular Disease: Original Articlemgoez077No ratings yet
- Association Between Right Heart Failure and Hospital Mortality in Exacerbation of COPDDocument6 pagesAssociation Between Right Heart Failure and Hospital Mortality in Exacerbation of COPDJOSE ALBEIRO RIATIVA TORRESNo ratings yet
- Issue 4Document3 pagesIssue 4gineshaNo ratings yet
- COPD and Pulmonary Thromboembolism (For Galley Proof)Document6 pagesCOPD and Pulmonary Thromboembolism (For Galley Proof)Ram AdhikariNo ratings yet
- Pulmonary Hypertension in COPD: Hypoxic VasoconstrictionDocument5 pagesPulmonary Hypertension in COPD: Hypoxic VasoconstrictionRazvan PredaNo ratings yet
- Obesity Lung COPDDocument8 pagesObesity Lung COPDDumitru BiniucNo ratings yet
- Vias Moleculares HapDocument24 pagesVias Moleculares Hapdayanachuquimia95No ratings yet
- bollenbecker-et-al-2022-lung-kidney-interactions-and-their-role-in-chronic-kidney-disease-associated-pulmonary-diseasesDocument16 pagesbollenbecker-et-al-2022-lung-kidney-interactions-and-their-role-in-chronic-kidney-disease-associated-pulmonary-diseaseshilyalivaNo ratings yet
- (2247059X - Pneumologia) Asthma-COPD-Bronchiectasis Combination - An Unstudied TripletDocument3 pages(2247059X - Pneumologia) Asthma-COPD-Bronchiectasis Combination - An Unstudied TripletConstantin PopescuNo ratings yet
- Epidemiology and Risk Factors in CKD Patients With Pulmonary HypertensionDocument8 pagesEpidemiology and Risk Factors in CKD Patients With Pulmonary HypertensionshaheershayanqaziNo ratings yet
- Chronic Obstructive Pulmonary Disease and Diabetes MellitusDocument19 pagesChronic Obstructive Pulmonary Disease and Diabetes MellitusMirza RisqaNo ratings yet
- Cardiovascular Comorbidities in Chronic Obstructive Pulmonary Disease (COPD) - Current Considerations For Clinical PracticeDocument14 pagesCardiovascular Comorbidities in Chronic Obstructive Pulmonary Disease (COPD) - Current Considerations For Clinical Practicerbatjun576No ratings yet
- Chronic Obstructive Pulmonary DiseaseDocument8 pagesChronic Obstructive Pulmonary DiseaseGeozel VivienneNo ratings yet
- Chronic Obstructive Pulmonary Disease in Elderly PatientsDocument14 pagesChronic Obstructive Pulmonary Disease in Elderly PatientsFranz MiguelNo ratings yet
- Presentasi Jurnal Interna: Hubungan PPOK Dengan Gagal JantungDocument19 pagesPresentasi Jurnal Interna: Hubungan PPOK Dengan Gagal Jantungasep budiyantoNo ratings yet
- COPD ExacerbationDocument12 pagesCOPD ExacerbationJeffrey ShermanNo ratings yet
- Pulmonary Tuberculosis and Its Haematological Correlates-1Document8 pagesPulmonary Tuberculosis and Its Haematological Correlates-1mentari_64No ratings yet
- Copd Nihilismo BuenisimoDocument8 pagesCopd Nihilismo BuenisimoJose Lopez FuentesNo ratings yet
- Assessment of Cardiovascular Changes Among Chronic Obstructive Pulmonary Disease Patients at Rural Tertiary Care Center of Northern IndiaDocument5 pagesAssessment of Cardiovascular Changes Among Chronic Obstructive Pulmonary Disease Patients at Rural Tertiary Care Center of Northern IndiaKarthik SNo ratings yet
- 956 FullDocument7 pages956 FullayuNo ratings yet
- Medical Progress: C O P DDocument12 pagesMedical Progress: C O P DPablo CamposNo ratings yet
- Acute Exacerbation of Chronic Obstructive Pulmonary DiseaseDocument5 pagesAcute Exacerbation of Chronic Obstructive Pulmonary Diseaseteguh sNo ratings yet
- COPD As An Endothelial Disorder Endothelial Injury LinkingDocument18 pagesCOPD As An Endothelial Disorder Endothelial Injury LinkingAndreea MoalesNo ratings yet
- Copd 4 PDFDocument5 pagesCopd 4 PDFcornelia cindy SRDNo ratings yet
- Acute Lung InjuryDocument5 pagesAcute Lung InjuryKinanti Devia LarasatiNo ratings yet
- Imun Copd 2019Document12 pagesImun Copd 2019Amilia FrayantyNo ratings yet
- Obstructive Sleep Apnea in Chronic Obstructive PulmonaryDocument5 pagesObstructive Sleep Apnea in Chronic Obstructive PulmonaryGeorge Cătălin AlexandruNo ratings yet
- Transfusion-Related Acute Lung Injury: Free Research Articles Transfusion MedicineDocument9 pagesTransfusion-Related Acute Lung Injury: Free Research Articles Transfusion MedicineDiana AstariNo ratings yet
- Medicina: Pulmonary Hypertension in COPD: A Case Study and Review of The LiteratureDocument8 pagesMedicina: Pulmonary Hypertension in COPD: A Case Study and Review of The Literatureguhan taraNo ratings yet
- Hipertension PulmonarDocument5 pagesHipertension Pulmonarkarla lozadaNo ratings yet
- Fonc 11 640999Document13 pagesFonc 11 640999desconocido 123 ambticonNo ratings yet
- Concise Clinical Review: Non-Cystic Fibrosis BronchiectasisDocument11 pagesConcise Clinical Review: Non-Cystic Fibrosis BronchiectasisJuwitaNo ratings yet
- Biomarker Copd PDFDocument35 pagesBiomarker Copd PDFManoj KumarNo ratings yet
- ANEMIA P ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Document7 pagesANEMIA P ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Arv IraNo ratings yet
- 5g-Tantangan Terapi HF & COPDDocument6 pages5g-Tantangan Terapi HF & COPDsukiyantoNo ratings yet
- 2019 - Chronic Obstructive Pulmonary Disease andDocument6 pages2019 - Chronic Obstructive Pulmonary Disease andAndreea MoalesNo ratings yet
- Transfusion-Related Acute Lung Injury: HistoryDocument20 pagesTransfusion-Related Acute Lung Injury: HistoryBladimir CentenoNo ratings yet
- The Influence of Anemia On One-Year Exacerbation Rate of Patients With COPD-PHDocument8 pagesThe Influence of Anemia On One-Year Exacerbation Rate of Patients With COPD-PHrinzNo ratings yet
- Metoprolol y El EPOCDocument10 pagesMetoprolol y El EPOCMadyurit RamírezNo ratings yet
- Medical Progress: C O P DDocument12 pagesMedical Progress: C O P DglaysonvelNo ratings yet
- FPI Progn TratDocument13 pagesFPI Progn TratTurcu AndreeaNo ratings yet
- Emboli Paru & PPOKDocument7 pagesEmboli Paru & PPOKsukiyantoNo ratings yet
- 2019 Article 181Document7 pages2019 Article 181gede suryaNo ratings yet
- Hypertension & CancerDocument7 pagesHypertension & CancerAndi Khomeini Takdir HaruniNo ratings yet
- Angiogenesis and CopdDocument10 pagesAngiogenesis and CopdDonytra Arby WardhanaNo ratings yet
- Submitted - Manuscript - Red FontDocument20 pagesSubmitted - Manuscript - Red FontKartik DeshmukhNo ratings yet
- Copd 2Document26 pagesCopd 2Abid SunhanNo ratings yet
- Proteome Profiling of Lung Tissues in ChronicDocument8 pagesProteome Profiling of Lung Tissues in ChronicAndreea MoalesNo ratings yet
- Chest: Cardiovascular Comorbidity in COPDDocument16 pagesChest: Cardiovascular Comorbidity in COPDAndry Wahyudi AgusNo ratings yet
- Bilateral Massive Pulmonary Embolism Secondary To Decompression Sickness: A Case ReportDocument4 pagesBilateral Massive Pulmonary Embolism Secondary To Decompression Sickness: A Case ReportPatricio Toledo FuenzalidaNo ratings yet
- Hematological Findings and Complications of COVID-19: AffiliationsDocument32 pagesHematological Findings and Complications of COVID-19: Affiliationsnicky_kelly_3No ratings yet
- Pathophysiology of COPDDocument4 pagesPathophysiology of COPDrinieeeNo ratings yet
- Review Article: The Cardiorenal Syndrome: A ReviewDocument11 pagesReview Article: The Cardiorenal Syndrome: A ReviewrezykurniaNo ratings yet
- The Systemic Face of Airway Diseases: The Role of C-Reactive ProteinDocument3 pagesThe Systemic Face of Airway Diseases: The Role of C-Reactive ProteinHarli FeryadiNo ratings yet
- Secondary HypertensionFrom EverandSecondary HypertensionAlberto MorgantiNo ratings yet
- Free PPT Templates: Insert The Title of Your Presentation HereDocument3 pagesFree PPT Templates: Insert The Title of Your Presentation HereeffendyNo ratings yet
- Kimed 1 Parameter BDocument3 pagesKimed 1 Parameter BSabda KartikaNo ratings yet
- Structure and Bonding of Mefenamic AcidDocument5 pagesStructure and Bonding of Mefenamic AcidSabda KartikaNo ratings yet
- Kelp 3Document11 pagesKelp 3Sabda KartikaNo ratings yet
- Struktur Tidak Stabil: Energi Minimum Asam MefenamatDocument5 pagesStruktur Tidak Stabil: Energi Minimum Asam MefenamatSabda KartikaNo ratings yet
- Phenobarbital Structure and EnergyDocument8 pagesPhenobarbital Structure and EnergySabda KartikaNo ratings yet
- AABB Antibody IdentificationDocument66 pagesAABB Antibody IdentificationDevie Mara67% (3)
- Chapter 17 Anatomy and Physiology NotesDocument10 pagesChapter 17 Anatomy and Physiology NotesZachary WatsonNo ratings yet
- Cardiovascular EnduranceDocument7 pagesCardiovascular EnduranceFrancine ValdezNo ratings yet
- Physiology and Injuries in Sports: Unit - 7Document33 pagesPhysiology and Injuries in Sports: Unit - 7Vansh GoyalNo ratings yet
- Set 7 QnaDocument13 pagesSet 7 QnaRebornNgNo ratings yet
- Deconditioning SyndromeDocument62 pagesDeconditioning SyndromeSheikha Khadijah50% (2)
- Ravenloft - Van Richten's GuideDocument484 pagesRavenloft - Van Richten's GuideВиталий Артюшкин100% (2)
- CHI and Water Bending ChiniseDocument11 pagesCHI and Water Bending ChiniseThe PirateNo ratings yet
- NBS 2021 Program - Updated May 13Document1 pageNBS 2021 Program - Updated May 13CBR UBCNo ratings yet
- Form 3 Ujian Rasmi 1 2019 (2) SueDocument10 pagesForm 3 Ujian Rasmi 1 2019 (2) Suesuraya nazaNo ratings yet
- R138911 Amit Kumar 300822180312Document3 pagesR138911 Amit Kumar 300822180312amit kumarNo ratings yet
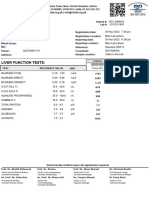
- Liver Function Tests:: SajidaDocument1 pageLiver Function Tests:: Sajidaufaqnavid29No ratings yet
- ASH Hematology Review Series - Hemophilia and Other Factor DeficienciesDocument66 pagesASH Hematology Review Series - Hemophilia and Other Factor Deficienciesdr israrNo ratings yet
- GLC in Depth Sudy of A Moral Issue Example V4eDocument2 pagesGLC in Depth Sudy of A Moral Issue Example V4eapi-272879715No ratings yet
- Intermediate Model Question PapersDocument143 pagesIntermediate Model Question PapersPrakash KumarNo ratings yet
- NEJM vonWDDocument14 pagesNEJM vonWDMonica Aleja FernándezNo ratings yet
- SGL 2 (Hemolytic Anemia & Hemoglobinopathies)Document53 pagesSGL 2 (Hemolytic Anemia & Hemoglobinopathies)raman mahmudNo ratings yet
- RBC SeminarDocument80 pagesRBC SeminarSourav Ron BoseNo ratings yet
- F3 Topic 11 & 12 PracticeDocument10 pagesF3 Topic 11 & 12 PracticePianna IeongNo ratings yet
- Ans KeysDocument11 pagesAns KeysMuhammad Talha TayyebNo ratings yet
- Automation in HaematologyDocument67 pagesAutomation in Haematologyk11a1r18No ratings yet
- Catalogo Nuevo GboDocument7 pagesCatalogo Nuevo GboCaro ErazoNo ratings yet
- Parvati Tripathi - Female - 62 - 2022 - 12Document13 pagesParvati Tripathi - Female - 62 - 2022 - 12Rajeev TripathiNo ratings yet
- RMLHDocument1 pageRMLHAsmaa DarwishNo ratings yet
- Summative Test Q2Document9 pagesSummative Test Q2Jing Pelingon CartenNo ratings yet
- Fingerprint Identification Pre-Board Exam ReviewDocument4 pagesFingerprint Identification Pre-Board Exam ReviewAngelica MadayagNo ratings yet
- 3rd Year Survival Guide TipsDocument15 pages3rd Year Survival Guide TipsTravelle Franklin-Ford EllisNo ratings yet
- CompleteBloodCounts NORMAL VALUEDocument4 pagesCompleteBloodCounts NORMAL VALUEWoro Hapsari Wahyuningrum100% (1)
- AcknowledgementDocument9 pagesAcknowledgementJovin AshickNo ratings yet
- Lesson 2Document26 pagesLesson 2Janielle FajardoNo ratings yet