You might also like
- Mechanical Ventilation Made EasyDocument5 pagesMechanical Ventilation Made EasypraveenbhavniNo ratings yet
- Westmead Obstetric Anaesthesia Manual 2020Document72 pagesWestmead Obstetric Anaesthesia Manual 2020DavidNo ratings yet
- Assistant Director (Environment) BPS-17Document23 pagesAssistant Director (Environment) BPS-17nomanNo ratings yet
- Catalogo de Pecas Carregadeira Pneus Volvo L120e PDFDocument1,172 pagesCatalogo de Pecas Carregadeira Pneus Volvo L120e PDFPedro Matheus90% (10)
- Guideline Title: Intra-Aortic Balloon Pump ManagementDocument16 pagesGuideline Title: Intra-Aortic Balloon Pump ManagementJansen ChNo ratings yet
- Perfusion SystemDocument30 pagesPerfusion SystemShailendra Singh Khichi100% (1)
- Liverpool SDL CRRTDocument62 pagesLiverpool SDL CRRTupul85No ratings yet
- Isbi Practice Guidelines For Burn Care Part 2 2018 PDFDocument90 pagesIsbi Practice Guidelines For Burn Care Part 2 2018 PDFAstri SuyataNo ratings yet
- Main Engine Manual s70mcDocument287 pagesMain Engine Manual s70mcarun100% (1)
- Drug Guideline Title: Remifentanil: SummaryDocument11 pagesDrug Guideline Title: Remifentanil: SummaryyafetNo ratings yet
- Management of The EVDDocument7 pagesManagement of The EVDplethoraldork100% (1)
- Ventricular Assist DeviceDocument12 pagesVentricular Assist DevicesamadonyNo ratings yet
- A Guide To ECG Reporting For Year 3 Medical StudentsDocument2 pagesA Guide To ECG Reporting For Year 3 Medical StudentscsngiuNo ratings yet
- Awareness Under AnesthesiaDocument27 pagesAwareness Under AnesthesiaagatakassaNo ratings yet
- Surgical Implications of Low Cardiac Output Syndrome After Myocardial InfarctionDocument5 pagesSurgical Implications of Low Cardiac Output Syndrome After Myocardial Infarctionrandomized1234No ratings yet
- Anaesthetic Management of Joint Replacement SurgeriesDocument55 pagesAnaesthetic Management of Joint Replacement SurgeriesRaguNo ratings yet
- Regional AnesthesiaDocument54 pagesRegional AnesthesiaIdza Fariha AfriNo ratings yet
- Journal ClubDocument26 pagesJournal Clubysindhura23gmailcom100% (1)
- Difficult Weaning From Cardiopulmonary Bypass Final Edit LiaDocument41 pagesDifficult Weaning From Cardiopulmonary Bypass Final Edit LiaYuri SadewoNo ratings yet
- Intravenous Regonal Anaesthesia Biers BlockDocument2 pagesIntravenous Regonal Anaesthesia Biers BlockOkenabirhieNo ratings yet
- Appendix 10 - Warfarin Counselling ChecklistDocument3 pagesAppendix 10 - Warfarin Counselling ChecklistMuhammad TahirNo ratings yet
- Bier Block (Intravenous Regional Anesthesia), Handout PDFDocument8 pagesBier Block (Intravenous Regional Anesthesia), Handout PDFjahangirealamNo ratings yet
- Management of Acute PainDocument76 pagesManagement of Acute PainAnonymous nruHyuwtJ100% (1)
- A Comparative Study of Phenylephrine, Ephedrine and Mephentermine For Maintainance of Arterial Pressure During Spinal Anaesthesia in Caesarean SectionDocument6 pagesA Comparative Study of Phenylephrine, Ephedrine and Mephentermine For Maintainance of Arterial Pressure During Spinal Anaesthesia in Caesarean SectionInternational Organization of Scientific Research (IOSR)No ratings yet
- MayoclinprocDocument12 pagesMayoclinprocpriyaNo ratings yet
- Assessment of Postoperative Fever BMJDocument40 pagesAssessment of Postoperative Fever BMJMario Guzmán GutiérrezNo ratings yet
- Anesthesia For Cardiac Surgery - General Principles - UpToDateDocument58 pagesAnesthesia For Cardiac Surgery - General Principles - UpToDateEvoluciones MedicinaNo ratings yet
- Anesthetic Consideration in Hypertensive PatientDocument11 pagesAnesthetic Consideration in Hypertensive PatientYosiAsmaraNo ratings yet
- DIVITI Slide Prophylaxis VTE SPPD Ringkas-1Document11 pagesDIVITI Slide Prophylaxis VTE SPPD Ringkas-1Fera NurrizaNo ratings yet
- Adult Bradycardia Algorithm: Identify and Treat Underlying CauseDocument1 pageAdult Bradycardia Algorithm: Identify and Treat Underlying CausenebrasNo ratings yet
- Guideline Title: Cardiac Monitoring in ICUDocument14 pagesGuideline Title: Cardiac Monitoring in ICURirin RozalinaNo ratings yet
- Electrolyte Replacement Guide - ICU CliniciansDocument8 pagesElectrolyte Replacement Guide - ICU Cliniciansnolan4266No ratings yet
- Best Practice in ShockDocument30 pagesBest Practice in ShockFoungZanz D. LuffyzNo ratings yet
- Effect of Magnesium Sulphate On Intraoperative Hemodynamic Responses in Laparoscopic CholecystectomyDocument10 pagesEffect of Magnesium Sulphate On Intraoperative Hemodynamic Responses in Laparoscopic CholecystectomyIOSRjournalNo ratings yet
- Neurologic Assessment RationaleDocument16 pagesNeurologic Assessment RationaleflorenzoNo ratings yet
- Anesthesia For Tracheoesophageal Fistula RepairDocument29 pagesAnesthesia For Tracheoesophageal Fistula RepairArop AkechNo ratings yet
- 1095 Preoperative Risk Stratification and OptimizationDocument99 pages1095 Preoperative Risk Stratification and OptimizationHening Tirta KusumawardaniNo ratings yet
- Point of View Heparin ResistanceDocument20 pagesPoint of View Heparin ResistanceSameer Goyal100% (1)
- Myocardial ProtectionDocument36 pagesMyocardial ProtectionRheecha JoshiNo ratings yet
- TachycardiaDocument12 pagesTachycardiaPuskesmas Pinang JayaNo ratings yet
- MonitoringDocument128 pagesMonitoringShahzada irfanNo ratings yet
- Peripheral Nerve Stimulation Train of Four Monitoring Resource Manual Rev Jan 2020.2Document17 pagesPeripheral Nerve Stimulation Train of Four Monitoring Resource Manual Rev Jan 2020.2pankaj88gmcNo ratings yet
- Massive TransfusionDocument104 pagesMassive Transfusionbingkydoodle1012No ratings yet
- Enhanced Recovery AfterDocument14 pagesEnhanced Recovery Afterpiceng ismailNo ratings yet
- Traumatic Brain InjuryDocument40 pagesTraumatic Brain InjuryRed DevilNo ratings yet
- Anesthesia Considerations in Microlaryngoscopy or Direct LaryngosDocument6 pagesAnesthesia Considerations in Microlaryngoscopy or Direct LaryngosRubén Darío HerediaNo ratings yet
- Levosimendan in Patients With Low Cardiac Output SyndromeDocument7 pagesLevosimendan in Patients With Low Cardiac Output SyndromeNehemias MD GuevaraNo ratings yet
- Pitfalls in Anesthesia MonitoringDocument56 pagesPitfalls in Anesthesia MonitoringDr.Sandeep Kumar Kar100% (1)
- Anesthesia For Patients With Thyroid Disease - UpToDateDocument12 pagesAnesthesia For Patients With Thyroid Disease - UpToDateJavier GlezqNo ratings yet
- Acls Course HandoutsDocument8 pagesAcls Course HandoutsRoxas CedrickNo ratings yet
- Symptoms Respiratory System Cardiovascular System DiagnosisDocument2 pagesSymptoms Respiratory System Cardiovascular System DiagnosisAdelina RinataNo ratings yet
- Rosenberg Circulatory Assist DevicesDocument61 pagesRosenberg Circulatory Assist DevicesMilisha Albro100% (1)
- Mechanical ThrombectomyDocument58 pagesMechanical Thrombectomyres.uditacharyaNo ratings yet
- Scape Vs FospeDocument5 pagesScape Vs FospeDr. FarhanNo ratings yet
- Standard Treatment Protocol of Emergency Health Service PackageDocument279 pagesStandard Treatment Protocol of Emergency Health Service Packagekapil khanalNo ratings yet
- West Visayas State University: Nursing ProcessDocument4 pagesWest Visayas State University: Nursing ProcessPhylum Chordata100% (1)
- FINAL CA-1 Tutorial Textbook 2017Document74 pagesFINAL CA-1 Tutorial Textbook 2017Farjad IkramNo ratings yet
- Adrenaline (Anaethesia Tutorial of The Week)Document8 pagesAdrenaline (Anaethesia Tutorial of The Week)Raisa AriesthaNo ratings yet
- Principles of Antibiotics: Deepa V Post Graduate Student DSCDS, BangaloreDocument117 pagesPrinciples of Antibiotics: Deepa V Post Graduate Student DSCDS, BangaloreDeepa VenkateshNo ratings yet
- Defibrillatorppt 131028115457 Phpapp01Document41 pagesDefibrillatorppt 131028115457 Phpapp01Simon JosanNo ratings yet
- Anesthesia For The Patient With Preeclampsia - UpToDateDocument31 pagesAnesthesia For The Patient With Preeclampsia - UpToDateJazivi AlejoNo ratings yet
- Bronchiectasis: Dr.K.M.LakshmanarajanDocument238 pagesBronchiectasis: Dr.K.M.LakshmanarajanKM Lakshmana Rajan0% (1)
- DC Power Supply With 220V AC Input and 3V, 5V, 9V and 12V DC OutputDocument13 pagesDC Power Supply With 220V AC Input and 3V, 5V, 9V and 12V DC Output2XWinNo ratings yet
- Fun Projects 02 ChapterDocument3 pagesFun Projects 02 ChaptertihomihoNo ratings yet
- Ursa Anqtillea Teddy Bear - GirlDocument16 pagesUrsa Anqtillea Teddy Bear - Girlkarol bueno100% (2)
- The Method of The Siddhas 5 Walking The Dog PDF FreeDocument25 pagesThe Method of The Siddhas 5 Walking The Dog PDF FreeDesiré Angelica GANo ratings yet
- Snorkel TB126J PDFDocument234 pagesSnorkel TB126J PDFAnar QasimovNo ratings yet
- Sample Business Plan 1 2021 2022Document23 pagesSample Business Plan 1 2021 2022Claudio MatarazzoNo ratings yet
- Fluid Mechanics White 7th SOL Part1 Part1Document5 pagesFluid Mechanics White 7th SOL Part1 Part1Jose EscobarNo ratings yet
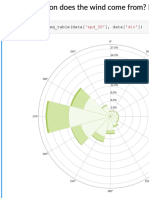
- Predicting The Wind: Data Science in Wind Resource AssessmentDocument61 pagesPredicting The Wind: Data Science in Wind Resource AssessmentFlorian RoscheckNo ratings yet
- Third Semester Form Submitted SuccessfullyDocument1 pageThird Semester Form Submitted SuccessfullyMohit KumarNo ratings yet
- Egypt Exam 2021 (Second Session) QuestionsDocument27 pagesEgypt Exam 2021 (Second Session) QuestionsMaroska YoussefNo ratings yet
- Organic DPPDocument11 pagesOrganic DPPRahul KumarNo ratings yet
- Grade VII ScienceDocument20 pagesGrade VII ScienceSunny BbaNo ratings yet
- Efficiency, Economy Polymer Metering SystemDocument12 pagesEfficiency, Economy Polymer Metering Systemjuanper01No ratings yet
- Week 5 - Design Automation - Lecture PresentationDocument39 pagesWeek 5 - Design Automation - Lecture PresentationsrinivaskayalaNo ratings yet
- GEN-CHEM-1 G11 Module3 Q1W3 MODDocument15 pagesGEN-CHEM-1 G11 Module3 Q1W3 MODDaniel Corcino100% (1)
- LogDocument2 pagesLogAlexander HackerNo ratings yet
- 2321-Article Text-10181-1-10-20110622Document23 pages2321-Article Text-10181-1-10-20110622steve rubioNo ratings yet
- Polaroid FLM1911Document30 pagesPolaroid FLM1911videosonNo ratings yet
- Data Dependences: CS 524 - High-Performance ComputingDocument20 pagesData Dependences: CS 524 - High-Performance Computingmarifs2002No ratings yet
- Waiting For GodotDocument2 pagesWaiting For GodotIoana OlteanuNo ratings yet
- 6-Transport System in Ancient IndiaDocument69 pages6-Transport System in Ancient IndiaAshok Nene100% (1)
- Seminar Presentation 7Document60 pagesSeminar Presentation 7emma_ade92007No ratings yet
- Earth Moving Machines-A GlanceDocument27 pagesEarth Moving Machines-A GlanceVinod YbNo ratings yet
- SPEC 3 ColteneDocument2 pagesSPEC 3 ColteneVaneza ZambranoNo ratings yet
- Chocolate AnalysisDocument15 pagesChocolate AnalysissbdcmailNo ratings yet
- Kisi Kisi Utama USBN Bahasa Dan Sastra Inggris Peminatan Lintas Minat K 2013 2019 Valid Docx 2Document20 pagesKisi Kisi Utama USBN Bahasa Dan Sastra Inggris Peminatan Lintas Minat K 2013 2019 Valid Docx 2Man KotamobaguNo ratings yet
- CFSEI Tech Note X Bracing L001-09Document8 pagesCFSEI Tech Note X Bracing L001-09Jane EyreNo ratings yet