You might also like
- Lower GI Chapter Summary: Constipation, Diarrhea, Appendicitis & MoreDocument8 pagesLower GI Chapter Summary: Constipation, Diarrhea, Appendicitis & MoreRebeccaNo ratings yet
- Gastrointestinal Anatomy and Physiology: The EssentialsFrom EverandGastrointestinal Anatomy and Physiology: The EssentialsJohn F. ReinusNo ratings yet
- NEURO2 1.02C Hemorrhagic Stroke - Dr. HiyadanDocument2 pagesNEURO2 1.02C Hemorrhagic Stroke - Dr. HiyadanAra Diocos100% (1)
- Surgery II - Pancreas 2014Document20 pagesSurgery II - Pancreas 2014Medisina101No ratings yet
- Problem-based Approach to Gastroenterology and HepatologyFrom EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisNo ratings yet
- Congenital Heart DefectsDocument45 pagesCongenital Heart Defectskathylaine100% (1)
- A System of Operative Surgery, Volume IV (of 4)From EverandA System of Operative Surgery, Volume IV (of 4)Rating: 4 out of 5 stars4/5 (1)
- Approach To The Adult With Unexplained Thrombocytopenia - UpToDateDocument65 pagesApproach To The Adult With Unexplained Thrombocytopenia - UpToDateMagdy GabrNo ratings yet
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Placement and Management of Thoracostomy Tubes - UpToDateDocument24 pagesPlacement and Management of Thoracostomy Tubes - UpToDateAndres Felipe Cuspoca OrduzNo ratings yet
- Postcholecystectomy SyndromeDocument27 pagesPostcholecystectomy SyndromeMonica TurnerNo ratings yet
- GI BLEED - Medicine - Internal MedicineDocument11 pagesGI BLEED - Medicine - Internal Medicinezezma GamingNo ratings yet
- Intra Abdominal 2009Document8 pagesIntra Abdominal 2009Shinta Dwi Septiani Putri WibowoNo ratings yet
- Surgery: by DR - Mohammad Z. Abu Sheikha@Document145 pagesSurgery: by DR - Mohammad Z. Abu Sheikha@صقر حورانNo ratings yet
- Common Surgical PresentationsDocument49 pagesCommon Surgical PresentationsJeremiah HiiNo ratings yet
- Differential Diagnosis Pain Right HypochondriumDocument35 pagesDifferential Diagnosis Pain Right HypochondriumDrArish Mahmood100% (1)
- Colon Anatomy and Appendicitis GuideDocument30 pagesColon Anatomy and Appendicitis GuideKiara GovenderNo ratings yet
- History Taking for Gallstones (CholelithiasisDocument6 pagesHistory Taking for Gallstones (CholelithiasisToria053No ratings yet
- Abdominal LumpDocument19 pagesAbdominal LumpDeepak AnNo ratings yet
- Acute Pain Abdomen in Surgical PracticeDocument34 pagesAcute Pain Abdomen in Surgical PracticedrakashnardeNo ratings yet
- Approach To Patient With GI BleedDocument22 pagesApproach To Patient With GI BleedZaidatul Atiqah Mustafa100% (1)
- Abdominal Wall IncisionDocument42 pagesAbdominal Wall IncisionURo KkuNo ratings yet
- 6 Imaging of Acute AbdomenDocument73 pages6 Imaging of Acute AbdomenAliyah Tofani PawelloiNo ratings yet
- DDX - Gastrointestinal Disorders ChartDocument21 pagesDDX - Gastrointestinal Disorders Chartapi-26938624100% (2)
- Diseases of Esophagus & Dysphagia: Dr. Vishal SharmaDocument146 pagesDiseases of Esophagus & Dysphagia: Dr. Vishal SharmaMohamed KamaraNo ratings yet
- Acute abdomen and bone fracture conditionsDocument50 pagesAcute abdomen and bone fracture conditionsSharaz AhmedNo ratings yet
- Git DisturbancesDocument119 pagesGit DisturbancesPeterpan NguyenNo ratings yet
- (HLMN 5-19) Evaluation of The Adult With Abdominal Pain - UpToDateDocument21 pages(HLMN 5-19) Evaluation of The Adult With Abdominal Pain - UpToDateandylumanNo ratings yet
- Management of Acute Appendicitis in Adults - UpToDateDocument28 pagesManagement of Acute Appendicitis in Adults - UpToDateaulia rachman100% (1)
- Radiofrequency AblationDocument6 pagesRadiofrequency Ablationraviks34No ratings yet
- Phyllodes Tumors of The Breast UpToDateDocument22 pagesPhyllodes Tumors of The Breast UpToDateSean SialanaNo ratings yet
- Jaundice: Seminar Under The Guidance Of-Dr. Shiva NarangDocument47 pagesJaundice: Seminar Under The Guidance Of-Dr. Shiva NarangMiguel MansillaNo ratings yet
- Baltarowich ABD pt1 Hepatobiliary US PDFDocument22 pagesBaltarowich ABD pt1 Hepatobiliary US PDFEka KusumaningatiNo ratings yet
- PR BleedDocument20 pagesPR BleedCathy KayNo ratings yet
- Surgical Management of ObesityDocument13 pagesSurgical Management of Obesityمحمد حميدانNo ratings yet
- Surgical Anatomy of The Chest Wall, Pleura, and MediastinumDocument8 pagesSurgical Anatomy of The Chest Wall, Pleura, and MediastinumNooneNo ratings yet
- PancreatitisDocument51 pagesPancreatitisMizrab NadeemNo ratings yet
- TransplantationDocument11 pagesTransplantationmardsz100% (1)
- Polycystic Kidney DiseaseDocument9 pagesPolycystic Kidney DiseaseCésar Aguilar ContrerasNo ratings yet
- Child With Bruises 00Document36 pagesChild With Bruises 00Awatef AbushhiwaNo ratings yet
- 17 - Gallbladder StonesDocument71 pages17 - Gallbladder StonesRashed ShatnawiNo ratings yet
- Case Sheet - Abdominal Lump in Right Lumbar RegionDocument5 pagesCase Sheet - Abdominal Lump in Right Lumbar RegionpradeepNo ratings yet
- Pathology of the Digestive SystemDocument28 pagesPathology of the Digestive SystemDianNursyifaRahmahNo ratings yet
- Conservative Management of Perforated Peptic UlcerDocument4 pagesConservative Management of Perforated Peptic UlcerAfiani JannahNo ratings yet
- Abdominal PainDocument26 pagesAbdominal Painsammy_d6No ratings yet
- Absite CH 32 BilliaryDocument14 pagesAbsite CH 32 BilliaryJames JosephNo ratings yet
- Acute Abdominal Pain: Associate Professor, Dept. of Surgery Mti, KMC, KTHDocument45 pagesAcute Abdominal Pain: Associate Professor, Dept. of Surgery Mti, KMC, KTHWaleed MaboodNo ratings yet
- Vascular Diseases (1 of 3)Document4 pagesVascular Diseases (1 of 3)Doctor GeneralNo ratings yet
- Acute Abdomen: - DefinitionDocument27 pagesAcute Abdomen: - DefinitionWorku KifleNo ratings yet
- Approach To The Adult Patient With Anemia - UpToDateDocument23 pagesApproach To The Adult Patient With Anemia - UpToDateNicole SierraNo ratings yet
- History and Physical Examination TemplateDocument3 pagesHistory and Physical Examination TemplateRawa MuhsinNo ratings yet
- Kidney AnatomyDocument2 pagesKidney Anatomyameerabest100% (1)
- 10 EdemaDocument23 pages10 EdemaTalmaciu AmyNo ratings yet
- Pathophysiology: Rectal CarcinomaDocument25 pagesPathophysiology: Rectal CarcinomaCristina CristinaNo ratings yet
- Upper GIT BleedingDocument69 pagesUpper GIT BleedingSoleh Ramly100% (1)
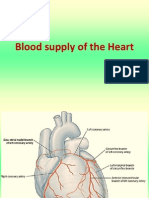
- Blood Supply of HeartDocument7 pagesBlood Supply of Heartmariposa_0612No ratings yet
- Endovascular Surgery - BenkőDocument33 pagesEndovascular Surgery - BenkőpampaszNo ratings yet
- Definition, Classification, Etiology, and Pathophysiology of Shock in Adults - UpToDateDocument16 pagesDefinition, Classification, Etiology, and Pathophysiology of Shock in Adults - UpToDatevara prasadNo ratings yet
- Colorectal CancerDocument1 pageColorectal CancerMary GiuntiniNo ratings yet
- Exemplar - Inflammatory Bowel DiseaseDocument1 pageExemplar - Inflammatory Bowel DiseaseMary GiuntiniNo ratings yet
- Hyper GlycemiaDocument1 pageHyper GlycemiaMary GiuntiniNo ratings yet
- Exemplar - Protein-Calorie MalnutritionDocument1 pageExemplar - Protein-Calorie MalnutritionMary GiuntiniNo ratings yet
- Exemplar - Hypoglycemia: If Blood Glucose Levels Continue To Drop.Document1 pageExemplar - Hypoglycemia: If Blood Glucose Levels Continue To Drop.Mary GiuntiniNo ratings yet
- DiverticulitisDocument1 pageDiverticulitisMary GiuntiniNo ratings yet
- Peptic Ulcer DiseaseDocument1 pagePeptic Ulcer DiseaseMary GiuntiniNo ratings yet
- Concept Map StrokeDocument1 pageConcept Map StrokeMary GiuntiniNo ratings yet
- Exemplar - Obesity/BMI: Energy ExpenditureDocument1 pageExemplar - Obesity/BMI: Energy ExpenditureMary GiuntiniNo ratings yet
- Concept Map PDDocument1 pageConcept Map PDMary GiuntiniNo ratings yet
- AppendicitisDocument1 pageAppendicitisMary GiuntiniNo ratings yet
- Concept Map SeizuresDocument1 pageConcept Map SeizuresMary GiuntiniNo ratings yet
- Obessive Compulsive Disorder (OCD)Document10 pagesObessive Compulsive Disorder (OCD)marketingmoneyindiaNo ratings yet
- Registration Form Proficiency Testing Program: Name Designation Mob. / Tel. NoDocument4 pagesRegistration Form Proficiency Testing Program: Name Designation Mob. / Tel. NoOwais Manzoor MalikNo ratings yet
- 1868 Sop Work at HeightDocument10 pages1868 Sop Work at HeightAbid AzizNo ratings yet
- Test Bank For American Pageant Volume 1 16th EditionDocument36 pagesTest Bank For American Pageant Volume 1 16th Editionzoonwinkfoxyj8100% (48)
- Maintenance Manual: Ul-Aircraft Ltf-Ul 2003 Manufacturer No.: FRXXX Registration No: D-MXXXDocument27 pagesMaintenance Manual: Ul-Aircraft Ltf-Ul 2003 Manufacturer No.: FRXXX Registration No: D-MXXXAlbaz DarwishNo ratings yet
- Integrate Payments Direct Post APIDocument31 pagesIntegrate Payments Direct Post APIAnjali SharmaNo ratings yet
- 1967 Painting Israeli VallejoDocument1 page1967 Painting Israeli VallejoMiloš CiniburkNo ratings yet
- Types of Motivation in Language LearningDocument8 pagesTypes of Motivation in Language LearningAlya IrmasyahNo ratings yet
- Communication Strategy Target AudienceDocument47 pagesCommunication Strategy Target Audienceguille simariNo ratings yet
- SALICYLATE POISONING SIGNS AND TREATMENTDocument23 pagesSALICYLATE POISONING SIGNS AND TREATMENTimmortalneoNo ratings yet
- National Geographic USA - 01 2019Document145 pagesNational Geographic USA - 01 2019Minh ThuNo ratings yet
- NEW HOLLAND - Trucks, Tractor & Forklift Manual PDDocument14 pagesNEW HOLLAND - Trucks, Tractor & Forklift Manual PDAjjaakka0% (2)
- Reliability and CredibilityDocument1 pageReliability and CredibilitycedrictuasonNo ratings yet
- Contrastive Study of English and Romanian Legal TerminologyDocument39 pagesContrastive Study of English and Romanian Legal TerminologyVictorNo ratings yet
- Weekly Capital Market Report Week Ending 22.07.2022 2022-07-22Document2 pagesWeekly Capital Market Report Week Ending 22.07.2022 2022-07-22Fuaad DodooNo ratings yet
- Emotion-WPS OfficeDocument2 pagesEmotion-WPS OfficemikaNo ratings yet
- List of Registered Non Govt and Govt Secondary SchoolDocument200 pagesList of Registered Non Govt and Govt Secondary SchoolDennisEudes78% (9)
- Forms of WillsDocument24 pagesForms of WillsJasNo ratings yet
- Document Application and Review FormDocument1 pageDocument Application and Review FormJonnel CatadmanNo ratings yet
- School RulesDocument2 pagesSchool RulesAI HUEYNo ratings yet
- GES1003 AY1819 CLS Tutorial 1Document4 pagesGES1003 AY1819 CLS Tutorial 1AshwinNo ratings yet
- Sponsor A Child With E-Tuition 2022Document19 pagesSponsor A Child With E-Tuition 2022nuur xiemaNo ratings yet
- Criteria For Judging MR and Ms UNDocument9 pagesCriteria For Judging MR and Ms UNRexon ChanNo ratings yet
- Surio vs. ReyesDocument3 pagesSurio vs. ReyesAdrian FranzingisNo ratings yet
- Hacking Web ApplicationsDocument5 pagesHacking Web ApplicationsDeandryn RussellNo ratings yet
- Use VCDS with PC lacking InternetDocument1 pageUse VCDS with PC lacking Internetvali_nedeleaNo ratings yet
- EasyGreen ManualDocument33 pagesEasyGreen ManualpitoupitouNo ratings yet
- Skills Test Unit 1 Test A EmailDocument4 pagesSkills Test Unit 1 Test A EmailЛиза ОмельченкоNo ratings yet
- Joyce2016 PDFDocument13 pagesJoyce2016 PDFAffan ArrizqiNo ratings yet
- Reported SpeechDocument2 pagesReported SpeechlacasabaNo ratings yet