You might also like
- Cs5 Midterm PPT Maya KawwaDocument12 pagesCs5 Midterm PPT Maya KawwaMaya KawwaNo ratings yet
- Sindrom Chediak HigashiDocument8 pagesSindrom Chediak HigashiDiana AstriaNo ratings yet
- Ple 2015 Board Review May 2015 Patho OnlyDocument10 pagesPle 2015 Board Review May 2015 Patho OnlyMa Katherina ArellanoNo ratings yet
- Vogt Koyanagi Harada SyndromeDocument3 pagesVogt Koyanagi Harada SyndromeHarry DhaliwalNo ratings yet
- Medscape Reference ReferenceDocument35 pagesMedscape Reference Referencevinorry_vheetaNo ratings yet
- Kuliahskin Pigmentation + Hair Disorder-Power Pointedit-2 - 26april11Document113 pagesKuliahskin Pigmentation + Hair Disorder-Power Pointedit-2 - 26april11Andersen ChenNo ratings yet
- Di George SyndromeDocument14 pagesDi George SyndromeStetho LoveNo ratings yet
- Disorders of BloodDocument3 pagesDisorders of BloodCondurache Ilie-AndreiNo ratings yet
- Genodermatosis: The IchthyosisDocument4 pagesGenodermatosis: The IchthyosisOman ArifNo ratings yet
- LeptospirosisDocument7 pagesLeptospirosisFarah Nadia MoksinNo ratings yet
- Approach To A Child With Pallor and Hepatosplenomegaly: Anirban DasDocument8 pagesApproach To A Child With Pallor and Hepatosplenomegaly: Anirban DasvgmanjunathNo ratings yet
- Incidence: Specific Types of UveitisDocument15 pagesIncidence: Specific Types of UveitisImatunnisaZiNo ratings yet
- Objective PEDSDocument58 pagesObjective PEDSlaraNo ratings yet
- Background: Staphylococcal Scalded Skin SyndromeDocument6 pagesBackground: Staphylococcal Scalded Skin Syndromeطاهرة حربية AlcaldeNo ratings yet
- Out 7Document8 pagesOut 7Musthafa Afif WardhanaNo ratings yet
- Review: Ocular Toxoplasmosis II: Clinical Features, Pathology and ManagementDocument14 pagesReview: Ocular Toxoplasmosis II: Clinical Features, Pathology and Managementhidrisdmnk_747467972No ratings yet
- ANA TestDocument9 pagesANA TestNena_mileyNo ratings yet
- Frosted Branch AngiitisDocument9 pagesFrosted Branch AngiitisDragos-Constantin LuncaNo ratings yet
- Diseases of SkinDocument12 pagesDiseases of SkinpayalpachiNo ratings yet
- Whitedotsyndromes EditedDocument37 pagesWhitedotsyndromes EditedSadyaja SmitaNo ratings yet
- Hereditary Elliptocytosis: A Seminar Report OnDocument11 pagesHereditary Elliptocytosis: A Seminar Report OnSantosh SangleNo ratings yet
- Scleroderma PDFDocument9 pagesScleroderma PDFAustine OsaweNo ratings yet
- Lecture 2 MLTDocument24 pagesLecture 2 MLTAbood dot netNo ratings yet
- Diseases of Salivary Glands 1Document30 pagesDiseases of Salivary Glands 1MahasnehEhab100% (1)
- Approach To A Child With Pallor and Hepatosplenomegaly: Anirban Das, MD, DMDocument7 pagesApproach To A Child With Pallor and Hepatosplenomegaly: Anirban Das, MD, DMMarc Lyndon CafinoNo ratings yet
- Systemic Lupus Erythematosus in Children and AdolescentsDocument2 pagesSystemic Lupus Erythematosus in Children and Adolescentsarlette aviñaNo ratings yet
- Skin PigmentatDocument110 pagesSkin Pigmentatsteven saputra0% (1)
- 1семестр Екзамен на місу іноз нове PDFDocument9 pages1семестр Екзамен на місу іноз нове PDFHart ElettNo ratings yet
- Ocular Manifestations of SLEDocument9 pagesOcular Manifestations of SLEChiquitaPutriVaniaRauNo ratings yet
- Deletion Syndromes: By: Rania ZahoDocument55 pagesDeletion Syndromes: By: Rania ZahoRania ZahoNo ratings yet
- Hemolytic Uremic Syndrome: Ankit GurjarDocument18 pagesHemolytic Uremic Syndrome: Ankit GurjarAnkit Tonger AnkyNo ratings yet
- LymphadenopathyDocument12 pagesLymphadenopathyErikha Chairil100% (1)
- SleDocument66 pagesSlebhushan vichareNo ratings yet
- Emergencias Hematologicas y OncologicasDocument17 pagesEmergencias Hematologicas y OncologicasFelipe Villarroel RomeroNo ratings yet
- Hiv & PsychiatryDocument25 pagesHiv & PsychiatryAbdulahi SaedNo ratings yet
- Hemolytic-Uremic Syndrome in ChildrenDocument17 pagesHemolytic-Uremic Syndrome in ChildrenYuri vanessa Ortiz hNo ratings yet
- Sle NewestDocument70 pagesSle NewestTuhinaRajNo ratings yet
- K-5 Pathophysiology of Cyanotic Congenital Heart DefectsDocument15 pagesK-5 Pathophysiology of Cyanotic Congenital Heart DefectsJessica GintingNo ratings yet
- Lipid Storage DiseaseDocument1 pageLipid Storage DiseaseRalphus KarlaNo ratings yet
- Genetic Disorders of PigmentationDocument58 pagesGenetic Disorders of Pigmentationkahkashanahmed065No ratings yet
- Cat Scratch DiseaseDocument4 pagesCat Scratch DiseasefabsscribdworksNo ratings yet
- Vesicubullous Diseases & Mucocutaneous DisordersDocument23 pagesVesicubullous Diseases & Mucocutaneous Disordersshahlaraib001No ratings yet
- Platelet Disorder Week 2Document3 pagesPlatelet Disorder Week 2KelvssNo ratings yet
- PediatricsDocument38 pagesPediatricskhanNo ratings yet
- Chronic Leukemia: Carlos Alfredo Cedeño RodríguezDocument24 pagesChronic Leukemia: Carlos Alfredo Cedeño RodríguezCarlos CedeñoNo ratings yet
- Technical Writing: Example Definition Sickle Cell AnemiaDocument4 pagesTechnical Writing: Example Definition Sickle Cell AnemiaNikko SterlingNo ratings yet
- Fatty Acids Synthesis L3: Lipid Storage DiseaseDocument6 pagesFatty Acids Synthesis L3: Lipid Storage DiseaseJerome EkohNo ratings yet
- AVIAN - Diseases of The Avian SpleenDocument7 pagesAVIAN - Diseases of The Avian Spleentaner_soysuren100% (1)
- Systemic Lupus ErythematosusDocument4 pagesSystemic Lupus ErythematosusFokeerbux ZyadNo ratings yet
- Sickle CellDocument16 pagesSickle CellAnastasiafynnNo ratings yet
- CIDPDocument21 pagesCIDPidno1008No ratings yet
- In Neonates, A Transient 6th Nerve Paresis Can Occur It Usually ClearsDocument22 pagesIn Neonates, A Transient 6th Nerve Paresis Can Occur It Usually ClearsFull MarksNo ratings yet
- Infantile Spasms: Review of The Literature and Personal ExperienceDocument10 pagesInfantile Spasms: Review of The Literature and Personal ExperienceDianMuliasariNo ratings yet
- Subacute and Chronic MeningitisDocument8 pagesSubacute and Chronic MeningitisLucky PuspitasariNo ratings yet
- Parasitology International: ReviewDocument7 pagesParasitology International: ReviewAhmad PradhanaNo ratings yet
- Photo QuizDocument21 pagesPhoto Quizabas_maytham1021100% (3)
- 2Farticle2F210752 PrintDocument12 pages2Farticle2F210752 PrintAnas ObiedNo ratings yet
- Hereditary SpherocytosisDocument23 pagesHereditary SpherocytosisKashan SiddiquiNo ratings yet
- Systemic Lupus Erythematosus (SLE)Document5 pagesSystemic Lupus Erythematosus (SLE)Daniel MazariegoNo ratings yet
- Nonprotein Nitrogenous SubstancesDocument1 pageNonprotein Nitrogenous SubstancesReynan Pornel RolleNo ratings yet
- Argument Number 1!Document3 pagesArgument Number 1!Reynan Pornel RolleNo ratings yet
- Immune System 2Document39 pagesImmune System 2AnaNo ratings yet
- BloodDocument28 pagesBloodapi-3802092No ratings yet
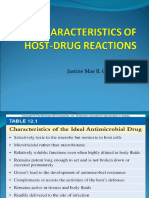
- Justine Mae R. Gonzales, RMTDocument24 pagesJustine Mae R. Gonzales, RMTReynan Pornel RolleNo ratings yet
- Chemical Agents FayDocument11 pagesChemical Agents FayReynan Pornel Rolle100% (1)
- Request For Proposals/quotationsDocument24 pagesRequest For Proposals/quotationsKarl Anthony Rigoroso MargateNo ratings yet
- High Speed Power TransferDocument33 pagesHigh Speed Power TransferJAYKUMAR SINGHNo ratings yet
- Nascsa - Sponsor Solicitation List: January 06, 2021Document35 pagesNascsa - Sponsor Solicitation List: January 06, 2021Prasoon SimsonNo ratings yet
- RS2 Stress Analysis Verification Manual - Part 1Document166 pagesRS2 Stress Analysis Verification Manual - Part 1Jordana Furman100% (1)
- Installation of Submarine PE PipesDocument84 pagesInstallation of Submarine PE Pipeswaseemiqbal133100% (2)
- Presentation LI: Prepared by Muhammad Zaim Ihtisham Bin Mohd Jamal A17KA5273 13 September 2022Document9 pagesPresentation LI: Prepared by Muhammad Zaim Ihtisham Bin Mohd Jamal A17KA5273 13 September 2022dakmts07No ratings yet
- DatuinMA (Activity #5 - NSTP 10)Document2 pagesDatuinMA (Activity #5 - NSTP 10)Marc Alen Porlaje DatuinNo ratings yet
- (Ebook - Antroposofia - EnG) - Rudolf Steiner - Fundamentals of TheraphyDocument58 pages(Ebook - Antroposofia - EnG) - Rudolf Steiner - Fundamentals of Theraphyblueyes247No ratings yet
- A Detailed Lesson PlanDocument5 pagesA Detailed Lesson PlanIsaac-elmar Agtarap74% (23)
- Democracy or Aristocracy?: Yasir MasoodDocument4 pagesDemocracy or Aristocracy?: Yasir MasoodAjmal KhanNo ratings yet
- Charter of The New UrbanismDocument4 pagesCharter of The New UrbanismBarabas SandraNo ratings yet
- Mossbauer SpectrosDocument7 pagesMossbauer SpectroscyrimathewNo ratings yet
- Cummins: ISX15 CM2250Document17 pagesCummins: ISX15 CM2250haroun100% (4)
- Operation and Maintenance Manual Compressor Models: P105WJD, P130DWJD, P160DWJD, P175DWJDDocument70 pagesOperation and Maintenance Manual Compressor Models: P105WJD, P130DWJD, P160DWJD, P175DWJDManuel ParreñoNo ratings yet
- Unit-5 Harmonics & FiltersDocument25 pagesUnit-5 Harmonics & FiltersBhanu100% (1)
- NauseaDocument12 pagesNauseakazakom100% (2)
- 1id Abstracts Season 2 Episode 6Document406 pages1id Abstracts Season 2 Episode 6Jennifer BrownNo ratings yet
- Writing About Graphs, Tables and DiagramsDocument68 pagesWriting About Graphs, Tables and DiagramsLangers BastasaNo ratings yet
- Chromatographic Separation PDFDocument7 pagesChromatographic Separation PDFNicolle CletoNo ratings yet
- 8 Adam AmuraroDocument28 pages8 Adam Amurarokmeena73No ratings yet
- V13 D03 1 PDFDocument45 pagesV13 D03 1 PDFFredy Camayo De La CruzNo ratings yet
- PID Marcado Operación Del Paquete Del Compresor de Hidrogeno PHP-K-002 PDFDocument7 pagesPID Marcado Operación Del Paquete Del Compresor de Hidrogeno PHP-K-002 PDFDenisNo ratings yet
- VERGARA - RPH Reflection PaperDocument2 pagesVERGARA - RPH Reflection PaperNezer Byl P. VergaraNo ratings yet
- Zillah P. Curato: ObjectiveDocument1 pageZillah P. Curato: ObjectiveZillah CuratoNo ratings yet
- A Structural Modelo of Limital Experienci Un TourismDocument15 pagesA Structural Modelo of Limital Experienci Un TourismcecorredorNo ratings yet
- Week 1 Familiarize The VmgoDocument10 pagesWeek 1 Familiarize The VmgoHizzel De CastroNo ratings yet
- CLT Apllications NewestDocument49 pagesCLT Apllications NewestMackBrideNo ratings yet
- Present Perfect and Present Perfect ProgressiveDocument5 pagesPresent Perfect and Present Perfect ProgressiveKiara Fajardo matusNo ratings yet
- Oracle SOA Suite Oracle Containers For J2EE Feature Overview OC4JDocument10 pagesOracle SOA Suite Oracle Containers For J2EE Feature Overview OC4JLuis YañezNo ratings yet
- Earth Science NAME - DATEDocument3 pagesEarth Science NAME - DATEArlene CalataNo ratings yet