You might also like
- Cardio DrugsDocument68 pagesCardio DrugsIconMaicoNo ratings yet
- Antihypertensive Drugs RTDocument41 pagesAntihypertensive Drugs RTMaherNo ratings yet
- Antiplatelets: Prabina - P K 2 ND MSC Nursing Govt. College of Nursing KozhikodeDocument53 pagesAntiplatelets: Prabina - P K 2 ND MSC Nursing Govt. College of Nursing Kozhikodeanju rachel joseNo ratings yet
- Farmakologi 1 Antihypertension: NURUL HASANAH (1800085)Document31 pagesFarmakologi 1 Antihypertension: NURUL HASANAH (1800085)MutiaraBintangNo ratings yet
- Cardiac DrugsDocument35 pagesCardiac DrugsCristina Centurion100% (3)
- Pharmacology of Cardiac Diseases MINEDocument3 pagesPharmacology of Cardiac Diseases MINEMitu Miressa تNo ratings yet
- Applying Pharmacology Concepts to Beta Blocker TherapyDocument269 pagesApplying Pharmacology Concepts to Beta Blocker TherapyTrishaNo ratings yet
- Drugs of CvsDocument32 pagesDrugs of CvsAgus HaryantoNo ratings yet
- عرض تقديمي2Document18 pagesعرض تقديمي2Sabrina ShalhoutNo ratings yet
- Drugs Acting On Cardiovascular SystemDocument81 pagesDrugs Acting On Cardiovascular SystemevaNo ratings yet
- Farmakoterapi StrokeDocument33 pagesFarmakoterapi StrokeMuhammad Aldi SetiawanNo ratings yet
- Heart Disease Drugs: Cardiac Glycosides, Antihypertensives & DiureticsDocument24 pagesHeart Disease Drugs: Cardiac Glycosides, Antihypertensives & Diureticsblah4020No ratings yet
- Complications DM FinalDocument57 pagesComplications DM FinalBarbie GirlNo ratings yet
- Heart Attack Medications and Nursing ConsiderationsDocument35 pagesHeart Attack Medications and Nursing ConsiderationsFev BanataoNo ratings yet
- PENGGUNAAN OBAT PADA SISTEM CARDIOVASCULARDocument56 pagesPENGGUNAAN OBAT PADA SISTEM CARDIOVASCULARwidya vannesaNo ratings yet
- On Emergency DrugsDocument25 pagesOn Emergency DrugsBikram Chhetry100% (1)
- ACLS DrugsDocument16 pagesACLS Drugstostc100% (2)
- Hypertension Lecture3: Pharmacological TreatmentDocument25 pagesHypertension Lecture3: Pharmacological TreatmentRam NiwasNo ratings yet
- Drugs in Cardiac EnmergenciesDocument94 pagesDrugs in Cardiac EnmergenciesVijayan VelayudhanNo ratings yet
- PharmaDocument8 pagesPharma2022105340No ratings yet
- Hypertension: Silent KillerDocument28 pagesHypertension: Silent KilleribratiNo ratings yet
- Drugs Used in CcuDocument169 pagesDrugs Used in CcuAnusha Verghese100% (3)
- EE Tarek Exam Hints 2019-1Document83 pagesEE Tarek Exam Hints 2019-1Ibrahim Sayed AhmedNo ratings yet
- Y7PH0566, Yedla Pradeep Kumar, 4 B.Pharmacy, Cips, Lam, GunturDocument33 pagesY7PH0566, Yedla Pradeep Kumar, 4 B.Pharmacy, Cips, Lam, Gunturప్రదీప్ కుమార్100% (4)
- HTN JmiDocument39 pagesHTN Jmink999999No ratings yet
- Study Guide For Final Pharmacology HypertensionDocument39 pagesStudy Guide For Final Pharmacology HypertensionAlejandro Daniel Landa MoralesNo ratings yet
- LisinoprilDocument3 pagesLisinoprilapi-37979410% (1)
- DRUGS PediatricsDocument42 pagesDRUGS PediatricsRAJ BADMERANo ratings yet
- Understanding Hypertension: Causes, Symptoms, Diagnosis and TreatmentDocument37 pagesUnderstanding Hypertension: Causes, Symptoms, Diagnosis and TreatmentrasheedNo ratings yet
- Cardiac Glycosides and Phosphodiesterase InhibitorsDocument30 pagesCardiac Glycosides and Phosphodiesterase Inhibitorskenneth santosNo ratings yet
- Drugs Study Neh Jai2xDocument10 pagesDrugs Study Neh Jai2xjai2xNo ratings yet
- HypertensiveDocument2 pagesHypertensiveReinhard Lumbag PacitengNo ratings yet
- Congestive Heart Failure: Dr. J. SaravananDocument31 pagesCongestive Heart Failure: Dr. J. Saravananpetervazhayil100% (1)
- Captopril Pharmacological Properties and UsesDocument13 pagesCaptopril Pharmacological Properties and UsesputrinadNo ratings yet
- 6.Z8sNyP 6 GHafez HT and Antihypertensive DrugsDocument81 pages6.Z8sNyP 6 GHafez HT and Antihypertensive Drugsyasmin.rahmany03No ratings yet
- CVS Prescription-1 2023Document25 pagesCVS Prescription-1 2023Stock CheckNo ratings yet
- Anti-Anginal DrugsDocument39 pagesAnti-Anginal Drugspoonam rana100% (1)
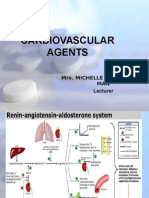
- Cardiovascular Agents: Mrs. Michelle A. Iduria, RN, MAN LecturerDocument131 pagesCardiovascular Agents: Mrs. Michelle A. Iduria, RN, MAN LecturerNiala AlmarioNo ratings yet
- Pharmacological-Management-of-HypertensionDocument35 pagesPharmacological-Management-of-Hypertensiontf.almutairi88No ratings yet
- Pad HPNDocument137 pagesPad HPNpmm21d229No ratings yet
- CarvedilolDocument3 pagesCarvedilolapi-3797941100% (3)
- Drugs Used in Cardio Vascular SystemDocument138 pagesDrugs Used in Cardio Vascular SystemSagun lohalaNo ratings yet
- Drug Book 1Document89 pagesDrug Book 1PUNET KUMARNo ratings yet
- Chapter 2 - A - III Hypertension TreatmentDocument37 pagesChapter 2 - A - III Hypertension TreatmentEmmaNo ratings yet
- Drug StudyDocument96 pagesDrug StudyirismirzigNo ratings yet
- Chapter 35Document41 pagesChapter 35HannaNo ratings yet
- Anti Hypertensive DrugsDocument40 pagesAnti Hypertensive DrugsjawadNo ratings yet
- Common Misconceptions About HypertensionDocument31 pagesCommon Misconceptions About Hypertensionkirathsidhu.stitchNo ratings yet
- Cad Sihd 2Document67 pagesCad Sihd 2mohammedghassan53No ratings yet
- Vasodil - Ischemic Heart DiseaseDocument52 pagesVasodil - Ischemic Heart DiseaseNorms YoramNo ratings yet
- 15 - CCLS - PharmacologyDocument32 pages15 - CCLS - PharmacologyVENKATESH RAMSALINo ratings yet
- Antihypotensive Drugs: Roger Joseph Ii Ramos Jecino, RN, M.DDocument28 pagesAntihypotensive Drugs: Roger Joseph Ii Ramos Jecino, RN, M.DFranz Earl Niño AlbesaNo ratings yet
- Antihypertensives 1Document36 pagesAntihypertensives 1Muhammad Ilham HidayatNo ratings yet
- HPNDocument32 pagesHPNkaren GoNo ratings yet
- Drug StudyDocument3 pagesDrug StudyTrixia ArcegonoNo ratings yet
- CaptoprilDocument3 pagesCaptoprilapi-3797941100% (1)
- Case Presentation On Ischemic Cardiomyopathy & Ccf-1-1Document18 pagesCase Presentation On Ischemic Cardiomyopathy & Ccf-1-1Maliha aliNo ratings yet
- 40 Questions in CPRDocument16 pages40 Questions in CPRأبوأحمد الحكيمNo ratings yet
- Fundamentals of Nursing KeysDocument22 pagesFundamentals of Nursing KeysAijem Ryan0% (1)
- Newborn Nursing CareDocument23 pagesNewborn Nursing Careأبوأحمد الحكيمNo ratings yet
- Pediatric Genitourinary Nursing QuestionsDocument8 pagesPediatric Genitourinary Nursing Questionsأبوأحمد الحكيمNo ratings yet
- Adult 3 FinalDocument29 pagesAdult 3 Finalأبوأحمد الحكيم100% (1)
- 20 Questions in CPRDocument5 pages20 Questions in CPRأبوأحمد الحكيم100% (1)
- ملزمة منتدي الممرض الفلسطيني 2017 NewDocument37 pagesملزمة منتدي الممرض الفلسطيني 2017 Newأبوأحمد الحكيمNo ratings yet
- مزاولة شاميةDocument18 pagesمزاولة شاميةأبوأحمد الحكيمNo ratings yet
- Fundamentals of Nursing Test IIIDocument15 pagesFundamentals of Nursing Test IIIRose AnnNo ratings yet
- Inflammatory Cardiac Diseases ExplainedDocument96 pagesInflammatory Cardiac Diseases Explainedأبوأحمد الحكيمNo ratings yet
- نقابة التمريض الفلسطينية 7Document11 pagesنقابة التمريض الفلسطينية 7أبوأحمد الحكيمNo ratings yet
- Understanding Central Venous Pressure (CVPDocument50 pagesUnderstanding Central Venous Pressure (CVPأبوأحمد الحكيمNo ratings yet
- Heart FailureDocument49 pagesHeart Failureأبوأحمد الحكيمNo ratings yet
- PiC Mtg02 Insulin Chart-1Document1 pagePiC Mtg02 Insulin Chart-1أبوأحمد الحكيمNo ratings yet
- Mechanical Ventilation Modes and Settings ExplainedDocument84 pagesMechanical Ventilation Modes and Settings Explainedأبوأحمد الحكيم100% (1)
- Aortic Dissection AneurysmsDocument32 pagesAortic Dissection Aneurysmsأبوأحمد الحكيمNo ratings yet
- Cerebral Vascular DisorderDocument6 pagesCerebral Vascular Disorderأبوأحمد الحكيمNo ratings yet
- نقابة التمريض الفلسطينية 23Document7 pagesنقابة التمريض الفلسطينية 23أبوأحمد الحكيمNo ratings yet
- Human Growth Development PDFDocument498 pagesHuman Growth Development PDFأبوأحمد الحكيمNo ratings yet
- cardiomyopathy types and causesDocument39 pagescardiomyopathy types and causesأبوأحمد الحكيمNo ratings yet
- Diabetic Foot: N. Craig Stone April 17, 2003Document47 pagesDiabetic Foot: N. Craig Stone April 17, 2003Gabriel KlemensNo ratings yet
- Respiratory Disorders2Document11 pagesRespiratory Disorders2أبوأحمد الحكيمNo ratings yet
- Abruptio PlacentaDocument29 pagesAbruptio Placentaأبوأحمد الحكيمNo ratings yet
- Peripheral Vascular DisordersDocument15 pagesPeripheral Vascular Disordersأبوأحمد الحكيمNo ratings yet
- Neuro AssessmentDocument5 pagesNeuro Assessmentأبوأحمد الحكيمNo ratings yet
- Pediatric AntibioticsDocument3 pagesPediatric Antibioticsأبوأحمد الحكيمNo ratings yet
- Copd ExacerbationDocument42 pagesCopd Exacerbationأبوأحمد الحكيمNo ratings yet
- Pediatric AntibioticsDocument3 pagesPediatric Antibioticsأبوأحمد الحكيمNo ratings yet
- Spinal Cord DisordersDocument6 pagesSpinal Cord Disordersأبوأحمد الحكيمNo ratings yet
- BotoxMedical Patient BrochureDocument21 pagesBotoxMedical Patient BrochurePatricia Avalos C.No ratings yet
- SPIRIVA HandiHaler InstructionsDocument9 pagesSPIRIVA HandiHaler InstructionssamyvnNo ratings yet
- Medication DilutionDocument23 pagesMedication DilutionamgdanielaNo ratings yet
- Stabilis Monographie Ketorolac TromethamineDocument5 pagesStabilis Monographie Ketorolac Tromethamineintan kusumaningtyasNo ratings yet
- Format FormulairumDocument76 pagesFormat FormulairumfennyrahmaNo ratings yet
- Obcs 2012 02Document60 pagesObcs 2012 02nhanvn1No ratings yet
- Treatment of Constipation in Older Adult AAFPDocument8 pagesTreatment of Constipation in Older Adult AAFPTom KirklandNo ratings yet
- HTN Protocol 6.05Document2 pagesHTN Protocol 6.05Sergiu CiurdariuNo ratings yet
- BASIC PHARMACOKINETICS - CHAPTER 8: BioavailabilityDocument111 pagesBASIC PHARMACOKINETICS - CHAPTER 8: BioavailabilityDrHeba100% (10)
- ClonazepamDocument3 pagesClonazepamapi-3797941No ratings yet
- PFE PfizerDocument12 pagesPFE PfizerArthur HoNo ratings yet
- Librium ChlordiazepoxideDocument2 pagesLibrium ChlordiazepoxideENo ratings yet
- Drug Regulatory Affairs Syllabus KUDocument11 pagesDrug Regulatory Affairs Syllabus KUsathyasrireddyNo ratings yet
- Daftar Obat Psikotropika di Apotek PuspitDocument2 pagesDaftar Obat Psikotropika di Apotek Puspitapotek puspita0% (1)
- Courseregistration FormDocument1 pageCourseregistration FormBenjamin Dagmil Zamora IIINo ratings yet
- IV CompatibilityDocument44 pagesIV CompatibilityPhoebe SedantesNo ratings yet
- General Anesthesia and Sedation in DentistryDocument45 pagesGeneral Anesthesia and Sedation in DentistryIyad Abou-Rabii100% (2)
- Amitriptyline detection methods in blood using HPLCDocument8 pagesAmitriptyline detection methods in blood using HPLCJuan PerezNo ratings yet
- Sodium BicarbonateDocument8 pagesSodium BicarbonateRaf AylaniNo ratings yet
- Transitioning Anticoagulants 2016Document4 pagesTransitioning Anticoagulants 2016S_XangaiNo ratings yet
- Azacitidine V2 4.14Document3 pagesAzacitidine V2 4.14GabrielNo ratings yet
- DAFTAR OBAT HIGH ALERT DAN ELEKTROLIT KONSENTRATDocument2 pagesDAFTAR OBAT HIGH ALERT DAN ELEKTROLIT KONSENTRATBenk Nurhidayat SusiloNo ratings yet
- Brompheniramine (Bromax, Lodrane)Document8 pagesBrompheniramine (Bromax, Lodrane)Asniah Hadjiadatu AbdullahNo ratings yet
- Marketing Lecture 3 Updated Pharmaceutical Market ResearchDocument29 pagesMarketing Lecture 3 Updated Pharmaceutical Market ResearchAhmed AbdellahNo ratings yet
- Hypoglycemia Treatment ProtocolDocument1 pageHypoglycemia Treatment ProtocolCherryBeeNo ratings yet
- Critical Care Antibiotic GuideDocument1 pageCritical Care Antibiotic GuideAdna NelsonNo ratings yet
- Prozac (Fluoxetine) 40mgDocument1 pageProzac (Fluoxetine) 40mgENo ratings yet
- Brochure of PSI Platinum Plan Approved by WSUDocument46 pagesBrochure of PSI Platinum Plan Approved by WSUBalaji KartikNo ratings yet
- LGH Medical File From 302 by Detective Bearinger of Lancaster City Police of July 10, 2015unDocument25 pagesLGH Medical File From 302 by Detective Bearinger of Lancaster City Police of July 10, 2015unStan J. CaterboneNo ratings yet
- Geriatric Constipation ManagementDocument7 pagesGeriatric Constipation ManagementAdy Adha NorsanieNo ratings yet