You might also like
- Medical Record Documentation Standards For Practitioners: Aetna Better Health® of West VirginiaDocument3 pagesMedical Record Documentation Standards For Practitioners: Aetna Better Health® of West VirginiaMkamal MosaNo ratings yet
- Medical Audit of Inpatient Medical Records in A Tertiary Care Hospital - January - 2022 - 1381401306 - 8501173Document3 pagesMedical Audit of Inpatient Medical Records in A Tertiary Care Hospital - January - 2022 - 1381401306 - 8501173sanjay yadavNo ratings yet
- NapulanRM - Health Records Analysis and Clinical AuditDocument64 pagesNapulanRM - Health Records Analysis and Clinical AuditJeffreyReyesNo ratings yet
- QA Medical Record ReviewDocument4 pagesQA Medical Record ReviewJames JavierNo ratings yet
- Documentation by The Nurse: Texas Health and Human Services Quality Monitoring ProgramDocument35 pagesDocumentation by The Nurse: Texas Health and Human Services Quality Monitoring ProgramClaire Dean Sarmiento100% (1)
- To Error Is Human, To Persist in Error Is Diabolical:the Importance of Documentation in Medical PracticeDocument5 pagesTo Error Is Human, To Persist in Error Is Diabolical:the Importance of Documentation in Medical PracticeIJAR JOURNALNo ratings yet
- 1 Client Records 1Document15 pages1 Client Records 1Grape JuiceNo ratings yet
- Healthcare ProjectDocument13 pagesHealthcare ProjectDivyansh SrivastavaNo ratings yet
- Binder 1Document5 pagesBinder 1Walid YoussefNo ratings yet
- Health Information System Developmen T (Medical Records)Document21 pagesHealth Information System Developmen T (Medical Records)skidz137217100% (10)
- Chapter 02Document44 pagesChapter 02Carlos ChuNo ratings yet
- The Importance of Keeping Good Medical RecordsDocument3 pagesThe Importance of Keeping Good Medical RecordsLady ZahraNo ratings yet
- Specific Skills: Types of Documentation: 1. RecordingDocument5 pagesSpecific Skills: Types of Documentation: 1. Recordingmsah820No ratings yet
- 10 Principle in Medical DocumentationDocument4 pages10 Principle in Medical DocumentationKKCDIAL100% (1)
- (Nursing English) DIYAH AHADYATUNNISADocument10 pages(Nursing English) DIYAH AHADYATUNNISAdiyah hansuNo ratings yet
- HCM Module 5Document10 pagesHCM Module 5HisanaNo ratings yet
- Documentation and Coding Presentation Focuses on Risk AdjustmentDocument24 pagesDocumentation and Coding Presentation Focuses on Risk AdjustmentVANESSANo ratings yet
- Clinical Documentation Zuri March 28 2023Document36 pagesClinical Documentation Zuri March 28 2023KUYA CHICO MORALESNo ratings yet
- Medical Records Doc GuideDocument51 pagesMedical Records Doc Guidealwy aliNo ratings yet
- 1st Lecture ImprovedDocument26 pages1st Lecture ImprovedSahan SahANo ratings yet
- NC State University Veterinary Teaching Hospital Medical Records Documentation GuideDocument14 pagesNC State University Veterinary Teaching Hospital Medical Records Documentation GuideTriwanti TiagaNo ratings yet
- Lesson 5-The Medical Record As A Source DocumentDocument5 pagesLesson 5-The Medical Record As A Source DocumentSwamyNo ratings yet
- LILOY INTEGRATED HEALTH DISTRICT HOSPITAL - MarlynDocument7 pagesLILOY INTEGRATED HEALTH DISTRICT HOSPITAL - Marlynmarlyn donioNo ratings yet
- Coding & IndexingDocument26 pagesCoding & IndexingRahul RoyNo ratings yet
- Medical Records: Making and Retaining Them: What Is A Medical Record?Document6 pagesMedical Records: Making and Retaining Them: What Is A Medical Record?mfadly maulanaNo ratings yet
- Booklet 14 Keeping of Patience RecordsDocument12 pagesBooklet 14 Keeping of Patience RecordsNeo Mervyn MonahengNo ratings yet
- Medical Records and PX ChartDocument17 pagesMedical Records and PX ChartAi ÅiNo ratings yet
- Group11 MOPDocument5 pagesGroup11 MOPjilliantrcieNo ratings yet
- Integration of Administrative Responsibilities Into The HospitalDocument18 pagesIntegration of Administrative Responsibilities Into The HospitalNoor ButtNo ratings yet
- Documentation and Reporting in NursingDocument9 pagesDocumentation and Reporting in NursingMuruganNo ratings yet
- Quality IndicatorsDocument10 pagesQuality IndicatorsKanna NikithaNo ratings yet
- 1 Client Records EditedDocument38 pages1 Client Records EditedLiane Kc TawanaNo ratings yet
- Relevance of Nursing Documentation and Its Legal ImplicationsDocument8 pagesRelevance of Nursing Documentation and Its Legal ImplicationsGeorge AyiteyNo ratings yet
- Documenting Nursing ActivitiesDocument38 pagesDocumenting Nursing ActivitiesHoneylet Villanueva100% (1)
- Medical RecordsMedical ReportsDocument24 pagesMedical RecordsMedical ReportshaasviniNo ratings yet
- Assessment of The Documentation Completeness Level of The Medical Records in Basrah General HospitalDocument10 pagesAssessment of The Documentation Completeness Level of The Medical Records in Basrah General HospitalRajaa A. MahmoudNo ratings yet
- PatientCareDocDocument15 pagesPatientCareDocAra- Cvsu Francisco100% (2)
- NCM 103a W1 Patients Chart Module StudentsDocument3 pagesNCM 103a W1 Patients Chart Module StudentsNathaniel PulidoNo ratings yet
- Risk 201008 Medical Records and You PDFDocument4 pagesRisk 201008 Medical Records and You PDFFitra PringgayudaNo ratings yet
- Importance of DocumentationDocument2 pagesImportance of DocumentationSamantha Angeli CartonNo ratings yet
- Sample of Outdoor Medical Records SheetDocument11 pagesSample of Outdoor Medical Records Sheet27mickieNo ratings yet
- Med Record Auditor - Sample PagesDocument5 pagesMed Record Auditor - Sample PagesDaniel O. FernandezNo ratings yet
- Assignment InfoDocument4 pagesAssignment Infoabenezer g/kirstosNo ratings yet
- Collaborative Practice AgreementDocument3 pagesCollaborative Practice Agreementapi-228554702No ratings yet
- 2 Medical Record Documentation Guidelines - (Dpp-mrd-002-V2)Document4 pages2 Medical Record Documentation Guidelines - (Dpp-mrd-002-V2)shehab elsayedNo ratings yet
- MRD Meaning, FNDocument22 pagesMRD Meaning, FNRiya Pinto100% (1)
- Pharmacovigilance Monitoring in Clinical TrialsDocument26 pagesPharmacovigilance Monitoring in Clinical TrialsJAGADEESAN BALAJINo ratings yet
- 9 3 2012 Charting and DocumentationDocument44 pages9 3 2012 Charting and DocumentationMacrossBalaNo ratings yet
- 15 Define Process To Whom The Patient Record Can Be ReleasedDocument8 pages15 Define Process To Whom The Patient Record Can Be ReleasedSanjay KadamNo ratings yet
- Investigator Responsibilities in Clinical Research Mod 2Document6 pagesInvestigator Responsibilities in Clinical Research Mod 2Raquel VargasNo ratings yet
- Medical Records: An Introduction and OverviewDocument14 pagesMedical Records: An Introduction and OverviewZakwan AhmadNo ratings yet
- Documentation in NursingDocument41 pagesDocumentation in NursingGLAIZA PALATINONo ratings yet
- Medical Record Audit in Clinical Nursing Units in Tertiary HospitalDocument7 pagesMedical Record Audit in Clinical Nursing Units in Tertiary HospitalIOSRjournalNo ratings yet
- Nursing DocumentationDocument17 pagesNursing Documentationprema100% (4)
- NICU Documentation: Gama Hospital Al Khobar K.S.ADocument8 pagesNICU Documentation: Gama Hospital Al Khobar K.S.ALucian CaelumNo ratings yet
- @@assessment of Medical Documentation As Per Joint Commission InternationDocument6 pages@@assessment of Medical Documentation As Per Joint Commission InternationNahari ArifinNo ratings yet
- Documenting and ReportingDocument17 pagesDocumenting and ReportingalelichengNo ratings yet
- Medical Records Importance LawDocument14 pagesMedical Records Importance Law27mickie0% (1)
- Guidelines Releasing Pathology Results PatientsDocument4 pagesGuidelines Releasing Pathology Results PatientsNeelu PrasharNo ratings yet
- LAS IN ENTREPRENEURSHIP WEEK 4Document5 pagesLAS IN ENTREPRENEURSHIP WEEK 4IMELDA CORONACIONNo ratings yet
- Bridge Design Manual Part 3 - July14Final MASTERDocument50 pagesBridge Design Manual Part 3 - July14Final MASTERTsegawbezto75% (4)
- Gmail - DFA Passport Appointment System - Confirmation Notification PDFDocument2 pagesGmail - DFA Passport Appointment System - Confirmation Notification PDFGarcia efrilNo ratings yet
- Entrepreneurship & New Venture Management 6e - Chapter 1Document19 pagesEntrepreneurship & New Venture Management 6e - Chapter 1Hlulani Decision50% (2)
- Guided Overview of Impression MaterialsDocument212 pagesGuided Overview of Impression MaterialsSai Kumar100% (1)
- PDF Vertical Axis Wind Turbines DDDocument38 pagesPDF Vertical Axis Wind Turbines DDKunal AhiwaleNo ratings yet
- Nitro2 User Manual v2.24 PDFDocument29 pagesNitro2 User Manual v2.24 PDFReifesxd ProNo ratings yet
- 4 AppleDocument9 pages4 AppleSam Peter GeorgieNo ratings yet
- Malware Analysis Project ClusteringDocument11 pagesMalware Analysis Project ClusteringGilian kipkosgeiNo ratings yet
- Hello World in FortranDocument43 pagesHello World in Fortranhussein alsaedeNo ratings yet
- The Ultimate Experience With AvatradeDocument3 pagesThe Ultimate Experience With AvatradeAnonymous wk2GeJ8ERQNo ratings yet
- GPS Consent and TrackingDocument3 pagesGPS Consent and TrackingJoel KionisalaNo ratings yet
- Join in SQLDocument9 pagesJoin in SQLSugeenaNo ratings yet
- SCL 3711Document2 pagesSCL 3711MikeNo ratings yet
- Mid 185 - Pid 70 - Fmi 2Document3 pagesMid 185 - Pid 70 - Fmi 2Akbar100% (1)
- Power Engineering May 2013Document95 pagesPower Engineering May 2013Portal studentesc - EnergeticaNo ratings yet
- Consumer Behaviour 1Document11 pagesConsumer Behaviour 1Rushika ShahNo ratings yet
- PFRS SGV PDFDocument18 pagesPFRS SGV PDFJonathan Javier GajeNo ratings yet
- Palacio VsDocument2 pagesPalacio VsRaymart SalamidaNo ratings yet
- MSG 01084Document4 pagesMSG 01084testiandiniNo ratings yet
- L27 - Optical Measuring InstrumentsDocument14 pagesL27 - Optical Measuring Instrumentschaitanyamohod2020No ratings yet
- Hi Flow GroutDocument2 pagesHi Flow Groutpravi3434No ratings yet
- PharmacophoreDocument7 pagesPharmacophoresatheeshpharma6No ratings yet
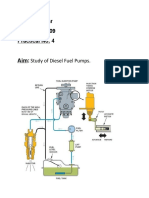
- Study of Diesel Fuel Pumps ComponentsDocument6 pagesStudy of Diesel Fuel Pumps ComponentsPro GamerssNo ratings yet
- ACCO 20073 Backflush CostingDocument2 pagesACCO 20073 Backflush CostingMaria Kathreena Andrea AdevaNo ratings yet
- Smith & Wesson Semi-Automatic Light Rifle HandbookDocument12 pagesSmith & Wesson Semi-Automatic Light Rifle Handbookxamxam0987654321100% (1)
- Solutions Manual For Introduction To Management Accounting 16Th Edition Horngren Sundem Schatzberg Burgstahler 0133058786 9780133058789 Full Chapter PDFDocument36 pagesSolutions Manual For Introduction To Management Accounting 16Th Edition Horngren Sundem Schatzberg Burgstahler 0133058786 9780133058789 Full Chapter PDFdavid.rex111100% (10)
- Free V Bucks Generator Vbucks1Document2 pagesFree V Bucks Generator Vbucks1Paula BoulesNo ratings yet
- Understanding Data GovernanceDocument28 pagesUnderstanding Data GovernanceJoe leninja100% (1)
- Anchor ChairDocument3 pagesAnchor ChairrsubramaniNo ratings yet