You might also like
- Death by Medicine 2003 PDFDocument46 pagesDeath by Medicine 2003 PDFportosinNo ratings yet
- Jurnal CA TyroidDocument4 pagesJurnal CA TyroidErvina ZelfiNo ratings yet
- Differential Diagnosis of Genital Ulcer Differential Diagnosis of Genital UlcersDocument3 pagesDifferential Diagnosis of Genital Ulcer Differential Diagnosis of Genital UlcersNurhayati HasanahNo ratings yet
- Candidosis A New ChallengeDocument7 pagesCandidosis A New ChallengeSalvador contreras huertaNo ratings yet
- Mycoplasma and UreaplasmaDocument17 pagesMycoplasma and UreaplasmaSteph ReyesNo ratings yet
- W2. 01. Introduction - To - Surveillance SerouriDocument53 pagesW2. 01. Introduction - To - Surveillance Serouriع كيف كيفك Dhaif-saeedNo ratings yet
- Covid ReportDocument20 pagesCovid ReportMarianne MartinezNo ratings yet
- Relative Trends in Hospitalizations and Mortality Among Infants by The Number of Vaccine Doses and Age, Based On The VAERS, 1990-2010Document10 pagesRelative Trends in Hospitalizations and Mortality Among Infants by The Number of Vaccine Doses and Age, Based On The VAERS, 1990-2010SY LodhiNo ratings yet
- Monkeypox External SitrepDocument11 pagesMonkeypox External SitrepEsty Saehaebath KaengendNo ratings yet
- Darah, TransfusiDocument157 pagesDarah, TransfusiRiza ZaharaNo ratings yet
- Oregon Health Authority COVID-19 Weekly Report (Published 10/7)Document31 pagesOregon Health Authority COVID-19 Weekly Report (Published 10/7)KGW NewsNo ratings yet
- Leading Causes of MortalityDocument12 pagesLeading Causes of MortalityJayricDepalobosNo ratings yet
- Oie E-2Document29 pagesOie E-2Khinci KeyenNo ratings yet
- Monkeypox External Sitrep FinalDocument11 pagesMonkeypox External Sitrep FinalAkshat SharmaNo ratings yet
- Guidelines Amoebiasis 2011 PDFDocument7 pagesGuidelines Amoebiasis 2011 PDFVickha Dian HapsariNo ratings yet
- Monitoring The Outbreak: Regulations For Disease Reporting and Control, It Has Been Clarified ThatDocument5 pagesMonitoring The Outbreak: Regulations For Disease Reporting and Control, It Has Been Clarified ThatShaina Fe RabaneraNo ratings yet
- PowerPoint UDRS Training CityStateDocument276 pagesPowerPoint UDRS Training CityStateAprilAngeliRoble100% (1)
- Michael Gregg - Field Epidemiology Tahap Awal InvestigasiDocument61 pagesMichael Gregg - Field Epidemiology Tahap Awal InvestigasiMegan TariNo ratings yet
- Oregon Health Authority COVID-19 Weekly Report (Published 10/28)Document38 pagesOregon Health Authority COVID-19 Weekly Report (Published 10/28)KGW NewsNo ratings yet
- Protocol On Idsr002 Reporting at The Health Facilities Guided by The New Idsr Technical Guideline, 3 EditionDocument3 pagesProtocol On Idsr002 Reporting at The Health Facilities Guided by The New Idsr Technical Guideline, 3 EditionSalihu MustaphaNo ratings yet
- Reporting Sars-Cov-2 To The Oie: Code, "A New Occurrence in AnDocument3 pagesReporting Sars-Cov-2 To The Oie: Code, "A New Occurrence in AnAZUCENANo ratings yet
- Gastriccancer: Epidemiology and Risk FactorsDocument22 pagesGastriccancer: Epidemiology and Risk FactorsRaul RamirezNo ratings yet
- St. Louis County Health Department COVID-19 Report For Sept. 2, 2021Document24 pagesSt. Louis County Health Department COVID-19 Report For Sept. 2, 2021KSDKNo ratings yet
- Jegh 9 4 217Document6 pagesJegh 9 4 21715Mega RahmaniNo ratings yet
- Functional History: Abilities After and PrognosisDocument7 pagesFunctional History: Abilities After and PrognosisIcaroNo ratings yet
- Oregon COVID-19 Weekly Report (Published Oct. 21, 2020)Document33 pagesOregon COVID-19 Weekly Report (Published Oct. 21, 2020)KGW NewsNo ratings yet
- First Data On The Disease Associated With Vaping in ColombiaDocument19 pagesFirst Data On The Disease Associated With Vaping in Colombiadiegoud2003No ratings yet
- OIE Standards and Guidelines Related To Trade and Poultry DiseasesDocument7 pagesOIE Standards and Guidelines Related To Trade and Poultry DiseasesMuhammad AnwarNo ratings yet
- CESU ORD DRAFT EDITED Sent To Dr. AlfieDocument7 pagesCESU ORD DRAFT EDITED Sent To Dr. AlfieDulce TomotorgoNo ratings yet
- 2 LeprosyDocument3 pages2 Leprosyapi-281306164No ratings yet
- Key Updates For Week 15, Ending April 11, 2020: VirusDocument41 pagesKey Updates For Week 15, Ending April 11, 2020: Viruseka dyahNo ratings yet
- Melioidosis Cases and Selected Reports of Occupational Exposures To Burkholderia Pseudomallei - United States, 2008-2013Document12 pagesMelioidosis Cases and Selected Reports of Occupational Exposures To Burkholderia Pseudomallei - United States, 2008-2013worksheetbookNo ratings yet
- Articulo 4Document5 pagesArticulo 4Daniella Rodriguez ReyesNo ratings yet
- Notified TB Cases: (Absolute Numbers)Document37 pagesNotified TB Cases: (Absolute Numbers)ComingSoonNo ratings yet
- Newly Diagnosed HIV Cases in The Philippines: National Epidemiology CenterDocument3 pagesNewly Diagnosed HIV Cases in The Philippines: National Epidemiology Centerkbl27No ratings yet
- Social Mobilization Revitalization - Final - ENGLISH EditedDocument138 pagesSocial Mobilization Revitalization - Final - ENGLISH EditedAyeleNo ratings yet
- 2020 05 05 20054361v2 FullDocument32 pages2020 05 05 20054361v2 FullFelipe BrandãoNo ratings yet
- Cancer Incidence in Jordan 2016Document36 pagesCancer Incidence in Jordan 2016Ja'far HishamNo ratings yet
- Livestock Disease Control Regulations-RIS-final-wordDocument86 pagesLivestock Disease Control Regulations-RIS-final-wordnupurindus42893No ratings yet
- Hospitals, Morbidity and Mortality in The Philippines by HM PellejoDocument5 pagesHospitals, Morbidity and Mortality in The Philippines by HM PellejoHannah Marquiala PellejoNo ratings yet
- A Wealth of Information On Global Public HealthDocument12 pagesA Wealth of Information On Global Public HealthcephalicaNo ratings yet
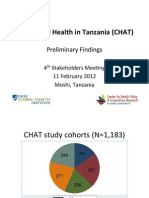
- Coping and Health in Tanzania (CHAT) : Preliminary FindingsDocument27 pagesCoping and Health in Tanzania (CHAT) : Preliminary Findingskyle_hamilton9947No ratings yet
- 45 20200213 Covid 19Document6 pages45 20200213 Covid 19rite nezzartNo ratings yet
- MT Law Topic 3Document23 pagesMT Law Topic 3Eran Mark RojasNo ratings yet
- Emergency Department Visits and Hospitalizations For Selected Nonfatal Injuries Among Adults Aged 65 Years - United States, 2018Document32 pagesEmergency Department Visits and Hospitalizations For Selected Nonfatal Injuries Among Adults Aged 65 Years - United States, 2018worksheetbookNo ratings yet
- NCR 2017 MoH Final Report Nov 2018 10.12.2018Document33 pagesNCR 2017 MoH Final Report Nov 2018 10.12.2018Veden SoobenNo ratings yet
- Ungass Country Progress Report Australia: Reporting Period: January 2006-December 2007 Submission Date: 15 January 2008Document16 pagesUngass Country Progress Report Australia: Reporting Period: January 2006-December 2007 Submission Date: 15 January 2008Pradeep George BabuNo ratings yet
- Needle Stick InjuryDocument6 pagesNeedle Stick InjuryNikitaNo ratings yet
- Tbnet 2005-2009: Continuity of Care For TB Patients Around The WorldDocument6 pagesTbnet 2005-2009: Continuity of Care For TB Patients Around The WorldlymorenoNo ratings yet
- 363713v1 FullDocument27 pages363713v1 FullALI MAKRINo ratings yet
- 16th April Daily News UMDocument18 pages16th April Daily News UMRaja KrNo ratings yet
- The European Medical Technology Industry in Figures 2020Document44 pagesThe European Medical Technology Industry in Figures 2020AbhishekNo ratings yet
- Newly Diagnosed HIV Cases in The Philippines: National Epidemiology CenterDocument4 pagesNewly Diagnosed HIV Cases in The Philippines: National Epidemiology CenternajafraganteNo ratings yet
- Cancer Registry Standard Operating ProceduresDocument3 pagesCancer Registry Standard Operating ProceduresAnan AghbarNo ratings yet
- World Malaria Report 2012Document286 pagesWorld Malaria Report 2012mwenyewe100% (2)
- Science Abc3517 FullDocument9 pagesScience Abc3517 FullroopNo ratings yet
- Whitehouse Ohio 10-11-20Document10 pagesWhitehouse Ohio 10-11-20Anne SakerNo ratings yet
- Global Socioeconomic Impact of Cystic Echinococcosis: Christine M. Budke, Peter Deplazes, and Paul R. TorgersonDocument14 pagesGlobal Socioeconomic Impact of Cystic Echinococcosis: Christine M. Budke, Peter Deplazes, and Paul R. TorgersonPlok PlotNo ratings yet
- Assessment of COVID-19 Pandemic in Nepal: A Lockdown Scenario AnalysisDocument13 pagesAssessment of COVID-19 Pandemic in Nepal: A Lockdown Scenario Analysispopov357No ratings yet
- Lung Cancer Peru 2020Document8 pagesLung Cancer Peru 2020Anthony Jason Castro JustinianoNo ratings yet
- World Cancer Report 2008Document260 pagesWorld Cancer Report 2008Donciu AlexandraNo ratings yet
- Acrr 2018Document28 pagesAcrr 2018Aliyan ZafarNo ratings yet
- Tuberculosis - Knowledge at AMBOSSDocument4 pagesTuberculosis - Knowledge at AMBOSSKC Dela RosaNo ratings yet
- Plant ProtectionDocument9 pagesPlant ProtectionPooja BhusalNo ratings yet
- C-Reactive Protein: Key FactsDocument12 pagesC-Reactive Protein: Key FactsAngel CañaresNo ratings yet
- Essay HI 4 LIADocument4 pagesEssay HI 4 LIANorbertus MarcellNo ratings yet
- Incidence of Intestinal Helminthes Among HIV Patients at Kampala International University Teaching Hospital, Uganda.Document12 pagesIncidence of Intestinal Helminthes Among HIV Patients at Kampala International University Teaching Hospital, Uganda.KIU PUBLICATION AND EXTENSIONNo ratings yet
- Viro OLADocument1 pageViro OLABenjamin SantiagoNo ratings yet
- Pneumonia CBLDocument22 pagesPneumonia CBLImAlien OrGodNo ratings yet
- Common Illnesses and Diseases of School-Aged ChildrenDocument2 pagesCommon Illnesses and Diseases of School-Aged ChildrenKnucasior BichNo ratings yet
- TPT Talking Points BookletDocument9 pagesTPT Talking Points BookletNasasira BensonNo ratings yet
- Explanation of The Physical ExaminationDocument3 pagesExplanation of The Physical ExaminationShuvo AhmedNo ratings yet
- Food Borne Diseases - 0Document131 pagesFood Borne Diseases - 0Nur FithriahNo ratings yet
- EO 7 S 2021 Creation-Of-CODE-Team - BarangayDocument2 pagesEO 7 S 2021 Creation-Of-CODE-Team - BarangayBARANGAY MOLINO IINo ratings yet
- Health 8 Poster MakingDocument9 pagesHealth 8 Poster MakingDe Leon, Aaron MarcusNo ratings yet
- Contingency Plan On Covid-19: Mahabang Sapa Elementary SchoolDocument13 pagesContingency Plan On Covid-19: Mahabang Sapa Elementary SchoolKriselle May DeslateNo ratings yet
- Laboratory Investigation ReportDocument1 pageLaboratory Investigation ReportMd blackNo ratings yet
- San TiDocument9 pagesSan TiMishael Kevin BuenaNo ratings yet
- Pre Travel Mosquitos SnakesDocument59 pagesPre Travel Mosquitos SnakesIsrael EspinNo ratings yet
- Physical Exam Form PDFDocument3 pagesPhysical Exam Form PDFOktavianNo ratings yet
- Minor Emergencies (Third Edition)Document3 pagesMinor Emergencies (Third Edition)Estefanía Castañeda MoralesNo ratings yet
- Dental Occupational SafetyDocument99 pagesDental Occupational SafetyHina HusnainNo ratings yet
- Artículo COVID-19 Alimentos (Prensa)Document11 pagesArtículo COVID-19 Alimentos (Prensa)TatianaNo ratings yet
- Subcutaneous MycosesDocument17 pagesSubcutaneous MycosesSit IsahNo ratings yet
- Severe Acute Respiratory Syndrome Coronavirus 2Document31 pagesSevere Acute Respiratory Syndrome Coronavirus 2Ian VillacrusisNo ratings yet
- Health Checkup - Kathmandu - IOMDocument3 pagesHealth Checkup - Kathmandu - IOMas afNo ratings yet
- 2.opportunistic Infections in HIV-infected PatientsDocument53 pages2.opportunistic Infections in HIV-infected PatientsAbebe TilahunNo ratings yet
- DiseaseResearchProject 1Document3 pagesDiseaseResearchProject 1Racheal MukiriNo ratings yet
- Lecture 1 The Background of HIVDocument32 pagesLecture 1 The Background of HIVAPONDI SIMON ODONGONo ratings yet