You might also like
- 2013 Kendrick KayDocument15 pages2013 Kendrick KayDr-Raheel ZafarNo ratings yet
- Differential Electrophysiological Response During Rest, Self-Referential, and Non - Self-Referential Tasks in Human Posteromedial CortexDocument6 pagesDifferential Electrophysiological Response During Rest, Self-Referential, and Non - Self-Referential Tasks in Human Posteromedial CortexTonitha Nahui-Ollin AraizaNo ratings yet
- An fMRI Stroop Task Study of Ventromedial Prefrontal Cortical Function in Pathological GamblersDocument5 pagesAn fMRI Stroop Task Study of Ventromedial Prefrontal Cortical Function in Pathological Gamblersmihaimihai5No ratings yet
- 2009 Cheng Schizophrenia Classification Using Regions of Interest in Brain MRIDocument6 pages2009 Cheng Schizophrenia Classification Using Regions of Interest in Brain MRImarciliomeiraNo ratings yet
- Mental Rotations Um, LÑKM,, (PDocument6 pagesMental Rotations Um, LÑKM,, (PAlfonsoNo ratings yet
- Beck LavieDocument6 pagesBeck LavieDanutza CezNo ratings yet
- Cerebelo en Hiperactividad y Deficit de AtencionDocument7 pagesCerebelo en Hiperactividad y Deficit de AtencionLiliann RiveraNo ratings yet
- Schiff Nature MedecineDocument2 pagesSchiff Nature MedecinePadma DorjeNo ratings yet
- Durably Reducing Transphobia: A Field Experiment On Door-To-Door CanvassingDocument6 pagesDurably Reducing Transphobia: A Field Experiment On Door-To-Door CanvassingLilimoon MaldonadoNo ratings yet
- Pusher Syndrome: Its Cortical CorrelateDocument7 pagesPusher Syndrome: Its Cortical Correlatepokharelriwaj82No ratings yet
- The Functional Anatomy of Attention To Visual Motion: A Functional MRI StudyDocument14 pagesThe Functional Anatomy of Attention To Visual Motion: A Functional MRI StudySam StuartNo ratings yet
- Hipofrontalidad y WM en EsquizofreniaDocument5 pagesHipofrontalidad y WM en EsquizofreniaGuillermo A ManriqueNo ratings yet
- Neuroimage: Clinical: Cyril Atkinson-Clement, Serge Pinto, Alexandre Eusebio, Olivier CoulonDocument13 pagesNeuroimage: Clinical: Cyril Atkinson-Clement, Serge Pinto, Alexandre Eusebio, Olivier CoulonKanagaraj SubramaniNo ratings yet
- Raven Prabhakaran1997 PDFDocument21 pagesRaven Prabhakaran1997 PDFargiaescuNo ratings yet
- C.A. - Estudo de ImagensDocument11 pagesC.A. - Estudo de ImagensPedro ValentimNo ratings yet
- Motion Induced Position Mis-Localization Predicts The Severity of Alzheimer DiseaseDocument13 pagesMotion Induced Position Mis-Localization Predicts The Severity of Alzheimer DiseaseZsuzsan LicaNo ratings yet
- Money RoadDocument9 pagesMoney RoadVicente CáceresNo ratings yet
- Interactions Between Posterior Gamma and Frontal Alpha/beta Oscillations During Imagined ActionsDocument12 pagesInteractions Between Posterior Gamma and Frontal Alpha/beta Oscillations During Imagined ActionsoroborobNo ratings yet
- Further Analyses of Clock Drawings Among Demented and Nondemented Older SubjectsDocument13 pagesFurther Analyses of Clock Drawings Among Demented and Nondemented Older Subjectsroberta schiavoneNo ratings yet
- 5 - Aerobic Exercise Alters Brain Function and Structure in Parkinson's Disease A Randomized Controlled TrialDocument14 pages5 - Aerobic Exercise Alters Brain Function and Structure in Parkinson's Disease A Randomized Controlled TrialGabriel NevesNo ratings yet
- Visuomotor Learning in Immersive 3D Virtual Reality in Parkinson's Disease and in AgingDocument18 pagesVisuomotor Learning in Immersive 3D Virtual Reality in Parkinson's Disease and in AgingKristineNo ratings yet
- Cognition and Mood in Parkinson's Disease in Subthalamic Nucleus Versus Globus Pallidus Interna Deep Brain Stimulation The COMPARE TrialDocument10 pagesCognition and Mood in Parkinson's Disease in Subthalamic Nucleus Versus Globus Pallidus Interna Deep Brain Stimulation The COMPARE TrialRicardo GarciaNo ratings yet
- The Adaptative Digit Ordering Test. Clicinal Applicarion, Reliability, and Validity of A Verbal Working Memory Test. Katja WerdheidDocument19 pagesThe Adaptative Digit Ordering Test. Clicinal Applicarion, Reliability, and Validity of A Verbal Working Memory Test. Katja WerdheidRodolfo PalleroNo ratings yet
- tmp6236 TMPDocument12 pagestmp6236 TMPFrontiersNo ratings yet
- Frontal White Matter Microstructure and Treatment Response of Late-Life Depression: A Preliminary StudyDocument4 pagesFrontal White Matter Microstructure and Treatment Response of Late-Life Depression: A Preliminary StudySharon AdeleNo ratings yet
- Déficit de Control Ejecutivo en La Depresión, Potenciales Relacionados Con Eventos en Una TareaDocument16 pagesDéficit de Control Ejecutivo en La Depresión, Potenciales Relacionados Con Eventos en Una TareaMiguel Ángel DominguezNo ratings yet
- Medciones de Atrofia Cronica ViejitoDocument5 pagesMedciones de Atrofia Cronica ViejitoFernando Dueñas MoralesNo ratings yet
- Poppelreuter-Ghent's Overlapping Figures Test ItsDocument24 pagesPoppelreuter-Ghent's Overlapping Figures Test ItsHarold Vivas100% (1)
- Coordincoj AutismoDocument14 pagesCoordincoj AutismoEvelyn Esther Díaz HarosNo ratings yet
- Accepted Manuscript: 10.1016/j.jpain.2015.08.008Document30 pagesAccepted Manuscript: 10.1016/j.jpain.2015.08.008Ayat BissNo ratings yet
- 1 s2.0 S088761770100124X Main PDFDocument16 pages1 s2.0 S088761770100124X Main PDFFlorina AndreiNo ratings yet
- Mental Rotation Ability of Individuals W PDFDocument8 pagesMental Rotation Ability of Individuals W PDFEliMihaelaNo ratings yet
- Neural Correlates of Reward in AutismDocument7 pagesNeural Correlates of Reward in AutismLaumart HukomNo ratings yet
- Thilo Hinterberger, Joop M. Houtkooper and Boris Kotchoubey - Effects of Feedback Control On Slow Cortical Potentials and Random EventsDocument12 pagesThilo Hinterberger, Joop M. Houtkooper and Boris Kotchoubey - Effects of Feedback Control On Slow Cortical Potentials and Random EventsSorrenneNo ratings yet
- Imitating: Gestures Quantitative Approach ApraxiaDocument5 pagesImitating: Gestures Quantitative Approach ApraxiaJulian GorositoNo ratings yet
- 3 Parcial An Isela ArticuloDocument11 pages3 Parcial An Isela ArticuloDaisy RomeroNo ratings yet
- Atypical Eye Gaze Perception inDocument21 pagesAtypical Eye Gaze Perception inLeandro FerrazNo ratings yet
- Subliminal Words Durably A¡ect Neuronal ActivityDocument5 pagesSubliminal Words Durably A¡ect Neuronal ActivityNguyen Hong HaNo ratings yet
- Theta-Burst Transcranial Magnetic Stimulation To The Prefrontal Cortex Impairs Metacognitive Visual AwarenessDocument12 pagesTheta-Burst Transcranial Magnetic Stimulation To The Prefrontal Cortex Impairs Metacognitive Visual Awarenessdpf050No ratings yet
- Muniz 2010Document7 pagesMuniz 2010seyedmohamadNo ratings yet
- Lilli Crap 2013Document13 pagesLilli Crap 2013Víctor FuentesNo ratings yet
- Ingle, DJ. Jeannerod, M. Lee, DN. Brain Mechanisms and Spatial Vision (1985) PDFDocument468 pagesIngle, DJ. Jeannerod, M. Lee, DN. Brain Mechanisms and Spatial Vision (1985) PDFMauro CracchioloNo ratings yet
- Ivry1988 - Article - DissociationOfTheLateralAndMed N PDFDocument14 pagesIvry1988 - Article - DissociationOfTheLateralAndMed N PDFFábio SagginNo ratings yet
- 28 Svatkova2015Document10 pages28 Svatkova2015Sergio Machado NeurocientistaNo ratings yet
- Ana 24309Document14 pagesAna 24309cah bagusNo ratings yet
- Deficits Thalamic: in Human Visual Spatial Attention Following LesionsDocument5 pagesDeficits Thalamic: in Human Visual Spatial Attention Following LesionsmartingolicruzNo ratings yet
- Neural Substrates of Fluid Reasoning: An fMRI Study of Neocortical Activation During Performance of The Raven's Progressive Matrices TestDocument21 pagesNeural Substrates of Fluid Reasoning: An fMRI Study of Neocortical Activation During Performance of The Raven's Progressive Matrices TestAviraj MahadikNo ratings yet
- Use and Admissibility of Positron Emission Tomography (PET) Scanning in Head InjuryDocument59 pagesUse and Admissibility of Positron Emission Tomography (PET) Scanning in Head InjuryPrateek DubeyNo ratings yet
- Esquizofrenia e Arte TerapiaDocument2 pagesEsquizofrenia e Arte TerapiaBruno PerazioNo ratings yet
- Scalp Topography and Analysis of Intracranial SourcesDocument9 pagesScalp Topography and Analysis of Intracranial SourcesQualidade CSVHNo ratings yet
- 2 DBSDocument8 pages2 DBSHamzeh AlsalhiNo ratings yet
- Brain 2003 Siebner 2710 25Document16 pagesBrain 2003 Siebner 2710 25huanc_5No ratings yet
- Stimulation of Subthalamic Nuclei Restores A Near Normal Planning Strategy in Parkinson's PatientsDocument10 pagesStimulation of Subthalamic Nuclei Restores A Near Normal Planning Strategy in Parkinson's PatientsmcgilicuttyNo ratings yet
- A Four Dimensional Model of Vertebral SubluxationDocument4 pagesA Four Dimensional Model of Vertebral SubluxationrewassallfotosNo ratings yet
- A Comprehensive Framework For Differentiating Autism Spectrum Disorder From Neurotypicals by Fusing Structural MRI and Resting State Functional MRIDocument12 pagesA Comprehensive Framework For Differentiating Autism Spectrum Disorder From Neurotypicals by Fusing Structural MRI and Resting State Functional MRITaNiTa TiKaRaNNo ratings yet
- NIH Public Access: Cerebral Hemispherectomy: Sensory Scores Before and After Intensive Mobility TrainingDocument11 pagesNIH Public Access: Cerebral Hemispherectomy: Sensory Scores Before and After Intensive Mobility TrainingBimantoro SaputroNo ratings yet
- Carvalho Et Al 2013-HeadacheDocument7 pagesCarvalho Et Al 2013-Headachecris.endo.ceNo ratings yet
- Brain Potentials Associated With Voluntary Manual Tracking_ Bereitschaftspotential, Conditioned Premotion Positivity, Directed...Tivity of the Limbic and Frontal Cortex (Annals of the Lyceum of Natural History of New York, Vol. 425, Issue None) (1984)Document15 pagesBrain Potentials Associated With Voluntary Manual Tracking_ Bereitschaftspotential, Conditioned Premotion Positivity, Directed...Tivity of the Limbic and Frontal Cortex (Annals of the Lyceum of Natural History of New York, Vol. 425, Issue None) (1984)antonioopNo ratings yet
- Journal 7 N.vii 7Document5 pagesJournal 7 N.vii 7Azmi FananyNo ratings yet
- Evaluation of Acute Pelvic Pain in Nonpregnant Adult Women - UpToDate PDFDocument34 pagesEvaluation of Acute Pelvic Pain in Nonpregnant Adult Women - UpToDate PDFVictor MarquesNo ratings yet
- Evaluation and Management of Ruptured Ovarian Cyst - UpToDate PDFDocument21 pagesEvaluation and Management of Ruptured Ovarian Cyst - UpToDate PDFVictor MarquesNo ratings yet
- Pelvic Inflammatory Disease - Clinical Manifestations and Diagnosis - UpToDate PDFDocument16 pagesPelvic Inflammatory Disease - Clinical Manifestations and Diagnosis - UpToDate PDFVictor MarquesNo ratings yet
- Classification and Causes of Jaundice or Asymptomatic HyperbilirubinemiaDocument22 pagesClassification and Causes of Jaundice or Asymptomatic HyperbilirubinemiaVictor MarquesNo ratings yet
- Diagnostic Approach To The Adult With Jaundice or Asymptomatic Hyperbilirubinemia - UpToDateDocument17 pagesDiagnostic Approach To The Adult With Jaundice or Asymptomatic Hyperbilirubinemia - UpToDateVictor MarquesNo ratings yet
- Diagnostic Approach To The Adult With Jaundice or Asymptomatic Hyperbilirubinemia - UpToDateDocument17 pagesDiagnostic Approach To The Adult With Jaundice or Asymptomatic Hyperbilirubinemia - UpToDateVictor MarquesNo ratings yet
- A Deep Analysis of A Peace of Shit PDFDocument8 pagesA Deep Analysis of A Peace of Shit PDFVictor MarquesNo ratings yet
- Viral and Metabolic Factors Influencing Alanine Aminotransferase PDFDocument7 pagesViral and Metabolic Factors Influencing Alanine Aminotransferase PDFVictor MarquesNo ratings yet
- Viral and Metabolic Factors Influencing Alanine AminotransferaseDocument8 pagesViral and Metabolic Factors Influencing Alanine AminotransferaseVictor MarquesNo ratings yet
- Original: ArticleDocument9 pagesOriginal: ArticleVictor MarquesNo ratings yet
- 21 Rinite Como Fator de Associaçâo de Ansiedade e DepressâoDocument7 pages21 Rinite Como Fator de Associaçâo de Ansiedade e DepressâoVictor MarquesNo ratings yet
- Work & Stress: An International Journal of Work, Health & OrganisationsDocument17 pagesWork & Stress: An International Journal of Work, Health & OrganisationsVictor MarquesNo ratings yet
- Genética Clínica 2Document10 pagesGenética Clínica 2Victor MarquesNo ratings yet
- Kick-Ass Customer Service-Part 1Document3 pagesKick-Ass Customer Service-Part 1Mahfuzul Haque SujanNo ratings yet
- Module 6 - Using and Evaluating Instructional MaterialsDocument5 pagesModule 6 - Using and Evaluating Instructional MaterialsMaria Victoria Padro100% (4)
- 9A02505 Electrical Machines-IIIDocument4 pages9A02505 Electrical Machines-IIIsivabharathamurthyNo ratings yet
- Karyn Corbett Pedagogy Letter To SelfDocument2 pagesKaryn Corbett Pedagogy Letter To Selfapi-513861296No ratings yet
- (English (Auto-Generated) ) Intraday Trading On Nifty (2nd September, 2021) 8 Lakhs Profit Shreyas Bandi Trade Ideas Live (DownSub - Com)Document41 pages(English (Auto-Generated) ) Intraday Trading On Nifty (2nd September, 2021) 8 Lakhs Profit Shreyas Bandi Trade Ideas Live (DownSub - Com)YaaroNo ratings yet
- Rexroth Hd2 ControlairDocument15 pagesRexroth Hd2 ControlairRafaelNo ratings yet
- Sem06 Gca InsoDocument2 pagesSem06 Gca InsoBogdan PistolNo ratings yet
- PASSAGE ONE (Questions 1-4)Document5 pagesPASSAGE ONE (Questions 1-4)Vian LonkzeerNo ratings yet
- Dimensions and Methodology of Business Studies Dec 2018Document2 pagesDimensions and Methodology of Business Studies Dec 2018Nallavenaaya Unni100% (1)
- Assignment 4Document2 pagesAssignment 4Komal SinghNo ratings yet
- Basic Electrical Safety Module 1Document39 pagesBasic Electrical Safety Module 1malawi200No ratings yet
- Detailed Lesson Plan in Mathematics 10 I. ObjectivesDocument4 pagesDetailed Lesson Plan in Mathematics 10 I. ObjectivesLouis Fetilo FabunanNo ratings yet
- ENGLISH TOEFL Structure (3rd Exercise)Document5 pagesENGLISH TOEFL Structure (3rd Exercise)susannnnnnNo ratings yet
- Steam TableDocument3 pagesSteam TableMUHAMAD SAUKINo ratings yet
- Ficha Tecnica Reflector 2000W Led Lluminacion de Campos de Futbol Estadios Goled Philips Osram Opalux LedDocument5 pagesFicha Tecnica Reflector 2000W Led Lluminacion de Campos de Futbol Estadios Goled Philips Osram Opalux Ledluis perdigonNo ratings yet
- A Brief Tutorial On Studio MonitorsDocument18 pagesA Brief Tutorial On Studio MonitorsCurtis O'BrienNo ratings yet
- Staad 4Document37 pagesStaad 4saisssms9116100% (2)
- Pepperl KFD2 STC4 EX1.20 DatasheetDocument2 pagesPepperl KFD2 STC4 EX1.20 DatasheetAhmed HusseinNo ratings yet
- Chess AI: Competing Paradigms For Machine Intelligence: Shiva Maharaj Nick Polson Alex TurkDocument15 pagesChess AI: Competing Paradigms For Machine Intelligence: Shiva Maharaj Nick Polson Alex TurkDomingo IslasNo ratings yet
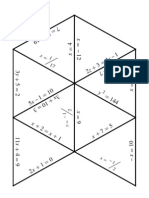
- Algebra1 Review PuzzleDocument3 pagesAlgebra1 Review PuzzleNicholas Yates100% (1)
- IES 2001 - I ScanDocument20 pagesIES 2001 - I ScanK.v.SinghNo ratings yet
- Mech Syllabus R-2017 - 1Document110 pagesMech Syllabus R-2017 - 1goujjNo ratings yet
- Evs ManualDocument24 pagesEvs ManualJoseph TuckerNo ratings yet
- Fiitjee All India Test Series: Concept Recapitulation Test - Iv JEE (Advanced) - 2019Document13 pagesFiitjee All India Test Series: Concept Recapitulation Test - Iv JEE (Advanced) - 2019Raj KumarNo ratings yet
- Theory 2 - The Demand of The Society From The Teacher As A Professional (PPST)Document6 pagesTheory 2 - The Demand of The Society From The Teacher As A Professional (PPST)Angel RodriguezNo ratings yet
- ENIRAM - Guide To Dynamic Trim Optimization 280611 PDFDocument14 pagesENIRAM - Guide To Dynamic Trim Optimization 280611 PDFPhineas MagellanNo ratings yet
- WideScreen Code For PS2 GamesDocument78 pagesWideScreen Code For PS2 Gamesmarcus viniciusNo ratings yet
- Budget of Work Inquiries Investigations and Immersion 19 20Document1 pageBudget of Work Inquiries Investigations and Immersion 19 20alma florNo ratings yet
- WebpdfDocument276 pagesWebpdfprateekvNo ratings yet
- Full TextDocument167 pagesFull Textjon minanNo ratings yet