You might also like
- Textbook of Urgent Care Management: Chapter 41, Measuring and Improving Patient SatisfactionFrom EverandTextbook of Urgent Care Management: Chapter 41, Measuring and Improving Patient SatisfactionNo ratings yet
- Complex, Pakistan BY Muhammad Ali (Baskent University Ankara) & Majid Khan (Yildirim Beyazit University Ankara)Document22 pagesComplex, Pakistan BY Muhammad Ali (Baskent University Ankara) & Majid Khan (Yildirim Beyazit University Ankara)IraaNo ratings yet
- Assessment of Service Quality Dimensions in Healthcare Industry A Study On Patient's Satisfaction With Bangladeshi Private HospitalsDocument9 pagesAssessment of Service Quality Dimensions in Healthcare Industry A Study On Patient's Satisfaction With Bangladeshi Private HospitalsZakariya BelalNo ratings yet
- Patient Satisfaction Survey at A Tertiary Care Speciality HospitalDocument5 pagesPatient Satisfaction Survey at A Tertiary Care Speciality HospitalJasneep0% (1)
- Consumer Perception On Service Quality in Health Care SectorDocument4 pagesConsumer Perception On Service Quality in Health Care SectorAmit Chauhan R.No ratings yet
- Patient's Satisfaction With Nursing Care Provided in Selected Areas of Tertiary Care Hospital 1Document13 pagesPatient's Satisfaction With Nursing Care Provided in Selected Areas of Tertiary Care Hospital 1Anonymous CuWlCKxXkENo ratings yet
- Service Quality Measurement in Health Care System: A Study of Patient Satisfaction On Healthcare of Dhaka CityDocument27 pagesService Quality Measurement in Health Care System: A Study of Patient Satisfaction On Healthcare of Dhaka CityKhaled KalamNo ratings yet
- Service quality factors in health careDocument12 pagesService quality factors in health careaqeel shoukatNo ratings yet
- Asamrew (2020) Level of Patient Satisfaction With Inpatient Services and Its Determinants A Study of A Specialized Hospital in EthiopiaDocument12 pagesAsamrew (2020) Level of Patient Satisfaction With Inpatient Services and Its Determinants A Study of A Specialized Hospital in EthiopiaDiego RiveraNo ratings yet
- How Patients Perceive Healthcare Services A Case of Ayub Teaching Hospital, Abbottabad - Pakistan. SERV Service QUAL QualityDocument9 pagesHow Patients Perceive Healthcare Services A Case of Ayub Teaching Hospital, Abbottabad - Pakistan. SERV Service QUAL QualityShan rNo ratings yet
- A Service Quality and Its Influence On Customer Satisfaction in A Multi-Speciality HospitalDocument4 pagesA Service Quality and Its Influence On Customer Satisfaction in A Multi-Speciality HospitalAr AmirNo ratings yet
- To Find Out The Relationship Between Service Quality and Customer Satisfaction in HospitalsDocument30 pagesTo Find Out The Relationship Between Service Quality and Customer Satisfaction in HospitalsAnonymous Bhnfli100% (1)
- JURNAL MutuDocument5 pagesJURNAL MutuWaras WidayatiNo ratings yet
- A Study On Patient Satisfaction Towards The Quality of Services Offered in Government Hospitals of Kanyakumari DistrictDocument11 pagesA Study On Patient Satisfaction Towards The Quality of Services Offered in Government Hospitals of Kanyakumari DistrictDr Sridevi R100% (1)
- Project ReportDocument41 pagesProject ReportAnoop PunathilNo ratings yet
- Patient Satisfaction With Access To 1malaysia Clinic: SciencedirectDocument8 pagesPatient Satisfaction With Access To 1malaysia Clinic: SciencedirectArrAryaNo ratings yet
- Pengaruh Kualitas Pelayanan Terhadap Kepuasan Pasien RawatDocument21 pagesPengaruh Kualitas Pelayanan Terhadap Kepuasan Pasien RawatFiddianNo ratings yet
- Impact - of - Hospital - Service - Quality - Dimensions - On - Customer Loyalty Final 23-12-12Document31 pagesImpact - of - Hospital - Service - Quality - Dimensions - On - Customer Loyalty Final 23-12-12badrinathNo ratings yet
- Paper Quality Assurance Di RsDocument21 pagesPaper Quality Assurance Di RsNisrinaNo ratings yet
- Lit Rev HealthcareDocument7 pagesLit Rev HealthcareIrbaz KhanNo ratings yet
- Importance Performance Analysis Matrix (Ipa Matrix) Service Quality of 22 Public Health in Padang CityDocument3 pagesImportance Performance Analysis Matrix (Ipa Matrix) Service Quality of 22 Public Health in Padang CityInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Registration 1Document4 pagesRegistration 1Gupta PrkNo ratings yet
- Mohammed Akram 7 September, 2019 MGT 5103 - Article Review ProfessorDocument5 pagesMohammed Akram 7 September, 2019 MGT 5103 - Article Review ProfessorElleNo ratings yet
- Quality of Dental Health Service in Indonesia: A Pilot Pathfinder SurveyDocument8 pagesQuality of Dental Health Service in Indonesia: A Pilot Pathfinder SurveyDimas Ahmad ZulfikarNo ratings yet
- Mary Journal of Health Management-2012Document16 pagesMary Journal of Health Management-2012Mary ThaherNo ratings yet
- Ijerph 20 01022Document17 pagesIjerph 20 01022Rehab DPUBMPsurabayaNo ratings yet
- The Influence of A Service Instrument For Measuring Patient Satisfaction in Multispecialty Teaching Hospital at OdishaDocument9 pagesThe Influence of A Service Instrument For Measuring Patient Satisfaction in Multispecialty Teaching Hospital at OdishaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- In Patient Satisfaction Survey-How Does It Help Our Health Care Delivery System (The Patient, The Health Care Giver and The Organization) ?Document10 pagesIn Patient Satisfaction Survey-How Does It Help Our Health Care Delivery System (The Patient, The Health Care Giver and The Organization) ?Pallavi PalluNo ratings yet
- Effective Communication Impacts Quality Healthcare ServicesDocument13 pagesEffective Communication Impacts Quality Healthcare Servicesمالك مناصرةNo ratings yet
- In Total With Result 1Document65 pagesIn Total With Result 1arshad khanNo ratings yet
- Effects of Hospital Service Quality On Patients Satisfaction and Behavioural Intention of Doctors and NursesDocument13 pagesEffects of Hospital Service Quality On Patients Satisfaction and Behavioural Intention of Doctors and NursesSiranjeevi SivakumarNo ratings yet
- Vijayrani Proj Titles Final2003Document10 pagesVijayrani Proj Titles Final2003sanbharasNo ratings yet
- Patient Satisfaction: A Study in General and Private Wards of A Multispecialty HospitalDocument15 pagesPatient Satisfaction: A Study in General and Private Wards of A Multispecialty HospitalAr AmirNo ratings yet
- Assessing The Quality of Dental Services Using SERVQUAL ModelDocument7 pagesAssessing The Quality of Dental Services Using SERVQUAL ModelHarari Management and Kaizen Institute (HMKI)No ratings yet
- Mapping Determinants of Healthcare Service Quality: A Systematic Literature ReviewDocument13 pagesMapping Determinants of Healthcare Service Quality: A Systematic Literature ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Factors Related to Customer Satisfaction of Medical Check-Up ServicesDocument14 pagesFactors Related to Customer Satisfaction of Medical Check-Up ServicesTaufiq HalimbatarNo ratings yet
- Satisfaction and Behavioral Intentions of Patients - A Study of Private HospitalsDocument6 pagesSatisfaction and Behavioral Intentions of Patients - A Study of Private HospitalsTJPRC PublicationsNo ratings yet
- Patient Experience of Inpatient Care and Services ReceivedDocument9 pagesPatient Experience of Inpatient Care and Services ReceivedsanjayNo ratings yet
- Patients - Quality - EvaluationDocument7 pagesPatients - Quality - EvaluationDumitru BiniucNo ratings yet
- A Study On Impact of Patient's Preferences On Service Quality of The Hospitals With Special Reference To Thanjavur District, TamilnaduDocument12 pagesA Study On Impact of Patient's Preferences On Service Quality of The Hospitals With Special Reference To Thanjavur District, TamilnaduIAEME PublicationNo ratings yet
- A Study On Patient Satisfaction Towards The Quality of Services Offered in Government Hospitals of Madurai DistrictDocument11 pagesA Study On Patient Satisfaction Towards The Quality of Services Offered in Government Hospitals of Madurai DistrictIAEME PublicationNo ratings yet
- Content ServerDocument8 pagesContent ServerClaypella MaskNo ratings yet
- Final Paper Satisfaction 2015Document18 pagesFinal Paper Satisfaction 2015Ananga ChakrabortyNo ratings yet
- ISSN No: 2456: International Open Access Journal International Open Access JournalDocument10 pagesISSN No: 2456: International Open Access Journal International Open Access JournalEditor IJTSRDNo ratings yet
- Impact of Service Quality On Patient Satisfaction A Study at Physiotherapy Unit Pku Muhammadiyah Hospital of YogyakartaDocument5 pagesImpact of Service Quality On Patient Satisfaction A Study at Physiotherapy Unit Pku Muhammadiyah Hospital of YogyakartaFahmi RizalNo ratings yet
- Joshua Ofori EssiamDocument9 pagesJoshua Ofori EssiamOfori EssiamNo ratings yet
- Service Quality Performance in HospitalDocument1 pageService Quality Performance in HospitalThirumal AzhaganNo ratings yet
- Chapter 1,2 Impact of Hospital Services On Outpatient SatisfactionDocument31 pagesChapter 1,2 Impact of Hospital Services On Outpatient SatisfactionHaseeb AhmedNo ratings yet
- Service Quality of Private HospitalDocument7 pagesService Quality of Private Hospitalgubbare86No ratings yet
- Service Quality in Hospital Care: The Development of An In-Patient QuestionnaireDocument9 pagesService Quality in Hospital Care: The Development of An In-Patient QuestionnaireBhavani B SNo ratings yet
- 30 D18 596.2 Fuad Husain Akbar2Document7 pages30 D18 596.2 Fuad Husain Akbar2khamilatusyNo ratings yet
- Patient' Satisfaction and Quality of Healthcare: Case of Hospitals in Ho Chi Minh CityDocument16 pagesPatient' Satisfaction and Quality of Healthcare: Case of Hospitals in Ho Chi Minh CityPSAKU International Journal of Interdisciplinary ResearchNo ratings yet
- Planning Based On Public PrivatDocument9 pagesPlanning Based On Public PrivatRenaldiPrimaSaputraNo ratings yet
- Muhammad Ikhwan InggrisDocument7 pagesMuhammad Ikhwan InggrisMuhammad IkhwanNo ratings yet
- Quality of Healthcare Services and Its Relationship With PatientDocument7 pagesQuality of Healthcare Services and Its Relationship With PatientBheru LalNo ratings yet
- A Roadmap For Improving Healthcare Service QualityDocument14 pagesA Roadmap For Improving Healthcare Service QualitySteve BlubaughNo ratings yet
- 197-Kajian Keratan Rentas Perb PDFDocument16 pages197-Kajian Keratan Rentas Perb PDFNisa HassanNo ratings yet
- Kelola,+05+ +JIMKES+2020+Vol+8+No+1+Mahfudhoh+EditDocument8 pagesKelola,+05+ +JIMKES+2020+Vol+8+No+1+Mahfudhoh+EditSwab IndonesiaNo ratings yet
- Service Quality Assessment in Health Care Sector: The Case of Durres Public HospitalDocument9 pagesService Quality Assessment in Health Care Sector: The Case of Durres Public HospitalIoana BoajeNo ratings yet
- Jurnal (TQS) 5Document15 pagesJurnal (TQS) 5djufri nurachmanNo ratings yet
- Jurnal Internasional 13Document9 pagesJurnal Internasional 13dinda mentari putriNo ratings yet
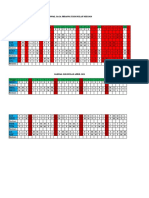
- JADWAL IGDDocument7 pagesJADWAL IGDdinda mentari putriNo ratings yet
- DeskriptifDocument71 pagesDeskriptifdinda mentari putriNo ratings yet
- Jadwal Perawat Igd Bulan Mei 2021 RevisiDocument7 pagesJadwal Perawat Igd Bulan Mei 2021 Revisidinda mentari putriNo ratings yet
- Patient-physician communication influence on loyaltyDocument5 pagesPatient-physician communication influence on loyaltydinda mentari putriNo ratings yet
- Jurnal Internasional 3Document12 pagesJurnal Internasional 3dinda mentari putriNo ratings yet
- Dimensi SERVPERF PDFDocument7 pagesDimensi SERVPERF PDFdinda mentari putriNo ratings yet
- Patient-physician communication influence on loyaltyDocument5 pagesPatient-physician communication influence on loyaltydinda mentari putriNo ratings yet
- Dimensi SERVPERF PDFDocument7 pagesDimensi SERVPERF PDFdinda mentari putriNo ratings yet
- Jurnal Internasional 12Document16 pagesJurnal Internasional 12dinda mentari putriNo ratings yet
- Jurnal Internasional 4Document9 pagesJurnal Internasional 4dinda mentari putriNo ratings yet
- Jurnal Internasional 5Document16 pagesJurnal Internasional 5dinda mentari putriNo ratings yet
- Jurnal InternasionalDocument9 pagesJurnal Internasionaldinda mentari putriNo ratings yet
- F 561Document9 pagesF 561Tarni AyuningsihNo ratings yet
- Jurnal Internasional 11Document12 pagesJurnal Internasional 11dinda mentari putriNo ratings yet
- Jurnal Internasional 9Document14 pagesJurnal Internasional 9dinda mentari putriNo ratings yet
- Jurnal Internasional 13Document9 pagesJurnal Internasional 13dinda mentari putriNo ratings yet
- Jurnal Internasional Kualitas PelayananaDocument6 pagesJurnal Internasional Kualitas Pelayananadinda mentari putriNo ratings yet
- Jurnal Internasional 14Document11 pagesJurnal Internasional 14dinda mentari putriNo ratings yet
- Jurnal Internasional 3Document12 pagesJurnal Internasional 3dinda mentari putriNo ratings yet
- Jurnal InternasionalDocument13 pagesJurnal Internasionaldinda mentari putriNo ratings yet
- Jurnal Internasional 2Document11 pagesJurnal Internasional 2dinda mentari putriNo ratings yet
- Analysis of Factors Are Relating To Service Quality and Patient Loyalty atDocument1 pageAnalysis of Factors Are Relating To Service Quality and Patient Loyalty atdinda mentari putriNo ratings yet
- Jurnal Internasional 3Document12 pagesJurnal Internasional 3dinda mentari putriNo ratings yet
- Analysis of Factors Are Relating To Service Quality and Patient Loyalty atDocument1 pageAnalysis of Factors Are Relating To Service Quality and Patient Loyalty atdinda mentari putriNo ratings yet
- Liworiz 3rd ShiftingDocument10 pagesLiworiz 3rd ShiftingKATHLEEN CALALANGNo ratings yet
- Horner Wadsworth Emmons ReactionDocument17 pagesHorner Wadsworth Emmons Reactiond1s7euu+rqc23kNo ratings yet
- Dingle National High School: Special Program in The ArtsDocument8 pagesDingle National High School: Special Program in The ArtsAngel MaeNo ratings yet
- BROAD CRESTED WEIR LABORATORY EXPERIMENTDocument12 pagesBROAD CRESTED WEIR LABORATORY EXPERIMENTSyafiq Roslan75% (4)
- January, 2021: Accuracy Check Test or Calibration of 15ppm Bilge Alarm FOCAS-1500C, FOCAS-1500EDocument2 pagesJanuary, 2021: Accuracy Check Test or Calibration of 15ppm Bilge Alarm FOCAS-1500C, FOCAS-1500Eengineer.ibrahim.miNo ratings yet
- Chemistry Thesis Infographics by SlidesgoDocument35 pagesChemistry Thesis Infographics by SlidesgobabithyNo ratings yet
- Research Design and Planning TechniquesDocument8 pagesResearch Design and Planning TechniquesAngelique BarizoNo ratings yet
- Typing Lesson KobeDocument2 pagesTyping Lesson KobeANNANo ratings yet
- Astm 3441Document6 pagesAstm 3441Todor Ivanov YankovNo ratings yet
- Informative & Explanatory Rubric SampleDocument1 pageInformative & Explanatory Rubric SampleDanielle GrayNo ratings yet
- Core Animation Enter The MatrixDocument99 pagesCore Animation Enter The MatrixtdkhoaNo ratings yet
- Kertas Trial Addmath MRSM K1 2021 SkemaDocument48 pagesKertas Trial Addmath MRSM K1 2021 SkemaRyan YongNo ratings yet
- Topic 5 DLL Elem LowerDocument4 pagesTopic 5 DLL Elem LowerLethBan100% (3)
- Making Something of A Hole in The GroundDocument7 pagesMaking Something of A Hole in The Groundcalude debussyNo ratings yet
- Bourdieu FoucaultDocument33 pagesBourdieu FoucaultChristie DanielsNo ratings yet
- National Council of Science Museums (NCSM) Block-GN, Sector-V, Bidhan Nagar Kolkata - 700 091Document8 pagesNational Council of Science Museums (NCSM) Block-GN, Sector-V, Bidhan Nagar Kolkata - 700 091saumitra_samNo ratings yet
- Problems Affecting Efficient Performance of Secretarial Functions (A Case Study of Selected Organizations and Ministries in Enugu Metropolis)Document14 pagesProblems Affecting Efficient Performance of Secretarial Functions (A Case Study of Selected Organizations and Ministries in Enugu Metropolis)johnNo ratings yet
- Caco Cell LineDocument9 pagesCaco Cell Linedonaldozc07No ratings yet
- Lecture 03 What Is ScienceDocument35 pagesLecture 03 What Is ScienceVivi AisahNo ratings yet
- Linux File System iDataAgent OverviewDocument267 pagesLinux File System iDataAgent OverviewBryan BowmanNo ratings yet
- Effective Academic Writing 1Document164 pagesEffective Academic Writing 1KYAW SOE100% (1)
- Comarch Fault ManagementDocument5 pagesComarch Fault ManagementJoaquinNo ratings yet
- XSLT Multiple Name Spaces in XML DocumentsDocument12 pagesXSLT Multiple Name Spaces in XML DocumentsFinnbarr P. MurphyNo ratings yet
- Sanjunath R Gajare Resume - Fresher Software EngineerDocument2 pagesSanjunath R Gajare Resume - Fresher Software EngineerSanju RaoNo ratings yet
- School Leadership and Management PracticesDocument114 pagesSchool Leadership and Management PracticesrandyNo ratings yet
- Surface Finish DefinitionsDocument2 pagesSurface Finish DefinitionsAntonioNo ratings yet
- Avinocs MilBusDocument2 pagesAvinocs MilBussakthisriniNo ratings yet
- Optimization Basic ConceptsDocument5 pagesOptimization Basic Conceptsjyothis_joy8315No ratings yet
- Mayer, Et Al (1996)Document10 pagesMayer, Et Al (1996)David John LemayNo ratings yet