You might also like
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
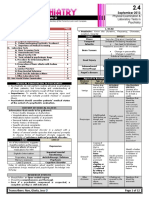
- 02.04. Physical Examination and Laboratory Tests in PsychiatryDocument12 pages02.04. Physical Examination and Laboratory Tests in PsychiatryMiguel C. DolotNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- HY Cardio - 2Document36 pagesHY Cardio - 2oopsseNo ratings yet
- Frequency DR Hulda Clark ZapperDocument45 pagesFrequency DR Hulda Clark ZapperkwbutterfliesNo ratings yet
- Approach To The Dysmorphic ChildDocument15 pagesApproach To The Dysmorphic ChildBashar KhalilNo ratings yet
- Stomach - GastritisDocument22 pagesStomach - GastritisaimanNo ratings yet
- Ujian Lokal MCQDocument23 pagesUjian Lokal MCQAnnissa Syaira100% (2)
- Criterios Beers 2019Document8 pagesCriterios Beers 2019Viki BernalNo ratings yet
- Chapter 32 Immunologic DisordersDocument12 pagesChapter 32 Immunologic DisordersStaceyNo ratings yet
- Diabetes Mellitus: DiagnosisDocument8 pagesDiabetes Mellitus: DiagnosisKelly YeowNo ratings yet
- Visayas Community Medical Center Department of Surgery: Curan, Jan Kleen Ediza, Janseen Tortugo, Andrea MarieDocument43 pagesVisayas Community Medical Center Department of Surgery: Curan, Jan Kleen Ediza, Janseen Tortugo, Andrea MarieJanseen EdizaNo ratings yet
- Aripiprazole Drug Study - Rhuby AbenojaDocument1 pageAripiprazole Drug Study - Rhuby AbenojaRHUBY ABENOJANo ratings yet
- Doppler-Atlas Stroke ManagementDocument7 pagesDoppler-Atlas Stroke ManagementdanielNo ratings yet
- Classification IHS Code 1Document4 pagesClassification IHS Code 1theresia 102018040No ratings yet
- Product Information Ultravist: 130829ultravistpi Page 1 of 1Document20 pagesProduct Information Ultravist: 130829ultravistpi Page 1 of 1Jasmeet Singh AroraNo ratings yet
- Drug StudyDocument1 pageDrug StudyMarichu BajadoNo ratings yet
- STUDY OF ILLNESS CONDITION FormatDocument2 pagesSTUDY OF ILLNESS CONDITION FormatChryst Louise SaavedraNo ratings yet
- ENT OT Supreme MergedDocument56 pagesENT OT Supreme MergedMary Rose JuanNo ratings yet
- Paracetamol (Alvedon) Acetylcysteine Fluimucil KCL (Kalium Durule)Document1 pageParacetamol (Alvedon) Acetylcysteine Fluimucil KCL (Kalium Durule)Jesse James Advincula EdjecNo ratings yet
- Clinical Biochemical Investigations For Inborn Errors of MetabolismDocument19 pagesClinical Biochemical Investigations For Inborn Errors of Metabolismzain and mariamNo ratings yet
- General Surgery II Exam PaperDocument2 pagesGeneral Surgery II Exam PaperSheikh Muhammad TabieshNo ratings yet
- Daftar Penyakit Gigi Dan MulutDocument10 pagesDaftar Penyakit Gigi Dan MulutbudiNo ratings yet
- Auntminnie SignsDocument56 pagesAuntminnie SignsHey ReelNo ratings yet
- HFA Position Papers 2019Document264 pagesHFA Position Papers 2019Irina Cabac-PogoreviciNo ratings yet
- ATI Flash Cards 10, Medications Affecting Digestion and NutritionDocument22 pagesATI Flash Cards 10, Medications Affecting Digestion and NutritionSue PadgettNo ratings yet
- Glossary of EMTDocument5 pagesGlossary of EMTErnan BaldomeroNo ratings yet
- Histology of Excretory System: OutlineDocument5 pagesHistology of Excretory System: Outlinekang seulgi can set me on fire with her gaze aloneNo ratings yet
- CREOGGYNREVIEW PP PDFDocument98 pagesCREOGGYNREVIEW PP PDFRima HajjarNo ratings yet
- Laporan Kematian NOVEMBER 2018Document8 pagesLaporan Kematian NOVEMBER 2018Rachmat KaryaNo ratings yet
- Bexarotene Induced Central HypothyroidisDocument257 pagesBexarotene Induced Central HypothyroidisAnghel Ana-MariaNo ratings yet
- Osce ped extern รวมเฉลยถึงรุ่นแปดโรสองDocument37 pagesOsce ped extern รวมเฉลยถึงรุ่นแปดโรสองNonthapat PaesarochNo ratings yet