Professional Documents
Culture Documents
Intelligence IQ Testing PDF
Uploaded by
Reynant Tayas Zapanta Jr.Original Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Intelligence IQ Testing PDF
Uploaded by
Reynant Tayas Zapanta Jr.Copyright:
Available Formats
See discussions, stats, and author profiles for this publication at: https://www.researchgate.
net/publication/6716188
Intelligence (IQ) Testing
Article in Pediatrics in Review · December 2006
DOI: 10.1542/pir.27-11-403 · Source: PubMed
CITATIONS READS
10 18,590
2 authors:
Ellen B Braaten Dennis Norman
Massachusetts General Hospital; Harvard Medical School Harvard University
36 PUBLICATIONS 1,181 CITATIONS 3 PUBLICATIONS 58 CITATIONS
SEE PROFILE SEE PROFILE
All content following this page was uploaded by Ellen B Braaten on 02 July 2014.
The user has requested enhancement of the downloaded file.
Editor-in-Chief: Lawrence F. Nazarian,
Rochester, NY
Associate Editors: Tina L. Cheng,
Baltimore, MD
Joseph A. Zenel, Portland, OR
contents
Editor, In Brief: Henry M. Adam, Bronx, NY
Consulting Editor: Janet Serwint, Baltimore, MD
Consulting Editor Online and Multimedia
PediatricsinReview姞 Vol.27 No.11 November 2006
Projects: Laura Ibsen, Portland, OR
Editor Emeritus and Founding Editor:
Robert J. Haggerty, Canandaigua, NY
Managing Editor: Luann Zanzola
Medical Copy Editor: Deborah K. Kuhlman
Articles
Editorial Assistant: Sydney Sutherland
Editorial Office: Department of Pediatrics
University of Rochester
403 Intelligence (IQ) Testing
School of Medicine & Dentistry Ellen B. Braaten, Dennis Norman
601 Elmwood Avenue, Box 777
Rochester, NY 14642
sydney_sutherland@urmc.rochester.edu
Editorial Board
409 Breastfeeding: The Essential Principles
Margie Andreae, Ann Arbor, MI Latha Chandran, Polina Gelfer
Richard Antaya, New Haven, CT
Laurence A. Boxer, Ann Arbor, MI
Consultation With the Specialist:
Latha Chandran, Stony Brook, NY
Howard Eigen, Indianapolis, IN
Leonard Feld, Charlotte, NC
Jeremy N. Friedman, Toronto, ON
418 Cardiovascular Preparticipation Sports Screening
Anoop Singh, Michael Silberbach
Vincent A. Fulginiti,Tucson, AZ
Mark Goldstein, Boston, MA
Russell J. Hopp, Omaha, NE
Peter Hoyer, Essen, Germany
Hal B. Jenson, Springfield, MA
425 Index of Suspicion
Chris P. Johnson, San Antonio, TX Katie E. McPeak, Abel Guerra, Christine Nefcy, Mark LaShell,
J. Jeffrey Malatack, Narberth, PA Michael Wolf, Sibel Algon
John Pascoe, Dayton, OH
DeWayne Pursley, Boston, MA
Matthew D. Sadof, Springfield, MA
Bennett A. Shaywitz, New Haven, CT
Michael Silberbach, Portland, OR
Technical Tip
Mark L. Silen, Portland, OR
David L. Skaggs, Los Angeles, CA
Nancy Spector, Philadelphia, PA
Dan Thomas, Los Angeles, CA
433 Corneal Abrasions
Ann U. Stout
Surendra K. Varma, Lubbock, TX
Publisher: American Academy of Pediatrics
Robert Perelman, Associate Executive Director
for Education In Brief
Pediatrics in Review姞
(ISSN 0191-9601) is owned and controlled by
the American Academy of Pediatrics. It is
published monthly by the American Academy of
434 Ampicillin and Amoxicillin
Pediatrics, 141 Northwest Point Blvd, Elk Grove
Village, IL 60007-1098
Statements and opinions expressed in Pediatrics
in Review威 are those of the authors and not
necessarily those of the American Academy of
436 Cocaine
Pediatrics or its Committees. Recommendations
included in this publication do not indicate an
exclusive course of treatment or serve as a
standard of medical care.
Subscription price for 2006: AAP Fellow $154;
Internet-Only Articles
AAP Candidate Fellow $144; Nonmember
$194; Allied Health or Resident $144.
Abstracts appear on page 432.
Institutions call for pricing (866-843-2271). For
overseas delivery, add $75. Current single issue
Visual Diagnosis:
price is $10 domestic, $12 international.
Replacement issues must be claimed within 6
months from the date of issue and are limited to
three per calendar year.
e71 A Child Who Has
Acute Onset of Unusual Skin Lesions and Edema
Periodicals postage paid at ARLINGTON Ceyda Acun, Gonca Ustundag, Ayhan Sogut, Rafet Koca,
HEIGHTS, ILLINOIS and at additional mailing Gamze Numanoglu
offices.
© AMERICAN ACADEMY OF PEDIATRICS,
2006. All rights reserved. Printed in USA. No
part may be duplicated or reproduced without Commentary: The Value of the ECG in the
permission of the American Academy of
Pediatrics. POSTMASTER: Send address
changes to PEDIATRICS IN
REVIEW威, American Academy
of Pediatrics, 141 Northwest
e75 Preparticipation Sports Physical Examination:
The Italian Experience
Renato Vitiello
Point Blvd., Elk Grove Village,
IL 60007-1098.
The printing and production of
Pediatrics in Review威 is made
possible, in part, by an
educational grant from Ross
Products Division, Abbott
Laboratories.
Cover: The artwork on the cover of this month’s issue
is by one of the winners of our 2005 Cover Art
Contest, 12-year-old Talia Niederman of North Ber-
Answer Key: 1. E; 2. A; 3. C; 4. E; 5. D; 6. D; 7. A; gen, NJ. Talia’s pediatrician is Alyssa Zenack, MD.
8. E; 9. C; 10. D; 11. C; 12. A; 13. B; 14. D; 15. C; 16. E;
17. A
Article cognition, language, learning
Intelligence (IQ) Testing
Ellen B. Braaten, PhD,*
Objectives After completing this article, readers should be able to:
Dennis Norman, EdD†
1. Define intelligence quotient (IQ) and what constitutes the “normal” range of IQ scores.
2. Describe the predictive validity of intelligence test scores.
Author Disclosure 3. Discuss the factors that may influence performance on intelligence tests.
Drs Braaten and 4. Recognize the relationship between variability observed in factor scores and the
Norman did not probability of the child having a learning or cognitive disability.
disclose any financial 5. Describe how achievement tests are used in conjunction with IQ tests to determine
relationships relevant eligibility for a learning disability.
to this article.
Introduction
Intelligence tests assess a person’s mental abilities and compare them with the abilities of
other people through the use of numerical scores. Although the term intelligence is used
as if there is agreement on what it means, in reality there is much debate as to how this term
should be and has been defined. For example, debate has surrounded whether intelligence
should be considered an inherent cognitive capacity, an achieved level of performance, or
a qualitative construct that cannot be measured. Psychologists have debated whether
intelligence is learned or inherited, culturally specific or universal, and one ability or several
abilities. While these debates are ongoing, evidence is increasing that traditional intelli-
gence tests measure specific forms of cognitive ability that are predictive of school
functioning, but do not measure the many forms of intelligence that are beyond these
more specific skills, such as music, art, and interpersonal and intrapersonal abilities. (1)
Despite these debates, most experts view intelligence as a person’s problem-solving
abilities, such as adapting to the environment and having vocabulary skills, higher-order
thinking (eg, decision making, reasoning skills, verbal and nonverbal problem-solving
skills), memory, and mental speed. More specifically, for the purpose of this article,
intelligence is discussed as it relates to a child’s score on the intelligence (IQ or “intelli-
gence quotient”) tests that are used most commonly to measure a person’s intelligence for
educational planning or neuropsychological assessment.
Intelligence Tests
Efforts to measure intelligence have long been a part of psychology, and despite contro-
versy over the meaning and scope of intelligence, an IQ score can provide meaningful data
about a child’s cognitive abilities if put within a conceptual framework that does not
overstate its meaning or implications for the child. Intelligence tests are the most studied
and, consequently, the most reliable, valid, and useful tests available for measuring specific
cognitive abilities. Within a particular IQ test, children tend to perform the same on items
designed to assess the same ability, which suggests internal consistency. The tests are
reliable because children generally receive the same score when they retake the same test
years later, although the reliability of the test usually increases with the age of the child.
Test validity is based on numerous studies that have found high correlations between
children’s IQ scores and their performance in school, achievement tests, and tests of
specific intellectual functioning (eg, measures of language, visual motor processing).
An IQ score reflects a child’s performance on an intelligence test relative to that of
children of the same age. In short, a child’s IQ score tells the extent to which his or her
*Psychologist, Massachusetts General Hospital; Assistant Professor, Harvard Medical School, Boston, Mass.
†
Chief of Psychology, Massachusetts General Hospital; Associate Professor, Harvard Medical School, Boston, Mass.
Pediatrics in Review Vol.27 No.11 November 2006 403
cognition, language, learning IQ testing
test children ages 21⁄2 to 6 years of
age. Each of these tests is composed
of subtests that measure a variety of
domains. The WISC-IV contains
15 subtests that are divided into 10
core subtests and 5 supplemental
(ie, optional) subtests, which form
four composites scales (referred to
as “factor scores”): Verbal Com-
prehension (verbal knowledge and
the ability to use verbal skills in new
situations), Perceptual Organiza-
tion (the ability to think about and
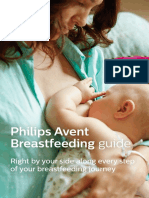
Figure. Classification ratings for IQ ranges as they are distributed along the normal curve. organize visual material without the
use of words), Working Memory
performance on the test departs from average. The IQ (the ability to hold information in memory to manipulate
score represents a construct of “intelligence” that in- it or perform calculations with it), and Processing Speed
cludes a combination of verbal and nonverbal processing (the speed at which one can process simple visual infor-
skills, such as vocabulary, information about the world, mation without making errors). The Table lists the
reasoning, short-term memory, and speed of information WISC-IV subtests and factor scores. Although there are
processing; these skills, together, are represented by the tests of infant “intelligence,” such as the Bayley Scales of
IQ score. Nearly all comprehensive psychological evalu- Infant Development, most tests for children younger
ations include some measure of intelligence. For exam- than age 3 years measure abilities, such as sensorimotor
ple, for a child who is being tested to confirm a diagnosis development and early language skills, which are not
of attention-deficit/hyperactivity disorder (ADHD), an highly correlated with later IQ.
intelligence test can confirm that the child’s academic
difficulties do not indicate a specific cognitive weakness Predictive Validity of IQ
or mild mental retardation. Intelligence tests are reasonably accurate at predicting
Most intelligence tests assess a range of verbal, visual- which children will be successful in school and which will
spatial, and problem-solving skills. Because they target
multiple cognitive skills, IQ tests are composed of
subtests that measure specific areas of functioning. Scores WISC-IV Factors and
Table.
on these subtests are combined to yield measures of Subtests
verbal and nonverbal problem-solving abilities, as well as
a full-scale IQ score. IQ scores are assumed to be nor- Verbal Comprehension Factor
mally distributed in the population, with most scores ● Three Core Subtests: Similarities—Vocabulary—
falling in the middle of the distribution and fewer scores Comprehension
● Two Supplemental Subtests: Information—Word
falling at the upper and lower extremes (Figure). The
Reasoning
average IQ score on most IQ tests is 100, with a standard
deviation of 15. Most IQ scores (about 68%) fall within 1 Perceptual Reasoning Factor
standard deviation on either side of the mean (eg, be- ● Three Core Subtests: Block Design—Picture
tween 85 and 115), and almost all scores (99% of popu- Concepts—Matrix Reasoning
lation) fall within 3 standard deviations above or below ● One Supplemental Subtest: Picture Completion
the mean. Working Memory Factor
School-age children most frequently are tested with ● Two Core Subtests: Digit Span—Letter-Number
the Wechsler Intelligence Scale for Children–Fourth Sequencing
Edition (WISC-IV). The Wechsler Adult Intelligence ● One Supplemental Subtest: Arithmetic
Scale, Third Edition (WAIS-III) is the test used most Processing Speed Factor
frequently for adolescents ages 16 and older. The
● Two Core Subtests: Coding—Symbol Search
Wechsler Preschool and Primary Scale of Intelligence – ● One Optional Subtest: Cancellation
Third Edition (WPPSI-III) is used most frequently to
404 Pediatrics in Review Vol.27 No.11 November 2006
cognition, language, learning IQ testing
have difficulty, with correlations between intelligence education, an enriched language environment, good
tests and measures of educational achievement averaging school attendance, good schools, and stable neighbor-
about 0.50. Thus, IQ tests are one of the best single hoods. (4)
indices of how well a child will do in school. However, Cultural and ethnic differences in performance on
IQ test scores are not the sole predictive factor of how a intelligence tests also have been documented. For exam-
person will perform in school and are not the definitive ple, studies have indicated that the average scores on
indication of how a person eventually will function in standardized intelligence tests of children from African-
society because other variables, such as intellectual do- American and Latino families often are below those of
mains not measured by a specific test, parenting, quality children from Caucasian families. However, the available
of schooling, motivation, and exposure to culture and data do not support a genetic interpretation; (5) rather,
books, also are important determinants of success in life. the differences likely reflect a cultural or language bias.
Research has shown that IQ constancy increases with In addition to innate and background factors, an
age, although correlations tend to be slightly higher for almost limitless list of intervening variables can affect a
elementary students than for high school or college child’s performance on an IQ test. A qualified test ad-
students. Generally, the correlations with educational ministrator attempts to minimize such variables as much
achievement and IQ are highest for verbal subjects, such as possible, but influencing factors can include the loca-
as reading. In contrast, the predictive power of IQ test tion of the evaluation (eg, noisy office), previous testing
scores before the first birthday are not very strong for experiences that may result in practice effects, the
children who fall in the average to superior range, (2) but examiner-examinee interaction, a negative stance on the
the tests are fairly predictive (ranging in studies from part of the child, peer-group pressure to fail, or poor
0.50 to 0.97) for children assessed
at lower IQ levels (ie, below IQs
.result. .in.largemany
of 50). (3)
Overall, the general rule of
thumb is that the older the child,
the more stable the IQ. By age 4
learning disabilities
years, the correlation with IQ 12 verbal-performance splits on
years later is relatively high
(r⫽0.77). (2) Although many
IQ tests.
older children show little fluctua-
tion in their IQ scores, research
has indicated that a subset of younger children show wide motivation. Other causes of poor performance can in-
fluctuation in IQ scores. Finally, even older children may clude limited hearing or visual acuity, a lack of profi-
show some fluctuations in scores in response to major ciency with the English language, situational stressors,
stressors such as a loss of a parent, divorce, or change in poor attentional skills, or acute emotional difficulties
schools. With these possible exceptions, by around age such as depression or anxiety.
10 years, IQ scores generally are relatively stable.
Discrepancies in IQ Test Score Patterns
Factors That Influence Performance on IQ In general, children’s factor scores on the WISC-IV
Tests should be fairly similar; the more variability observed in
IQ is influenced by genetic factors (eg, the child’s genetic factor scores, the higher the probability that the child has
makeup), familial factors (eg, parents’ IQs and education a learning or cognitive disability. Previous versions of the
and quality of the home environment), educational fac- WISC provided verbal and performance IQ scores in
tors (eg, quality of educational opportunities and teach- addition to a full-scale IQ. Differences greater than 15
ing), and other factors, such as the community in which points between a child’s verbal comprehension and per-
the child lives. Environmental influences on the develop- ceptual reasoning scores are worthy of an explanation
ment of intelligence include access to stimulating or and may be cause for concern because many learning
enriching experiences, caregivers who help the child disabilities result in large verbal-performance splits on IQ
learn problem-solving skills, access to books and sources tests. For example, many children who have dyslexia have
of knowledge, good nutrition, a high level of social lower verbal abilities compared with nonverbal abilities
support, parental involvement in the child’s learning and because dyslexia is a verbally based learning disability.
Pediatrics in Review Vol.27 No.11 November 2006 405
cognition, language, learning IQ testing
Children who have nonverbal learning disabilities, by objective standard. When used to diagnose a specific
definition, have lower perceptual reasoning scores com- learning disability, a child’s academic achievement in one
pared with verbal comprehension abilities and frequently or more areas is compared with his or her intellectual
have significantly weak processing speed scores, as well. abilities. If a child’s ability in one or more areas of
However, even a 15-point difference does not necessarily achievement, as measured on standardized tests, is sig-
indicate the presence of a learning disability. This is nificantly lower than expectations based on age, educa-
because differences in styles of thinking and learning are tion, and intelligence, the probability is high that a
common and often are reflected in a child’s pattern of IQ learning disability exists. However, these difficulties also
scores, such as in the case of a child who has superior must impede the child’s ability in academic achievement
intellect and has a verbal comprehension index of or activities of daily living. Also, if the child has a sensory
140 and a perceptual reasoning index of 120. That said, deficit, such as in visual perception, memory, or atten-
if an extremely large (⬎25-point) verbal comprehension- tion, the difficulties in math or writing need to be worse
perceptual reasoning split is present, and if one of these than what would be expected with the sensory deficit
scores is below the average range, psychologists fre- alone. For example, if a child who has ADHD has prob-
quently refer the child to a neurologist or to a develop- lems with math, the math difficulties must be worse than
mental pediatrician to rule out the possibility of neuro- what would be expected from a child who has attentional
logic impairment. Even if the difference between a child’s difficulties. Thus, although IQ and achievement tests are
factor scores on an IQ test is large, the discrepancy used frequently to diagnose a learning disability, a simple
should not be used alone to make a diagnosis of a discrepancy is not sufficient to make the diagnosis be-
learning disability or to predict brain functioning with- cause other issues need to be eliminated.
In addition, the lack of a dis-
crepancy is not necessarily an indi-
Comparisons
cation that a learning disability
does not exist. This is particularly
of IQs with tests true for the young child who may
exhibit early signs of a learning
of academic achievement frequently are used disability, but who does not yet
in diagnosing specific learning disabilities. lag behind to the extent that a
discrepancy exists. In these cases,
the pattern of scores on relevant
tests (eg, reading fluency, phonics
out substantial support from other test data and obser- skills, reading comprehension, prereading skills) be-
vations. Finally, when the differences between a child’s comes primary in the diagnosis of a learning disability.
WISC-IV factor scores are significant, the full-scale IQ Because current federal law recognizes the shortcomings
may not be a valid measure of the child’s level of overall of a discrepancy approach in determining a learning
intellectual functioning because the IQ may represent a disability, school districts are not bound by the discrep-
forced “average” of very disparate skills. ancy criteria before children are found to be eligible for
special education services. However, current law also
Using Intelligence Tests to Evaluate Learning states that the lack of achievement must not be due to
Disabilities mental retardation; a visual, hearing, or motor impair-
To evaluate specific learning disabilities, such as a reading ment; emotional disturbance; or environmental disad-
disorder, disorder of written expression, or math disabil- vantage. Thus, intelligence tests typically are given to
ity, IQ tests typically are used in conjunction with rule out the possibility that a cognitive deficit underlies
achievement tests. Achievement tests are designed to the child’s difficulties with academic skills.
measure what a child has actually learned, including
mathematical problem-solving, reading, spelling, writ- Summary
ing, or an understanding of science concepts. Most Intelligence is a multifaceted construct that, for the
achievement tests focus on a particular subject and mea- purposes of this review, is operationalized as the standard
sure a child’s learning with questions of varying difficulty. IQ tests (eg, Wechsler Scales) used by schools and psy-
The child’s score then either is compared with that of a chologists to measure cognitive functioning in a formal
child of the same age or grade or measured against an environment. Intelligence scores predict the ease with
406 Pediatrics in Review Vol.27 No.11 November 2006
cognition, language, learning IQ testing
which people learn in formal situations, but do not Detterman D, ed. Current Topics in Human Intelligence: Vol. 5. The
necessarily predict success in life or occupations. Mea- Environment. Norwood, NJ: Ablex; 1996:173–177
5. Brooks-Gunn J, Klebanov PK, Duncan GJ. Ethnic differences in
sures of intelligence can be affected by fluency of lan-
children’s intelligence test scores: role of economic deprivation,
guage, access to educational stimulation, educational home environment, and maternal characteristics. Child Devel.
resources, motivation, and emotional functioning. Vari- 1996;67:396 – 408
ability in terms of subtest or factor score performance
may be a sign of a learning disability, but a simple
discrepancy between verbal and nonverbal abilities is not Suggested Reading
sufficient to diagnose a learning disability. Comparisons Braaten E, Felopulos G. Straight Talk About Psychological Testing
of IQs with tests of academic achievement frequently are for Kids. New York, NY: The Guilford Press; 2004
used in diagnosing specific learning disabilities, but Flanagan DP, Kaufman AS. Essentials of WISC-IV Assessment. New
schools and diagnosticians are not bound by the discrep- York, NY: John Wiley & Sons; 2004
Hebben N, Milberg W. Essentials of Neuropsychological Assessment.
ancy criteria. However, to diagnosis a specific learning
New York, NY: John Wiley & Sons; 2002
disability, the possibility of a cognitive deficit needs to be Lezak MD, Howieson DB, Loring DW, Hannay HJ, Fischer JS.
ruled out, which typically is done through the adminis- Neuropsychological Assessment. 4th ed. Oxford, England: Oxford
tration of an IQ test. Overall, IQ tests are the most University Press; 2004
reliable and valid instruments used to measure a person’s Obrzut JE, Hynd GW. Neuropsychological Foundations of Learning
cognitive abilities, but they always should be interpreted Disabilities: A Handbook of Issues, Methods and Practice. San
Diego, Calif: Academic Press; 1996
within a conceptual framework that does not overstate its
Snyder PJ, Nussbaum PD. Clinical Neuropsychology: A Pocket
implications for the child. Handbook for Assessment. Washington, DC: American Psycho-
logical Association; 1998
Spreen O, Strauss E. A Compendium of Neuropsychological Tests:
References Administration, Norms and Commentary. Oxford, England:
1. Gardner H. Frames of Mind: The Theory of Multiple Intelligences. Oxford University Press; 1998
New York, NY: Basic Books; 1983 Wechsler D. Manual for the Wechsler Intelligence Scale for
2. Neisser U, Boodoo G, Bouchard TJ Jr, Boykin AW, Brody N, Ceci Children–Revised. New York, NY: The Psychological Corpora-
SJ. Intelligence: knowns and unknowns. Am Psychol. 1996;51:77–101 tion; 1974
3. Satler JM. Assessment of Children: Behavioral and Clinical Applica- Wechsler D. WAIS-R Manual: Wechsler Adult Intelligence
tions. 4th ed. La Mesa, Calif: Jerome M. Sattler, Publisher, Inc; 2002 Scale–Revised. New York, NY: The Psychological Corporation;
4. Spitz HH. Commentary on the contributions to this volume. In: 1981
Pediatrics in Review Vol.27 No.11 November 2006 407
cognition, language, learning IQ testing
PIR Quiz
Quiz also available online at www.pedsinreview.org.
1. Intelligence, as measured by IQ testing, is:
A. Independent of cultural background.
B. Invariant over time.
C. Non-normally distributed.
D. Not assessable in children younger than age 6 years.
E. Predictive of school performance.
2. An 8-year-old boy is being evaluated for his poor academic performance in third grade. Results from his
WISC-IV reveal:
Full Scale IQ: 100
Verbal Comprehension Factor Score: 85
Perceptual Reasoning Factor Score: 115
Working Memory Factor Score: 95
Processing Speed Factor Score: 105
These test findings are most consistent with a diagnosis of:
A. Dyslexia.
B. Expected variation.
C. Isolated attention-deficit disorder.
D. Math disability.
E. Mental retardation.
3. A 6-year-old girl whose teachers are concerned about her ability to keep up with her classmates is found
to have a WISC-IV IQ of 70 with a verbal comprehension factor score of 65 and a perceptual reasoning
factor score of 75. These results are most supportive of a diagnosis of:
A. Average intelligence.
B. Dyslexia.
C. General cognitive deficit.
D. Isolated attention-deficit disorder.
E. Isolated nonverbal learning disability.
4. An 8-year-old boy without evidence of sensory deficit is having difficulty reading at grade level. In
addition to a significant verbal-performance split on IQ testing, formal diagnosis of a reading disorder
requires:
A. A full-scale IQ of at least 110.
B. A home visit.
C. Grade retention.
D. Neurologic referral.
E. Standardized achievement testing.
408 Pediatrics in Review Vol.27 No.11 November 2006
Article nutrition
Breastfeeding: The Essential Principles
Latha Chandran, MBBS,
Objectives After completing this article, readers should be able to:
MPH,* Polina Gelfer, MD†
1. Understand the physiology of lactation.
2. Discuss the biologic specificity of human milk.
Author Disclosure 3. Delineate the benefits of breastfeeding for the infant, the mother, and the community.
Drs Chandran and 4. Know relative and absolute contraindications to breastfeeding.
Gelfer did not 5. Describe current recommendations for breastfeeding.
disclose any financial
relationships relevant
to this article. Introduction
Breastfeeding practice is the biologic norm for Homo sapiens and dates back some 40,000
years. Until the last several decades, breastfeeding was the norm, and wet-nursing was the
only alternative to allow infants to survive. Although pediatricians overwhelmingly agree
that breastfeeding is best for babies, in the United States today, only 68% of all new
mothers even attempt it, and at least 50% abandon it quickly. The United States Public
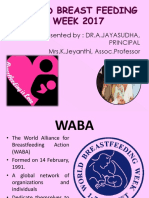
Health Service Healthy People 2010 Initiative calls for an increase in the rate of breast-
feeding to 75% at birth, 50% at age 6 months, and 25% at 1 year of age (Figure). The
presence or absence of breastfeeding affects the economics of the family and the commu-
nity. Multiple studies confirm that the annual cost to the United States health care system
from women not breastfeeding is several billion dollars. Promoting breastfeeding can
decrease costs for public health programs such as The Special Supplemental Nutrition
Program for Women, Infants, and Children, parental employee absenteeism as a result of
decreased infant illness, environmental burden for disposal of formula cans and bottles, and
energy demands for production and transport of artificial feeding products.
Physiology of Lactation
During pregnancy, the breast grows larger, the diameter of the areola increases, pigmen-
tation increases, the nipples become more erect, and the veins become more prominent.
Various hormones stimulate breast growth: prolactin and placental lactogen stimulate
nipple and areolar growth; estrogen facilitates the proliferation and differentiation of the
ductal system; and progesterone promotes an increase in size of the lobes, lobules, and
alveoli. During the first half of pregnancy, the ductal tree grows and proliferates, and
additional lobules form. The second half of pregnancy is characterized by acceleration of
secretory activity and distention of alveoli from accumulating colostrum. After 16 weeks of
pregnancy, lactation occurs, even if the pregnancy does not progress.
The volume of milk secreted by the mammary cells remains small until after the infant
is born. After delivery of the placenta, serum progesterone and estrogen concentrations
fall, and negative feedback by these hormones on pituitary prolactin release is lost.
Prolactin concentrations rise, leading to increased milk synthesis. When the neonate begins
suckling, the posterior pituitary hormone oxytocin is released. Oxytocin causes the
milk-ejection reflex or letdown, a contraction of the myoepithelial cells surrounding the
alveoli necessary for the ejection of milk.
The rate of milk synthesis after each breastfeeding episode varies and is related to the
degree of emptiness or fullness of the breast; an emptier breast makes milk faster than a
fuller one. Thus, breastfeeding is not a major factor for the initiation of lactation, but it is
essential for the continuation of lactation. Lactogenesis also is susceptible to outside
*Editorial Board.
†
Assistant Professor of Clinical Pediatrics, State University of New York at Stony Brook, Stony Brook, NY.
Pediatrics in Review Vol.27 No.11 November 2006 409
nutrition breastfeeding
tablishment of Lactobacillus bifidus flora in the infant’s
gut.
Mature Milk
Mature human milk contains fat, carbohydrates, and
protein as substrates for infant nutrition. The fat of
human milk provides about 50% of its calories. Triglyc-
erides are the primary constituents of the fat. The lipid
fraction provides essential fatty acids. Human milk is
rich in long-chain polyunsaturated fatty acids, including
docosahexanoic acid and arachidonic acid, which are
associated with higher visual acuity and cognitive ability
in the infant. The fats of human milk and cow milk are
qualitatively different, with human milk containing more
of the absorbable triglyceride olein and cow milk con-
taining more volatile fatty acids (butyric, capric, caproic,
Figure. Breastfeeding rates in 2003 and United States and caprylic). These differences may result in the preterm
Healthy People 2010 breastfeeding objectives. From Centers or sick infant possibly developing steatorrhea after in-
for Disease Control and Prevention breastfeeding national gesting cow milk.
immunization data.
Lactose is the primary carbohydrate in human milk,
although small quantities of galactose and fructose also
are present. Lactose enhances calcium absorption and is
influence. Certain conditions, such as type 1 diabetes metabolized readily to galactose and glucose, which sup-
mellitus, obesity, polycystic ovary syndrome, placental ply energy to the infant. Human milk consists predomi-
retention, and stress, can delay or diminish lactogenesis. nantly of whey proteins; cow milk mostly has casein.
The reasons for this delay are not clear. Human milk Whey protein is composed of five major components:
production is related to an infant’s demand. Infants have alpha-lactalbumin, serum albumin, lactoferrin, immuno-
the ability to self-regulate their milk intake. globulins, and lysozyme. The latter three elements play
important roles in immunologic defense. Human milk
Composition of Human Milk also contains free amino acids, including essential amino
Human milk is unique and species-specific. All substitute acids, as well as nucleotides. Table 1 lists comparisons
feeding preparations differ markedly from it, making between human milk, cow milk, and some infant formu-
human milk superior for infant feeding. Human milk is las. About one third of infants who are allergic to cow
rich in proteins, nonprotein nitrogen compounds, lipids, milk protein may be allergic to soy protein, as well; in
oligosaccharides, vitamins, and minerals. In addition, it such cases, protein hydrolysate formulas are used. The
contains hormones, enzymes, growth factors, and many standard caloric content for all formulas is 20 kcal/oz.
types of protective agents. The amount of vitamins and micronutrients in human
milk varies, depending on the diet and genetic differ-
Colostrum ences of mothers. Generally, as lactation progresses, the
The first milk secreted by the postpartum woman is level of water-soluble vitamins in human milk increases
colostrum. Human colostrum differs from mature milk. and the level of fat-soluble vitamins declines. Human
The energy value is about 67 kcal/100 mL compared milk is a good source of vitamin A and vitamin E, but has
with the 75 kcal/100 mL for mature milk. The volume very little fat-soluble vitamin D. The risk of vitamin D
varies with the parity of the mother and the number of deficiency rickets is greatest for dark-skinned children
feedings. The concentrations of sodium, potassium, and living in inner-city areas and for infants of solely breast-
chloride are greater than those of mature milk. Protein, feeding mothers eating strict vegetarian diets. All breast-
fat-soluble vitamins, and minerals are present in greater fed infants should receive 200 IU of oral vitamin D drops
percentages than in transitional and mature milk. The daily. (1)
high level of antibodies may provide protection against Human milk contains small amounts of vitamin K.
the bacteria and viruses that are present in the birth canal. A few days after birth, enteric bacteria produce sufficient
Colostrum facilitates the passage of meconium and es- quantities of the vitamin, but until ingestion of copious
410 Pediatrics in Review Vol.27 No.11 November 2006
Table 1. Composition of Human Milk, Cow Milk, and Infant Formulas
Cow Milk
Protein-based Soy Protein-based
Ingredients Human Milk Cow Milk Formula Formula Protein Hydrolysate Formula
Carbohydrate Lactose Lactose Lactose Sucrose Sucrose
(g/dL) 7.0 4.8 Corn syrup Corn syrup Corn syrup
3.6 to 3.7 3.6 3.4 to 3.7
Protein Human milk protein, Cow milk protein, whey: Nonfat milk Soy isolate Cow milk protein hydrolyzed
(g/dL) whey: casein ratio casein ratio of 22:78 Demineralized Methionine to reduce allergenicity
of 75:25 Total: 3.3 whey 1.8 to 2.0 1.9
Total: 1.1 1.4
Fat (g/dL) Human milk fat Butterfat Soy oil Palm olein Medium-chain triglyceride
Contains more Contains more volatile Coconut oil Soy oil oil
absorbable fatty acids Palm oil Coconut oil Soy oil
triglyceride 3.7 3.6 to 3.7 3.6 to 3.7 Coconut oil
3.8 3.4 to 3.7
Calcium 280 1,226 530 710 640 to 710
(mg/L) Higher calcium content
due to inhibition of
absorption by
phytates
Phosphorus 147 956 284 to 360 507 to 560 430 to 507
(mg/L)
Iron (mg/L) Vitamin C and 0.5 5.0 12 12
lactose facilitate
absorption
0.4
Suggested Preferred for all Children older than 1 Infants who Infants who have cow Infants who have food
uses infants year of age who have have milk allergy (30% allergies or underlying
normal gastrointestinal normal may have cross- gastrointestinal damage
tract gastrointestinal reactivity), lactose
tract but malabsorption,
cannot be galactosemia
breastfed
nutrition
breastfeeding
Pediatrics in Review Vol.27 No.11 November 2006 411
nutrition breastfeeding
Major Protective and Anti-inflammatory
Table 2. IQ scores nearly 4 points higher
than those who did not receive hu-
Factors in Human Milk man milk, after statistical control of
social and perinatal factors associ-
Factors Function
ated with breastfeeding such as
Immunoglobulins Generate immune response to specific antigens birthweight, multiplicity, gesta-
Secretory IgA, IgM, IgG tional age, maternal age, education,
Lactoferrin Antibacterial effect, especially against Escherichia
coli, inhibition of complement, carries iron and family income. (2)
Lysozyme Bactericidal and anti-inflammatory
Casein Inhibits microbial adhesion to mucosal membranes Anti-infective Properties of
Lipids Protect against enveloped viruses, anti-infective Human Milk
efforts Human milk provides protection
Prostaglandins Cytoprotective
Cytokines Activate the immune system against disease. The high concen-
Glycoconjugates Antiviral, antibacterial protection trations of secretory immunoglob-
Phagocytes Absorb pathogens, release IgA ulin (Ig)A, enzymes, other Igs, and
Lymphocytes Essential for cell-mediated immunity; antiviral leukocytes provide broad-spectrum
activity protection against infections and
Memory T cells give long-term protection
Prolactin Enhances development of B and T lymphocytes chronic conditions. Breastfeeding
Stimulates proliferation of intestinal mucosa helps to prevent infantile diarrhea
Human growth factors Mucosal barrier to antigens and other GI infections. It is now
well established that ingested anti-
bodies from human milk can pro-
amounts of human milk promotes gastrointestinal (GI) vide local GI immunity against specific enteric patho-
bacterial colonization, neonates are susceptible to vita- gens, including Campylobacter jejuni, Clostridium
min K deficiency-induced hemorrhagic disease. To pre- difficile, Escherichia coli, Giardia lamblia, rotavirus, Sal-
vent this condition, 1 mg of vitamin K is administered monella typhimurium, Shigella sp, and Vibrio cholerae.
routinely intramuscularly to infants immediately after The degree of protection is related to the amount of
birth. Mothers consuming strictly vegan diets may pro- human milk an infant receives; exclusive breastfeeding is
duce milk that is deficient in vitamin B12, as well. The associated with greater protection.
total mineral content in human milk is higher in the first Studies of the protective effects of breastfeeding
days after birth and slowly decreases throughout lacta- against respiratory tract infections offer conflicting re-
tion. Although human milk has only a small amount of sults. Several studies suggest that breastfeeding helps to
iron, breastfed babies rarely develop iron deficiency be- prevent respiratory illnesses; (3) others indicate little
cause iron absorption is facilitated by the high lactose and protection. There is, however, strong evidence that hu-
vitamin C concentrations of human milk. man milk protects against respiratory syncytial virus in-
Several anti-inflammatory and protective factors have fection. (4) Similar protection has been established
been identified in human milk and their functions delin- against Haemophilus influenzae bacteremia and menin-
eated (Table 2). gitis as well as pneumonia caused by Streptococcus pneu-
moniae. Breastfeeding also provides protection against
Benefits of Breastfeeding ear infections and atopic disorders.
Child Health Benefits
Human milk provides optimal nutrition to the infant,
facilitating adequate growth and development. Research Protection from Chronic Disease
studies among term and preterm infants have shown Breastfeeding contributes to the prevention of diabetes,
significant improvements in developmental outcomes of celiac disease, childhood cancer, sudden infant death
breastfed infants compared with formula-fed infants. In syndrome, obesity, and many other health problems.
addition, growing evidence suggests small, but signifi- The longer the duration of breastfeeding, the greater is
cant, cognitive benefits for breastfeeding. When tested at its protective effect. The protection by human milk
7 to 8 years of age, children who were breastfed as infants against illness extends beyond infancy to childhood and
for 8 months or longer had mean verbal intelligence adulthood. Exclusive breastfeeding during the first
quotient (IQ) scores 6 points higher and performance months after birth is associated with lower asthma rates
412 Pediatrics in Review Vol.27 No.11 November 2006
nutrition breastfeeding
during childhood. (5) Human milk Viruses Identified in Breast Milk and
Table 3.
also may protect preterm infants
against necrotizing enterocolitis. Impact on Breastfeeding
Virus Impact on Breastfeeding
Benefits for the Mother
Breastfeeding and lactation de- HIV-1, HIV-2 Contraindicated
crease postpartum bleeding and HTLV-1, HTLV-2 Contraindicated
Hepatitis B virus (HBV) Not contraindicated, especially if infant receives HBV
promote more rapid uterine involu- vaccine and HBV immune globulin
tion. They decrease the risk of Hepatitis C virus Not contraindicated. Nipple cracks or fissures may pose
breast and ovarian cancer and pos- a risk for transmission.
sibly decrease the risk of hip frac- Herpes simplex virus Contraindicated only if active breast lesions are present
tures and osteoporosis in the post- Cytomegalovirus Not contraindicated. Some experts recommend stopping
breastfeeding of preterm and immunosuppressed
menopausal period. They definitely infants if mother becomes infected during lactation.
promote development of bonding Rubella virus Not contraindicated
and attachment between the West Nile virus Not contraindicated
mother and the infant. HIV⫽human immunodeficiency virus, HTLV⫽human T-cell lymphoma/leukemia virus
Contraindications to
Breastfeeding
Medical Disorders
Breastfeeding is optimal for infants, but there are a few safe, exclusive breastfeeding is recommended during the
conditions when breastfeeding is not in the baby’s best first postnatal months. (7) The exact risk of transmission
interest. Breastfeeding is contraindicated for infants who is unknown, but risk is probably higher in mothers who
have classic galactosemia, an autosomal-recessive disor- have higher viral loads.
der in which the liver enzyme galactose-1-phosphate The human lymphotropic virus HTLV-1, associated
uridyltransferase is absent. Affected infants are unable to with adult T-cell leukemia and lymphoma, is uncommon
metabolize lactose or galactose, leading to liver failure in the United States. HTLV-2 is a related retrovirus.
and mental retardation. When this diagnosis is suspected, Mothers who are HTLV-1- or -2-positive should not
abrupt weaning from breastfeeding is necessary. breastfeed.
Mothers who have active untreated tuberculosis dis- Women who have herpetic lesions on their breasts
ease should be separated from their infants and advised to should refrain from breastfeeding. In the absence of
suspend breastfeeding until the mother and infant are breast lesions, the newborn can breastfeed and room-
receiving appropriate antituberculosis therapy. The in, but scrupulous hand washing and covering of any
mother should wear a mask and adhere to infection lesions is recommended to prevent possible cross-
control measures. Separation is no longer necessary once contamination.
the infant is started on isoniazid. However, if multidrug-
resistant tuberculosis is suspected, the infant should re- Medications
main separated from the mother even after he or she is Almost all drugs are excreted into human milk to some
started on isoniazid. (6) degree, but only a very few are unsafe for the infant.
Table 4 lists medications that are contraindicated when
Viruses breastfeeding. Mothers who are receiving radioactive
Human milk can transmit certain viral diseases. The isotopes, antimetabolites, or chemotherapeutic agents
viruses that can be identified in human milk and their should not breastfeed until the medications no longer are
impact on breastfeeding are listed in Table 3. excreted in the milk. Individual drugs that preclude
The World Health Organization recommends avoid- breastfeeding include lithium, atropine, chlorampheni-
ance of all breastfeeding by human immunodeficiency col, cyclosporine, bromocriptine, ergot alkaloids, and
virus (HIV)-infected mothers when replacement feeding iodides. Long-term maternal ingestion of drugs that
is acceptable, feasible, affordable, sustainable, and safe. have sedative effects can cause sedation in breastfeeding
Women in developed countries who are HIV-positive infants and withdrawal symptoms on interruption of
should not breastfeed their offspring, but in the develop- breastfeeding. (8) Although most drugs can be used
ing world when replacement feeding is not feasible or safely by breastfeeding women, physicians should make a
Pediatrics in Review Vol.27 No.11 November 2006 413
nutrition breastfeeding
Medications Contraindicated During
Table 4. mothers to avoid smoking within
the home and to make every effort
Breastfeeding to wean themselves from tobacco.
Women who have a history of
Drug/Class Possible Adverse Effects in Infant
breast reduction are at risk of insuf-
Antineoplastic agents Fetal death, congenital anomalies, organ system ficient lactation. Those diagnosed
toxicity with breast cancer can continue
Immunosuppressants Potential suppression of the immune system
Lithium High potential for toxicity breastfeeding. However, when che-
Chloramphenicol Blood dyscrasias, aplastic anemia motherapy begins, the infant must
Ergot alkaloids Ergotism poisoning be weaned. Inverted nipples should
Radiopharmaceuticals Potential toxicity; brief to full interruption of not impede breastfeeding. Usually
breastfeeding recommended the degree of inversion lessens as
Bromocriptine Suppresses prolactin secretion; hyperprolactinemic
mothers taking drug can breastfeed successfully breastfeeding continues. Women
Iodides Thyroid suppression who have acute mastitis should
continue frequent breastfeedings.
risk versus benefit assessment prior to the use of any Breastfeeding Considerations in Normal and
drugs during lactation. (8) Special Situations
American Academy of Pediatrics (AAP)
Conditions That Are Not Contraindications to Recommendations on Breastfeeding for
Breastfeeding Healthy Term Infants
Breastfeeding is not contraindicated for infants born to In its most recent recommendations, the AAP has taken
mothers who are hepatitis B surface antigen-positive. All a very strong position on promoting breastfeeding. (1)
such infants should receive hepatitis B immunoglobulin Recommendations include exclusive breastfeeding for
(HBIG) and hepatitis B virus (HBV) vaccine within the first 6 postnatal months and continuation of breast-
12 hours after birth. Multiple studies have shown that feeding for at least the first year and beyond, as long as
breastfeeding does not appear to increase the rate of desired by mother and child. Complementary foods rich
infection among neonates; moreover, in areas of high in iron and supplementary fluoride should be introduced
HBV prevalence, lack of breastfeeding places the infant beginning around 6 months of age. The AAP suggests
at greater risk of contracting the disease. enthusiastic support of breastfeeding by all health-care
Maternal hepatitis C virus (HCV) infection is not a professionals as well as recognition and sensitivity to
contraindication for breastfeeding. (1) The overall rate of cultural differences regarding breastfeeding attitudes and
maternal-infant HCV transmission among breastfed in- practices. Pediatricians should recommend human milk
fants is similar to that of formula-fed infants. It has been for all infants in whom breastfeeding is not contraindi-
suggested, but not shown, that the presence of cracks or cated. When direct breastfeeding is not possible, ex-
fissures in the nipple poses a risk for transmission of pressed human milk should be provided. Education of
HCV. Some experts believe that mothers should be both parents before and after delivery is an essential
counseled about potential risks. component of successful breastfeeding.
Although transmission of cytomegalovirus (CMV) Healthy infants should be in direct skin-to-skin con-
through breastfeeding has been established, no serious tact with their mothers immediately after birth. After the
illness or clinical symptoms in neonates fed CMV- recovery period, mother and infant should sleep in prox-
positive human milk have been reported. Breastfeeding is imity to each other to facilitate breastfeeding. Water and
not contraindicated for healthy term infants whose other fluids should not be given to breastfeeding infants
mothers have CMV infection. However, decisions about unless specifically ordered by the physician.
breastfeeding of preterm and immunosuppressed infants During the first weeks of breastfeeding, the infant
should be made with consideration of the potential ben- should have 8 to 12 feedings every 24 hours. After
efits of human milk versus the risk of CMV transmission. breastfeeding is well established, the frequency of feed-
Freezing and pasteurization can decrease the CMV viral ing may decline to about eight times per 24 hours. The
load in milk significantly. mother should offer both breasts at each feeding for as
Maternal tobacco smoking is not a contraindication long as the infant remains at the breast. In the early weeks
to breastfeeding. Clinicians, however, should advise after birth, infants should be aroused to feed if 4 hours
414 Pediatrics in Review Vol.27 No.11 November 2006
nutrition breastfeeding
early as possible. If the respiratory status of the infant
Markers of Successful
Table 5. precludes direct breastfeeding, gavage feedings with ex-
pressed human milk may be considered. Fortified human
Breastfeeding milk is recommended for many low-birthweight infants.
● 7% or less weight loss in first few days after birth Banked human milk can be a suitable alternative for
● Return to birthweight by at least 2 weeks infants whose mothers are unable or unwilling to breast-
● Weight gain per day of 20 to 30 g during first 3 feed.
postnatal months
● Lactation established in mother by 2 to 4 days after
MULTIPLE INFANTS. Most mothers of multiple infants
birth
● At least eight breastfeeding events every 24 hours are capable of producing most or all of the milk required
● Baby is latching onto breast easily for two to four infants. These mothers need substantial
● Three to six stools and four to six voids by 5 to 7 help and support with early feedings. Simultaneous feed-
days of age ing saves time, but it is important to assess each infant
initially at the breast separately.
have passed since the last feeding. It is recommended DOWN SYNDROME. Hypotonia, abnormal anatomic
that trained medical personnel in the hospital evaluate structure of the oral cavity, and significant congenital
breastfeeding at least twice daily, including observation heart disease may affect breastfeeding of infants who have
of position, latch, and milk transfer. Down syndrome. Large, flattened tongues cause diffi-
Follow-up of breastfeeding infants after hospital dis- culty latching on. In addition, affected infants may have
charge is critically important. The AAP recommends difficulty swallowing and are at increased risk of pulmo-
early follow-up within 2 days of discharge for any infant nary aspiration. Feeding usually improves as the infant’s
sent home when he or she is younger than 72 hours of muscle tone improves. Despite these challenges, the
age. An infant who has many risk factors might need to prevalence of breastfeeding among patients who have
be seen earlier (within 24 h of discharge). The health- Down syndrome is similar to that of the general popula-
care professional should evaluate the infant’s weight, tion. Very close monitoring of growth and development
hydration status, and the presence or absence of jaun- is imperative for children who have Down syndrome and
dice. Markers of successful breastfeeding are listed in are breastfed exclusively.
Table 5. The next ambulatory visit can be scheduled at
2 to 3 weeks of age so the physician can monitor weight CLEFT LIP AND PALATE. Studies reveal that approxi-
gain and provide additional support. Exclusive breast- mately 25% of infants who have cleft lip and palate have
feeding is one of several risk factors for worsening hyper- early feeding problems, leading to poor weight gain over
bilirubinemia in the infant. the first few postnatal months. Patients who have isolated
cleft lip have better feeding records and faster weight
Nursing While Pregnant gain compared with those who have isolated cleft palate.
Pregnancy can occur while lactating. There is no need to Common feeding problems include inability to generate
wean the first infant from the breast. It is possible to negative sucking pressure in the oral cavity, excessive air
lactate throughout pregnancy and to have both infants at intake, nasal regurgitation, and fatigue. However, for
the breast postpartum. This feeding pattern can be used patients who have cleft lip/palate, breastfeeding offers
without any apparent ill effects on the nourishment of several benefits over bottle-feeding. It allows a better seal
the new infant. The mother should be provided with due to pliability of the human breast, promotes develop-
psychological support as well as adequate rest and nour- ment of oral and facial muscles, and decreases the risk of
ishment. ear and respiratory infections. After repair of the cleft,
experts recommend resumption of nursing as early as
Breastfeeding Newborns Who Have Special possible, if not in the immediate postoperative period.
Needs
PRETERM OR ILL INFANTS. In this situation, breast- Practical Issues in Breastfeeding
feeding may be delayed for days or weeks. Medical per- Guidelines for Collection and Storage of
sonnel should advise mothers to begin expressing milk Expressed Human Milk
within hours of giving birth. Mother-infant skin-to-skin It is very important to maintain cleanliness to minimize
contact and direct breastfeeding should be encouraged as bacterial contamination in the process of collection. The
Pediatrics in Review Vol.27 No.11 November 2006 415
nutrition breastfeeding
mother should be instructed in washing her hands, her absolute contraindications to breastfeeding. It is imper-
breasts, and pumping equipment. Many hospitals, phar- ative that pediatricians and other medical care practitio-
macies, and local rental companies have electric pumps ners have an in-depth understanding of the innumerable
that are very time-efficient. Human milk can be stored in benefits of breastfeeding. Breastfeeding should become a
either glass or plastic containers. Glass or flexible bottles cultural norm among all women, regardless of education
(polypropylene containers) have significant advantages in and socioeconomic status.
maintaining the stability of the components of human
milk, particularly IgA.
Freshly expressed human milk can be used safely for References
up to 8 hours at room temperature, but the potential for 1. AAP Section on Breastfeeding Policy Statement. Breastfeeding
and the use of human milk. Pediatrics. 2005;115:496 –506
contamination is greater when milk is not refrigerated. 2. Horwood LJ, Darlow BA, Mogridge N. Breast milk feeding and
Various studies support storing milk in a refrigerator cognitive ability at 7– 8 years. Arch Dis Child Fetal Neonatal Ed.
(4°C/39°F) for up to 5 days without increasing the risk 2001;84:F23–F27
of bacterial contamination and to facilitate retaining 3. Lopez-Alarcon M, Villalpando S, Fajardo A. Breastfeeding low-
some cell viability. Because refrigerated milk separates, ers the frequency and duration of acute respiratory infection and
diarrhea in infants under six months of age. J Nutrition. 1997;127:
the container should be shaken vigorously before feeding 436 – 443
the baby. Milk can be kept for 3 months in a self- 4. Holberg CJ, Wright AL, Martinez FD, Ray CG, Taussig LM,
defrosting freezer and for 12 months in a freezer that has Lebowitz MD. Risk factors for respiratory syncytial virus-associated
no defrost cycle that maintains a temperature of 0°F lower respiratory illnesses in the first year of life. Am J Epidemiol.
(⫺20°C). The milk should be thawed in the refrigerator 1991;133:1135–1151
5. Oddy WH, Peat JK, de Klerk NH. Maternal asthma, infant
and used within 24 hours. Defrosting in the microwave is feeding and the risk of asthma in childhood. J Allergy Clin Immu-
not recommended. nol. 2002;110:65– 67
6. American Academy of Pediatrics, Committee on Infectious Dis-
Banking Human Milk eases. Management of newborn infant whose mother has tubercu-
The Human Milk Banking Association of North America losis. 2006 Red Book, Report of the Committee on Infectious Diseases.
27th ed. Elk Grove Village, Ill: American Academy of Pediatrics;
was established in 1985. It supervises collection, screen- 2006:694 – 695
ing, processing, storing, and distribution of donated 7. World Health Organization. New data on the prevention of
human milk for infants who are prescribed human milk. mother to child transmission of HIV and their policy implications.
Donors are screened carefully and are taught how to Conclusions and recommendations. Technical consultation on be-
express their milk by using sanitary collecting methods. half of the UNFPA/ UNICEF/WHO/UNADIS Inter-Agency
Task Team on Mother-Child Transmission of HIV. Geneva, Swit-
Donated milk is treated by heat to destroy any bacteria or zerland: October 2000. Available at: http://www.who.int/
viruses. Common reasons for prescribing donor milk reproductive-health/stis/mtct/kesho_bora.htm. Accessed 8/26/06
include allergies and formula intolerance, prematurity, 8. Hale T. Medications and Mother’s Milk. 11th ed. Amarillo, Tex:
failure to thrive, immunologic deficiencies, and postop- Pharmasoft Publishing; 2004
erative nutrition.
Conclusion Suggested Reading
Cahill JB, Wagner CL. Challenges in breastfeeding. Contemp Pedi-
Breastfeeding ensures the best possible physical health as atr. 2002;19:94 –138
well as developmental and psychosocial outcomes for Churchill RB, Pickering LK. The pros (many) and cons (a few) of
infants. Overwhelming evidence supports strong recom- breastfeeding. Contemp Pediatr. 1998;15:108 –119
mendations to increase and sustain breastfeeding in the Lawrence RA. Breastfeeding: A Guide for the Medical Profession. 5th
ed. St Louis, Mo: Mosby-YearBook, Inc; 1999
population. The biologic and immunologic markers in
Philipp BL, Cadwell K. Fielding questions about breastfeeding.
human milk, such as the specific antibodies and cellular Contemp Pediatr. 1999;16:149 –164
factors as listed in Table 2, are very important to infant Riordan J. Breastfeeding and Human Lactation. 3rd ed. Sudbury,
health, as are the various nutrients. There are very few Mass: Jones and Bartlett Publishers; 2005
416 Pediatrics in Review Vol.27 No.11 November 2006
nutrition breastfeeding
PIR Quiz
Quiz also available at www.pedsinreview.org.
5. You are discussing the physiology of lactation with a medical student. Which of the following statements is
true?
A. After delivery, the prolactin concentration drops, leading to increased milk synthesis.
B. Lactation does not occur if pregnancy does not progress beyond 20 weeks.
C. Obesity does not interfere with lactogenesis.
D. Oxytocin causes the milk-ejection reflex or letdown.
E. The rate of milk synthesis is not related to the degree of emptiness or fullness of the breast.
6. Compared with mature human milk, colostrum contains more:
A. Calories.
B. Carbohydrate.
C. Fat.
D. Protein.
E. Vitamin C.
7. Of the following pathogens, breastfeeding is most likely to protect against infection caused by:
A. Escherichia coli.
B. Hepatitis C virus.
C. Herpes simplex virus.
D. Human immunodeficiency virus.
E. Mycobacterium tuberculosis.
8. You are evaluating a healthy breastfed newborn. In which of the following conditions would you strongly
advise against breastfeeding?
A. The mother has a history of positive purified protein derivative test with negative chest radiograph and
is currently receiving isoniazid treatment.
B. The mother is a chronic hepatitis C carrier.
C. The mother is cytomegalovirus-positive.
D. The mother is hepatitis B surface antigen-positive.
E. The mother is receiving chemotherapeutic agents for breast cancer treatment.
Pediatrics in Review Vol.27 No.11 November 2006 417
consultation with the specialist
Cardiovascular Preparticipation
Sports Screening
Anoop Singh, MD,* Michael Silberbach, MD†
Objectives After reading this article, readers should be able to:
1. Describe the key cardiac elements of the preparticipation examination.
2. Identify red flags in a patient’s cardiac history and physical examination
that warrant consultation with a cardiologist.
3. Characterize the cardiovascular findings of the well-trained athlete.
4. Recognize the common causes of sudden cardiac death on the playing field.
5. Discuss the absolute and relative contraindications to athletic participation.
Background tention than a “yes/no” response.
In the United States, the prepartici- A checklist of questions that probes
pation examination (PPE) has be- for potential cardiac disease is also
come a standard for athletic clearance helpful (see the form available in the
of high school students in nearly ev- online version of this article only).
Author Disclosure
ery state. This screening serves many Family concerns or observations
Drs Singh and Silberbach did not
purposes, but a primary goal is to complement the picture of the ado-
disclose any financial relationships restrict athletic participation of those lescent’s health. Indeed, the Ameri-
relevant to this article. who may be predisposed to dying on can Heart Association recommends
the playing field. that a parent verify all elements of the
To view a sample preparticipation The death of a high school athlete history.
evaluation form, visit devastates the child’s family, signifi- The personal history focuses on
www.pedsinreview.org and click on cantly affects the local community, symptoms such as chest pain, chest
Consultation with the Specialist. and often generates extensive media tightness, dyspnea, near-syncope,
coverage. Fortunately, sudden death syncope, dizziness, exercise intoler-
remains a rare phenomenon; best es- ance, and fatigue. The setting in
timates predict an incidence of 1 per which symptoms occur is very impor-
200,000 high school athlete-years. tant. Symptoms in the context of ath-
In 75% of such cases, cardiovascular letic activity may be a harbinger of
disease is the cause. Accordingly, cardiovascular disease. For example,
medical professionals must have a a history suggestive of vasovagal syn-
keen sense for detecting silent cardiac cope is less concerning than one of
disease in young athletes. exercise-related syncope. On the
other hand, palpitations may be
History Taking more noticeable and worrisome
The medical history is the most im- when they occur at rest.
portant part of the cardiovascular A detailed medication history in-
PPE. It is best to ask open-ended cludes both prescribed medications
questions of the patient. A volun- and supplements. When asking about
teered complaint warrants greater at- illicit drug use, particular attention
should be given to performance-
enhancing drugs such as androgenic
*Fellow, Pediatric Cardiology, Department of steroids, human growth hormone, and
Pediatrics, Oregon Health & Science University,
Portland, Ore. amphetamines.
†
Editorial Board. Important components of the
418 Pediatrics in Review Vol.27 No.11 November 2006
consultation with the specialist
past medical history include rheu-
matic fever, Kawasaki disease, myo- Red Flags in the History or Physical
Table 1.
carditis, arrhythmias, congenital
heart disease, heart murmurs, or hy-
Examination
pertension. Essential hypertension, ● Syncope or near-syncope on exertion
increasingly common in the adoles- ● Chest pain/discomfort on exertion
cent population, always warrants an ● Palpitations at rest
evaluation for secondary causes. Fi- ● Excessive shortness of breath or fatigue with activities
● Family history of Marfan syndrome, cardiomyopathy, long QT syndrome, or
nally, unexplained seizures or near-
clinically significant arrhythmias
drowning raise the possibility of car- ● Family history of premature, sudden death
diac ion channel defects, such as the ● Irregular heart rhythm
long QT syndrome (LQTS). ● Weak or delayed femoral pulses
The family history is an integral ● Fixed, split second heart sound
● Any systolic murmur graded 3/6 or greater
part of the screening process because
● Any diastolic murmur
it may initiate additional evaluation ● Stigmata of Marfan syndrome
of an asymptomatic patient. Perti- ● Chest pain in Turner syndrome
nent family history includes congen-
ital heart disease, Marfan syndrome
or other connective tissue disorders, murmurs and is performed with the completely normal 12-lead ECG
cardiomyopathy, and LQTS or other patient in both the supine and stand- tracing. Accordingly, an echocardio-
arrhythmias. Searching for silent car- ing positions. The standing position gram is often part of the primary
diac disease entails asking specifically accentuates the dynamic obstruction investigation in referred patients. Ad-
about unexplained sudden death in murmur of hypertrophic cardiomy- ditional tests at the cardiologist’s
the family, such as unexplained opathy. The abdomen must be pal- disposal include ambulatory ECG
drowning, near-drowning, seizures, pated to detect organomegaly. Fi- monitoring, 30-day ECG-event mon-
or an automobile fatality, especially nally, the physical examination must itoring, exercise stress testing, electro-
involving a family member younger include assessment of femoral pulses physiology studies, stress echocardio-
than 50 years of age. to screen for aortic coarctation. grams, cardiac magnetic resonance
imaging, cardiac catheterization, and
Physical Examination When to Refer angiography.
Vital signs are an important aspect of Referring a patient to a pediatric car- The responsibilities of the pediat-
the physical examination. The heart diologist depends on the experience ric cardiologist are threefold: 1) find-
rate and blood pressure are com- and comfort level of the primary care ing cardiovascular disease in undiag-
pared with age-specific norms. Hy- practitioner. Although each case has nosed patients and initiating therapy,
pertension in children is defined as a its own nuances, there are “red flags” 2) identifying those patients at risk
blood pressure greater than the 90th in the history and examination that for sudden cardiac death, and
percentile for age, height, and sex. usually prompt consultation with a 3) clearing healthy individuals for full
Hypertension warrants, at a mini- pediatric cardiologist (Table 1). athletic participation.
mum, four extremity blood pressure There is, however, a gray area be-
measurements and another measure- Cardiology Evaluation tween healthy-appearing and diseased
ment at a separate office visit. A patient referred to a pediatric car- hearts. The well-trained athlete’s heart
The general examination of the diologist may or may not require any falls into this indeterminate category.
patient includes an overall assess- testing, depending on the results of
ment for features suggestive of the history and physical examination.
Marfan syndrome, such as kyphosco- When more information is needed, a The Athlete’s Heart
liosis, pectus deformity, arm span chest radiograph and electrocardio- Just as aerobic and isometric exercise
greater than height, joint hypermo- gram (ECG) often are obtained. have visible effects on skeletal mus-
bility, arachnodactyly, and a tall and However, left ventricular hypertro- cle, athletic training remodels cardiac
thin body habitus. phy is difficult to diagnose on a plain muscle. Such morphologic changes
Auscultation of the chest focuses film, and as many as 15% of those present a challenge to the clinician,
on heart sounds, clicks, and cardiac who have cardiac hypertrophy have a who must distinguish between be-
Pediatrics in Review Vol.27 No.11 November 2006 419
consultation with the specialist
nign adaptation to exercise and car- ever, it should be noted that such for electrical instability. Sudden
diac disease. physiologic changes cannot be la- death is likely the result of re-entrant
Endurance training normally re- beled definitively as benign. One ventricular arrhythmias.
sults in enlargement of the left ven- long-term echocardiographic study
tricular cavity due to an increased following elite athletes showed that Congenital Coronary Artery
stroke volume. Basal cardiac output cardiac chamber enlargement per- Anomalies
is unaffected because the well- sisted despite deconditioning in 20% Coronary arteries arising from the
conditioned athlete’s resting heart of the retired athletes. Thus, the sig- wrong sinus are the second leading
rate is decreased. However, the de- nificance of exercise-induced ventric- cardiac cause of death on the playing
gree of left ventricular enlargement ular remodeling remains undefined. field. Of these congenital malforma-
can approach dimensions seen pri- tions, a left main coronary artery
marily in diseased hearts. Sudden Death originating from the right sinus of
Another conundrum is presented The exact number of young athletes Valsalva and traveling between the
by left ventricular hypertrophy. Stud- dying during competitive sports is aorta and main pulmonary artery is
ies have shown that 2% of highly uncertain. Incidence estimates range the most common. Affected patients
trained male athletes demonstrate from 1 per 44,000 to 1 per 200,000 may experience chest pain on exer-
significant increases in left ventricular athlete-years. Approximately 75% of tion. However, findings on physical
wall thickness. Thus, echocardio- all sudden deaths are due to cardio- examination and ECG are usually
graphically determined cardiac mea- vascular disease, with hypertrophic normal. The exact mechanism of
surements may overlap with diagnostic cardiomyopathy being the most sudden death is debated. The abnor-
criteria for hypertrophic cardiomyopa- common cause. Fatal events due to mal coronary vessel often arises at an
thy. In these patients, the suspicion commotio cordis comprise the bulk acute angle from the sinus of Val-
increases if there is a positive family of sports-related deaths not due to salva; this precipitous origin may pre-
history for cardiomyopathy, an asym- underlying cardiovascular disease. dispose to ischemia when myocardial
metry between the septal and poste- Knowing that the presenting event of demands increase with exercise.
rior left ventricular wall thickness by previously undetected cardiovascular
echocardiography, a lack of concur- disease may be death makes a com- Marfan Syndrome
rent left ventricular cavity enlarge- pelling case for the importance of the Marfan syndrome is an autosomal
ment, an abnormal ECG tracing, or PPE. dominant disorder caused by muta-
no decrease in thickness with decon- tions in the gene encoding the pro-
ditioning. Hypertrophic Cardiomyopathy tein fibrillin, a key component of
In addition to structural changes, (HCM) connective tissue. The estimated
the athlete’s heart displays unusual HCM is the most common cause of prevalence ranges from 1 per 5,000
ECG patterns, arrhythmias, and con- sudden cardiac death in young ath- to 1 per 10,000. Clinical features in-
duction abnormalities. An Italian letes. HCM has an autosomal domi- clude kyphoscoliosis, pectus defor-
study showed that 40% of athletes nant inheritance pattern, with more mities, arm span greater than height,
had abnormal electrical patterns on than 400 mutations on 12 genes de- joint hypermobility, arachnodactyly,
ECG recordings in a population in scribed thus far. The prevalence in pes planus, lens dislocation, myopia,
whom only 5% had a cardiovascular the general population is estimated and a history of spontaneous pneu-
abnormality. Ambulatory ECG mon- to be 0.2%. Clinical features that may mothorax. Cardiac manifestations in-
itoring in normal athletes may show raise suspicion for the disease include clude aortic root dilatation, aortic
junctional rhythm at rest, frequent symptoms of left ventricular outflow dissection, and mitral valve prolapse.
premature ventricular beats, ventric- obstruction, a heart murmur, family The diagnosis is based on the family
ular couplets, or nonsustained ven- history of HCM, or an abnormal history and clinical criteria. Sudden
tricular tachycardia that can be con- ECG tracing. Echocardiography cardiac death is due to dissection and
fused with ventricular irritation from demonstrates left ventricular hyper- rupture of the aorta.
myocarditis. trophy that classically is asymmetric.
Athletes who have left ventricular However, absence of cardiac hyper- Congenital LQTS
enlargement or hypertrophy and are trophy does not rule out the presence LQTS involves the generation of an
deemed otherwise healthy should be of HCM. At the cellular level, myo- abnormal myocardial action poten-
cleared to participate in sports. How- fibrillary disarray creates a substrate tial due to defects in cell membrane-
420 Pediatrics in Review Vol.27 No.11 November 2006
consultation with the specialist
Figure. A. 12-lead electrocardiogram tracing from a 10-year-old who has long QT syndrome, demonstrating a prolonged QTc of 590
msec. B. Rhythm strip from a 14-year-old during an episode of polymorphic ventricular tachycardia (torsades de pointes).
Pediatrics in Review Vol.27 No.11 November 2006 421
consultation with the specialist
associated ion channel proteins. The Thus, the rationale for athletic dis- contraction, resulting in an increas-
diagnosis is considered when a pro- qualification is that the cessation of ing pressure load on the heart. Static
longed QTc interval [Bazett formula athletic activity may be protective. exercise should be avoided by pa-
(QT in msecs and RR in secs): The current recommendations for tients who have left heart obstructive
QTc⫽QT/公RR] accompanies a sports eligibility are based on the disease, regurgitant aortic valves, or
history of syncope. Sensorineural consensus opinion outlined in the connective tissue disorders where
deafness, present in the autosomal 36th Bethesda Conference guide- aortic dilation is a risk. However, it
recessive form of LQTS (Jervell and lines. Although the recommenda- may be appropriate to recommend
Lange-Nielsen syndrome), may be tions generally are conservative, only moderate dynamic and low static ac-
an additional clue. Syncope is due to a handful of cardiovascular condi- tivities for these individuals. Dy-
self-limited episodes of polymorphic tions require disqualification from all namic exercises, on the other hand,
ventricular tachycardia called tor- sports (Table 2). The Bethesda eligi- require isotonic muscle contraction
sades de pointes (Figure). Prolonged bility criteria do not apply to non- and typically result in increasing the
QTc interval and a positive family competitive, recreational activities. cardiac output. High-intensity dy-
history are important risk factors for The American Heart Association has namic exercises may be stressful for
sudden death. Although the arrhyth- published separate guidelines. patients who have even mild ventric-
mia may occur at any age, there is a The clinician must consider mul- ular dysfunction. Such patients
predilection for cardiac events in ad- tiple factors, both physical and psy- might be restricted to low dynamic/
olescence. Sudden death occurs chological, before disqualifying a low static competitive sports.
when the arrhythmia degenerates particular patient. In many cases, the
into ventricular fibrillation. activities may be limited and not Conclusion
eliminated. For example, individuals The PPE is the optimal tool available
Commotio Cordis who have Marfan syndrome or an im- to primary care practitioners for pre-
Commotio cordis causes 20% of all plantable cardioverter-defibrillator are venting heart disease-related deaths
sudden deaths in young athletes. It cautioned to avoid sports that carry a on the playing field. However, there
occurs when blunt, nonpenetrating risk of bodily collision. is considerable variability in the de-
trauma to the chest produces ventric- Because different sports carry dif- tails of the screening process, and
ular fibrillation. The blow often is ferent risks, it may be possible to many states have either no or inade-
neither excessive nor associated with tailor recommendations to an indi- quate examination forms. Standard-
structural injury. Arrhythmias may vidual patient. It is possible to cate- izing the history and physical form
be induced by enhanced energy gorize various activities into static and creating accreditation criteria for
transfer to the heart through the and dynamic exercise components, clinicians who perform the examina-
child’s compliant chest wall coincid- permitting classification in terms of tion would be two good steps toward
ing with a vulnerable period of car- the type of stress (Table 3). Static optimizing the PPE. The cost/
diac repolarization. Projectiles such exercise involves isometric muscle benefit ratio of obtaining an ECG or
as baseballs and hockey pucks have
been implicated most often in com-
motio cordis. Survival is less than
15% but improves if prompt cardio- Absolute Contraindications to Sports
Table 2.
pulmonary resuscitation and defibril- Participation
lation occur.
● Pulmonary vascular disease with cyanosis and large right-to-left shunt
Eligibility and ● Severe pulmonary hypertension
● Severe aortic stenosis or regurgitation
Disqualification From Sports ● Severe mitral stenosis or regurgitation
Young athletes who have cardiovas- ● Cardiomyopathies
cular disease are at greater risk for ● Vascular form of Ehlers-Danlos syndrome
sudden death than are nonathletes ● Coronary anomalies of wrong sinus origin
who have cardiac disease. Perhaps ex- ● Catecholaminergic polymorphic ventricular tachycardia
● Acute phase of pericarditis
treme exercise stress triggers rare
● Acute phase of myocarditis (at least 6 mo)
events such as malignant arrhythmias ● Acute phase of Kawasaki disease (at least 8 wk)
that otherwise would remain hidden.
422 Pediatrics in Review Vol.27 No.11 November 2006
consultation with the specialist
Classification of Sports According to
Table 3. and an ECG in addition to the his-
tory and physical examination. In
Type of Exercise this month’s Internet-only pages of
PIR, Dr Renato Vitiello cites data
Low Dynamic Moderate Dynamic High Dynamic
suggesting that sudden death from
Low Static Billiards Baseball Badminton HCM in athletes can be reduced by
Bowling Softball Field hockey this approach. The Italian perspec-
Cricket Fencing Racquetball
Golf Table tennis Soccer tive may soon be adopted by all of
Riflery Volleyball Tennis Europe. – Michael Silberbach, MD
Track (long distance)
Moderate Archery Field events Basketball
Static Auto racing Figure skating Ice hockey
Diving Football/Rugby Lacrosse
Equestrian Rodeo Track (middle distance) Suggested Reading
Motorcycling Surfing Swimming Corrado D, Pelliccia A, Bjornstad HH, et al.
Track (sprinting) Cross-country skiing Cardiovascular pre-participation screen-
High Static Bobsledding Bodybuilding Boxing ing of young competitive athletes for
Field (throwing) Downhill skiing Canoeing/Kayaking prevention of sudden death: proposal
Gymnastics Skateboarding Cycling for a common European protocol. Con-
Sailing/Windsurfing Snowboarding Rowing sensus Statement of the Study Group of
Sport climbing Wrestling Speed skating Sport Cardiology of the Working Group
Weight lifting Triathlon/Decathlon of Cardiac Rehabilitation and Exercise
Physiology and the Working Group of
Modified from Task Force 8; classification of sports. J Am Coll Cardiol. 2005;5:1366. Copyright Myocardial and Pericardial Diseases of
2005. The American College of Cardiology Foundation and American Heart Association, Inc. the European Society of Cardiology.
Permission granted for one time use. Additional reproduction is not permitted without permission of
the ACC/AHA. Eur Heart J. 2005;26:516 –524
Glover DW, Maron BJ. Profile of prepartici-
pation cardiovascular screening for high
school athletes. JAMA. 1998;279:
focused cardiac ultrasonography to 1817–1819
accidents, homicide, and suicide are
Maron BJ. Sudden death in young athletes.
rule out hypertrophic cardiomyopa- far more prevalent problems, causing N Engl J Med. 2003;349:1064 –1075
thy continues to be debated in the 10,000 deaths a year in 15- to 19- Maron BJ, Shirani J, Poliac LC, Mathenge
United States. A recent consensus year-olds. Although the primary care R, Roberts WC, Mueller FO. Sudden
statement from Europe has advo- practitioner assiduously seeks to death in young competitive athletes.
Clinical, demographic, and pathological
cated the use of 12-lead ECGs based identify heart disease during the
profiles. JAMA. 1996;276:199 –204
on the 25-year experience in Italy screening visit, it is equally important Moss AJ. Long QT syndrome. JAMA.
where electrocardiography has been to promote a physically active life- 2003;289:2041–2044
an integral part of the PPE. (See style that encourages both mental Pelliccia A, Maron BJ, Culasso F, et al.
commentary by Dr Renato Vitiello in and cardiovascular health. Clinical significance of abnormal elec-
trocardiographic patterns in trained ath-
the Internet-only pages.)
letes. Circulation. 2000;102:278 –284
This article has focused on identi- EDITORIAL BOARD NOTE. In the Pelliccia A, Maron BJ, De Luca R, Di Paolo
fying silent cardiovascular disease United States, medical evaluation FM, Spataro A, Culasso F. Remodeling
and defining criteria for determining prior to participation in sports is stan- of left ventricular hypertrophy in elite
sports eligibility in young athletes. It dard practice, but national guidelines athletes after long-term deconditioning.
Circulation. 2002;105:944 –999
is important to remember that the for the PPE are not established. In
36th Bethesda Conference: eligibility rec-
incidence of sudden cardiac death Italy, a federal law sets a single, high ommendations for competitive athletes
during sports participation is ex- standard for the entire country that with cardiovascular abnormalities. J Am
tremely low. In the United States, requires certification for screeners Coll Cardiol. 2005;45:1312–1375
Pediatrics in Review Vol.27 No.11 November 2006 423
consultation with the specialist
PIR Quiz
Quiz also available online at www.pedsinreview.org.
9. A pediatrician is conducting a history and preparticipation physical examination on a teenager. In the
medical history, the event that would be most suspicious for an inherited cardiac ion channel defect, such
as the long QT syndrome, is:
A. Extreme weight loss.
B. History of narcolepsy.
C. Near-drowning.
D. Status asthmaticus.
E. Episodes of vertigo.
10. Sudden death during competitive sports remains a tragic phenomenon in athletes. The percent of these
deaths attributable to underlying cardiovascular disease is estimated to be:
A. 20%.
B. 40%.
C. 50%.
D. 75%.
E. 100%.
11. You have been asked to help at the local sports clinic day for your community. Your assignment is the
cardiovascular station for the high school football team. In examination of the athletes, the physical
finding most suggestive of hypertrophic cardiomyopathy is:
A. A continuous murmur heard on auscultation.
B. A pectus deformity.
C. A systolic murmur accentuated in the standing position.
D. Joint hypermobility.
E. Weak or delayed femoral pulses.
12. You are examining a cross country runner who has had occasional episodes of chest pain. His daily
training includes running 10 miles a day. There is a family history of sudden death of an uncle at a young
age while playing football, raising your concern about cardiomyopathy. You schedule him for
echocardiography. The information on this study that would most suggest hypertrophic cardiomyopathy is:
A. Asymmetric thickness between the septal and posterior left ventricular wall.
B. Bicuspid aortic valve.
C. Left ventricular cavity enlargement.
D. Left ventricular thickening that normalizes with a month of deconditioning.
E. The presence of a patent foramen ovale.
For the following questions, match the specific condition with the way this condition might cause a fatal
event.
13. Commotio cordis
14. Congenital coronary artery anomalies
15. Hypertrophic cardiomyopathy
16. Long QT syndrome
17. Marfan syndrome
A. Aortic dissection.
B. Blunt trauma to the chest wall producing ventricular fibrillation.
C. Electrically unstable myocardium as substrate for ventricular arrhythmias.
D. Myocardial ischemia leading to ventricular fibrillation.
E. Torsades de pointes degenerating into ventricular fibrillation.
424 Pediatrics in Review Vol.27 No.11 November 2006
index of suspicion
Case 1 Presentation Case 2 Presentation
A 10-month-old boy is brought to a A 4-year-old boy is brought to the
community ED because he started clinic because of a chest deformity.
vomiting last night and “has not Born at term, his birthweight was 3.8
been the same since.” This morning, kg, and his perinatal course was un-
his mother noted that he was breath- remarkable. When he was 1 year old,
ing fast. He had a low-grade fever his mother first noticed a concavity in
this morning, but none prior. He has his mid-chest region. Two years ago,
had no weight loss or diarrhea and he developed mild intermittent
has not been exposed to illness. In- asthma that has been well controlled
The reader is encouraged to write with allergen avoidance and occa-
travenous access is obtained, and the
possible diagnoses for each case before sional inhaled bronchodilator ther-
child is intubated because of respira-
turning to the discussion. We invite apy. His weight is 17 kg (50th per-
readers to contribute case tory distress and is flown to a chil-
centile) and his height is 112 cm
presentations and discussions. dren’s hospital.
Please inquire first by contacting Dr. (99th percentile). His development
On examination, the boy’s tem-
Nazarian at LFredN@aol.com. is consistent with his age, except for
perature is 37.6°F (99.7°C), heart moderate language delays, for which
rate is 158 beats/min, and blood he receives speech therapy.
pressure is 90/44 mm Hg. His respi- On physical examination, a
Author Disclosure
ratory rate had been 60 breaths/min marked pectus excavatum deformity
prior to being intubated. He is a is evident, as well as thoracic spine
Drs McPeak, Guerra, Nefcy, LaShell,
plump, robust infant who is sedated scoliosis and bilateral pes planus. Ad-
Wolf, and Algon did not disclose any
on the ventilator. Faint crackles are ditional clinical findings lead to sus-
financial relationships relevant to audible in his lungs. His skin is warm picion of a specific syndrome.
these cases. and well perfused. The rest of his
findings are normal.
To view Suggested Reading lists for these
cases, visit pedsinreview.org and click on Laboratory findings include glu- Case 3 Presentation
Index of Suspicion. cose, 176 mg/dL (9.8 mmol/L); so- A 14-year-old boy is sent to the ED
dium, 140 mEq/L (140 mmol/L); by his pediatrician because of a
potassium, 3.1 mEq/L (3.1 mmol/); 2-month history of increasing fa-
chloride, 115 mEq/L (115 mmol/L); tigue, dyspnea on exertion, and an
Frequently Used Abbreviations 8-lb weight loss. A chest radiograph
bicarbonate, 10 mEq/L (10 mmol/
ALT: alanine aminotransferase L); calculated anion gap, 15 mEq/L performed yesterday shows bilateral
AST: aspartate aminotransferase (15 mmol/L); BUN, 5 mg/dL patchy infiltrates. He denies fever,
BUN: blood urea nitrogen (1.8 mmol/L); and creatinine, vomiting, diarrhea, changes in appe-
CBC: complete blood count tite, or feeling lightheaded. The boy
0.3 mg/dL (26.5 mcmol/L).
CNS: central nervous system recently visited Puerto Rico for
A blood gas reveals a pH of 7.29 with
CSF: cerebrospinal fluid 10 days and works in a dog kennel on
a bicarbonate level of 14 mEq/L
CT: computed tomography weekends. He has had no significant
(14 mmol/L), a carbon dioxide con-
ECG: electrocardiography past illnesses and does not take any
centration of 14 torr, and a base deficit
ED: emergency department medications on a regular basis.
of ⫺18.6 mEq/L. His WBC count is On physical examination, his tem-
EEG: electroencephalography
14.9⫻103/mcL (14.9⫻109/L) with perature is 97.6°F (36.5°C), heart
ESR: erythrocyte sedimentation
71% neutrophils and 2% bands. He is rate is 102 beats/min, respiratory
rate
started on vasoactive medication for rate is 20 breaths/min, and blood
GI: gastrointestinal
hypotension and treated for sepsis, pressure is 114/68 mm Hg. There
GU: genitourinary
but the clinicians are concerned that are diminished breath sounds bilater-
Hct: hematocrit
Hgb: hemoglobin he has had minimal fever and no rash, ally throughout his lung fields, but
MRI: magnetic resonance imaging and the laboratory findings are puz- he has no respiratory distress. His
WBC: white blood cell zling. An additional blood test re- oxygen saturation is 92% on room
veals the diagnosis. air.
Pediatrics in Review Vol.27 No.11 November 2006 425
index of suspicion
The boy’s WBC count is distress that required intubation led gastric irritation. Other effects in-
6.8⫻103/mcL (6.8⫻109/L), Hgb the clinicians to consider an underly- clude altered hearing (usually tinni-
value is 16.1 g/dL (160 g/L), Hct ing metabolic derangement. Other tus), fever, and altered mental status
is 45.6% (0.456), and platelet count disorders to consider in this case are that can range from agitation to sei-
is 283⫻103/mcL (283⫻109/L). methanol toxicity, uremia, diabetic zures to stupor and coma.
Electrolyte concentrations, liver ketoacidosis, paraldehyde ingestion, In the initial phase of aspirin over-
function tests, and protein and albu- iron and isoniazid toxicities, lactic ac- dose, patients experience respiratory
min concentrations are within nor- idosis, and ethylene glycol ingestion. alkalosis due to direct stimulation of
mal limits. Blood glucose concentra- The addition of salicylism to the list the CNS respiratory drive. To correct
tion is 92 mg/dL (5.1 mmol/L), creates the “MUDPILES” mne- this alkalosis, bicarbonate is excreted
calcium is 12.4 mg/dL (3.1 mmol/ monic. in the urine, causing alkaluria. Ini-
L), and ionized calcium is 5.6 mg/ In this case, the child’s mother tially, potassium also is excreted in
dL (1.4 mmol/L). His ESR is 3 mm/ later discovered that one of the sib- the urine, leading to global hypoka-
h. A CT scan of his chest reveals lings had given the infant several lemia. In the next phase of salicylate
bilateral ground-glass opacities with adult aspirin tablets. Although the toxicity, the kidneys attempt to pre-
prominent mediastinal and hilar ingestion history was not known at serve the potassium level by an ex-
lymph nodes bilaterally. He is admit- the time of admission, a thorough change for hydrogen ions in the
ted to the hospital for intravenous investigation of the child’s wide an- urine. This paradoxic aciduria in the
hydration, treatment of his hypercal- ion gap acidosis led to the diagnosis. face of a respiratory alkalosis is a hall-
cemia and oxygen requirement, and Other supporting laboratory findings mark of aspirin toxicity.
additional evaluation of his pulmo- included the potassium concentra- In the final stages of aspirin over-
nary disease. tion of 3.1 mEq/L (3.1 mmol/L) and dose, hyperpnea continues as a re-
serum bicarbonate level of 10 mEq/L sponse to the primary metabolic aci-
(10 mmol/L). dosis. This exaggerated breathing
Case 1 Discussion contributes further to insensible wa-
The child had an anion gap acidosis, The Disorder ter losses. Although adults tend to
but no evidence of a disorder that Aspirin toxicity remains one of the have a mixed respiratory alkalosis and
would cause lactic acidosis. Although most serious ingestions in the pediat- metabolic acidosis, acidosis often
he had been vomiting for 12 hours, ric population. Despite the recent predominates in young children. Fi-
he had no other insensible losses to declining incidence, there still are ap- nally, as in this infant, salicylates in-
explain the rapid deterioration. Dia- proximately 16,000 cases yearly of crease pulmonary vasculature perme-
betic ketoacidosis seemed unlikely aspirin overdose in this country, re- ability, leading to noncardiogenic
because his glucose level never ex- sulting in 30 to 35 deaths. An acute pulmonary edema.
ceeded 200 mg/dL (11.1 mmol/L). toxic dose for a child is greater than
The wide anion gap acidosis 150 mg (approximately one half of a Laboratory Evaluation
prompted measurement of salicylate 325-mg adult tablet) per kg. Al- Several studies should be ordered in
concentrations, although there was though overall use of aspirin has de- cases of suspected salicylate toxicity.
no history of ingestion. Salicylates creased, most households in the Electrolytes, BUN, creatinine, arte-
were present at a toxic level of United States still contain salicylates rial blood gases, complete blood
60 mg/dL (4.3 mmol/L). The pa- in one form or another (tablets, bis- count, and liver function tests should
tient was alkalinized immediately and muth compounds, keratolytic agents). be checked immediately. Hypokale-
dialyzed. In 24 hours, he was extu- mia is common and can be severe.
bated and was doing well. Pathophysiology Salicylate levels should be checked
Salicylates have a broad scope of ac- immediately if ingestion is suspected
Laboratory Clues tion, especially in toxic doses, be- and subsequently checked every 2 to
Severe dehydration from vomiting or cause of their ability to uncouple ox- 4 hours until decreasing or reaching
diarrhea can cause a significant lactic idative phosphorylation, inhibit less than 30 mg/dL (2.2 mmol/L).
acidosis due to tissue hypoxemia and amino acid synthesis, and inhibit Although levels typically peak 4 to
hypoperfusion. However, this child Krebs cycle enzymes. The emesis and 6 hours after aspirin ingestion and
had only a brief history of vomiting. nausea that patients experience after correlate poorly with clinical symp-
The rapid breathing and respiratory aspirin ingestion are related to direct toms, prolonged peaking of salicy-
426 Pediatrics in Review Vol.27 No.11 November 2006
index of suspicion
lates occurs with ingestion of enteric- toxicity or if there are signs of pulmo- tic, pulmonary, and mitral valve re-
coated tablets or in the presence of nary edema, renal failure, persistent gurgitation.
any obstruction in the GI tract, such altered mental status, worsening vital Ophthalmologic examination re-
as a pill bezoar or pylorospasm. signs such as fever, or congestive vealed bilateral astigmatism. CT scan
As in this patient, if the diagnosis heart failure. of the chest showed a severe pectus
is uncertain, additional laboratory Intubation might be considered excavatum deformity.
testing should be undertaken to rule in the most seriously ill patients. Cli- Although no history of MS was
out other causes of anion gap acido- nicians should realize, however, that recorded in the family, the patient
sis. Serum lactate, osmolarity, and a intubation of the patient poisoned by was diagnosed as having emerging
urinalysis looking for ketones can be salicylates can be dangerous. The pa- MS based on the presence of major
helpful. It also may be useful to mea- tient’s own ability to hyperventilate skeletal and cardiovascular findings,
sure iron and alcohol levels (looking and regulate acidosis is suppressed, and he was referred for additional
for methanol and ethylene glycol). and he or she may develop worsening management.
As always, a thorough history is indi- acidosis.
cated, particularly focusing on all Rarely do long-term sequelae re- The Condition
medications, including over-the- sult from salicylate toxicity. When MS is an autosomal dominant disor-
counter items, in the household. recognized and treated early, most der that affects 1 in 10,000 individu-
pediatric patients do very well. als in the United States. Thirty per-
Treatment cent of cases represent a new
If the patient is alert, activated char- mutation. A mutation in the gene
Lessons for the Clinician
coal should be administered. Gastric that encodes fibrillin-1 (FBN1) is the
It is important to consider salicylism
lavage usually is not recommended genetic basis of this disorder, and
in the differential diagnosis of a child
unless the ingestion is believed to more than one mutation has been
who has an anion gap acidosis. In this
have been a large, life-threatening noted. Defective connective tissue is
case, a careful review of the initial
dose and has been brought to medi- the mechanism through which ab-
history, physical findings, and labora-
cal attention within 1 hour. Most normalities develop.
tory studies narrowed the differential
important in the treatment of salicyl- The diagnosis of MS relies on the
diagnosis significantly. Early recogni-
ism is the correction of multiple met- recognition of both major and minor
tion and treatment can be life-saving.
abolic derangements and dehydra- clinical manifestations. In the ab-
(Katie E. McPeak, MD, Children’s
tion. Initially, fluid boluses should be sence of a family history of the disor-
Hospital of Pittsburgh, Pittsburgh,
considered in the face of severe dehy- der, the diagnosis is made by noting
Pa.)
dration. Caution must be exercised one major manifestation from two
in the presence of pulmonary edema different systems and involvement of
or renal failure. a third system with either a major or
Alkalinization enhances salicylate Case 2 Discussion minor criterion (Table). If a muta-
elimination and should be instituted On further examination, the boy’s tion known to cause MS has been
promptly. A goal for serum pH arm span was 114 cm and arm span- identified in a member of the family,
should be approximately 7.5, with a to-height ratio was 1.01 (upper limit the diagnosis requires one major cri-
goal for urinary pH of greater than of normal, 1.05). His lower segment terion and involvement of a second
7.5. Standard recommendations sug- measured 59 cm, upper segment was organ system.
gest using a 1 to 2-mEq/kg bolus of 53 cm, and upper-to-lower segment There is great clinical variability
bicarbonate followed by a sodium bi- ratio was 0.9 (normal, ⬎1). A scoli- among individuals as to when mani-
carbonate drip. Because persistent osis series showed a 25-degree devi- festations of the disorder develop.
hypokalemia may interfere with alka- ation of the thoracic spine to the The most serious problem is aortic
linization of the urine and salicylate right. enlargement, which may involve
excretion, it is critical to add potas- The presence of major skeletal multiple levels of the aorta, including
sium to fluids in patients who do not features of Marfan syndrome (MS) the sinus of Valsalva, the ascending
have renal failure. prompted referral for cardiac and aorta, and beyond. Aortic root en-
Dialysis should be instituted if the ophthalmologic evaluation. An largement can progress to cata-
serum salicylate level is greater than echocardiogram showed dilatation of strophic dissection. Cardiovascular
100 mg/dL (7.2 mmol/L) in acute the sinuses of Valsalva as well as aor- abnormalities manifest during child-
Pediatrics in Review Vol.27 No.11 November 2006 427
index of suspicion
Table. Diagnostic Criteria for Marfan Syndrome
System Major Criteria Minor Criteria
Skeletal System Presence of at least four of the following ● Pectus excavatum of moderate severity
manifestations: ● Joint hypermobility
● Pectus carinatum ● Highly arched palate with crowding of
● Pectus excavatum requiring surgery teeth
● Reduced upper-to-lower segment ratio ● Facial appearance (dolichocephaly, malar
or arm span-to-height ratio greater hypoplasia, enophthalmos, retrognathia,
than 1.05 down-slanting palpebral fissures)
● Wrist (distal phalanx protrudes beyond
border of clenched fist) and thumb
(thumb and fifth digit overlap circling
the wrist) signs
● Scoliosis >20° or spondylolisthesis
● Reduced extention at the elbows
(<170°)
● Medial displacement of the medial
malleolus causing pes planus
● Protrusio acetabulae of any degree
(ascertained on radiographs)
Ocular System ● Ectopia lentis (dislocated lens) ● Abnormally flat cornea (as measured by
keratometry)
● Increased axial length of globe (as
measured by ultrasonography)
Cardiovascular System ● Dilatation of the ascending aorta with ● Mitral valve prolapse with or without
or without aortic regurgitation and mitral valve regurgitation
involving at least the sinuses of ● Dilatation of the main pulmonary artery,
Valsalva in the absence of valvular or peripheral
OR pulmonic stenosis or any other obvious
● Dissection of the ascending aorta cause, below the age of 40 y
● Calcification of the mitral annulus below
the age of 40 y
● Dilatation or dissection of the descending
thoracic or abdominal aorta below the
age of 50 y
Pulmonary System None ● Spontaneous pneumothorax
● Apical blebs (ascertained by chest
radiography)
Skin and Integument None ● Stretch marks not associated with
marked weight changes, pregnancy, or
repetitive stress
● Recurrent incisional hernias
Dura ● Lumbosacral dural ectasia by CT or None
MRI
Family/Genetic ● Having a parent, child, or sibling who None
History meets these diagnostic criteria
independently
● Presence of a mutation in FBN1 known
to cause the Marfan syndrome
● Presence of a haplotype around FBN1,
inherited by descent, known to be
associated with unequivocally
diagnosed Marfan syndrome in the
family
CT⫽computed tomography, MRI⫽magnetic resonance imaging
From De Paepe A, Devereux RB, Dietz HC, Hennekam RC, Pyeritz RE. Revised diagnostic criteria for the Marfan syndrome. Am J Med Genet.
1996;62:417– 426. Published with permission of The American Journal of Medical Genetics.
428 Pediatrics in Review Vol.27 No.11 November 2006
index of suspicion
hood in about 25% of cases and are tional investigations are required. It sure that additional complications do
progressive in about 33% of affected is particularly helpful to perform an not result.
individuals. Dilatation of the mitral extended skeletal examination, with Children at risk for aortic enlarge-
annulus is a common cause of mitral additional measurements beyond the ment or dissection should refrain
valve regurgitation in these patients. usual height and weight. from collision and contact sports,
The chordae tendineae also can competitive sports, and exercises that
lengthen and rupture spontaneously. involve muscle straining, such as
Heart disease presenting in in- Management weight lifting.
fancy typically is mitral valve pro- If diagnostic criteria for MS are met,
lapse, whereas aortic disease usually is the affected child should be referred Lessons for the Clinician
identified during later childhood and for evaluation by a multidisciplinary It is important to recognize that al-
adolescence, when the characteristic medical team that includes a geneti- though tall stature, scoliosis, anterior
body habitus calls attention to the cist and a cardiologist who has expe- chest deformity, arachnodactyly,
general diagnosis of MS. rience in the management of MS. joint laxity, and flat feet are common
Dislocated lenses commonly de- All children who have MS require in the general population, diagnostic
velop by the age of 10 years. The frequent assessment of the aortic importance increases dramatically
skeletal features can become more root. Most patients afflicted with when such findings are prominent
pronounced during periods of rapid aortic enlargement are treated with and found in combination. The pur-
growth. Dural ectasia tends to de- medications such as beta blockers to pose of the diagnostic evaluation of
velop in adulthood, although this reduce hemodynamic stress. This tall stature is to distinguish the com-
feature can occur at an earlier age. treatment can slow the growth rate monly occurring, normal, familial
The phenomenon of partial ex- of the aortic root. Standard subacute constitutional variant from the rare
pression of MS in a child in whom the bacterial endocarditis prophylaxis pathologic conditions. Often, when
full criteria are suspected to appear at should be implemented in those hav- the history suggests familial tall stat-
an older age has been termed ing valve disease. Musculoskeletal ure and the findings on physical ex-
“emerging Marfan syndrome.” abnormalities of the chest or spine amination are entirely normal, no
are the most common cause of chest laboratory tests are indicated.
Differential Diagnosis pain. However, the diagnosis of aor- Early diagnosis and management
Mutations in the fibrillin gene FBN1 tic dissection always should be con- of MS and overlapping conditions
may result in overlapping pheno- sidered in these cases. The combina- can save lives. Pediatricians need to
types, including the MASS pheno- tion of dysphonia caused by traction be aware of the early manifestations
type (mitral valve prolapse, mild aor- of the recurrent laryngeal nerve and of MS so prompt evaluation and
tic enlargement, nonspecific skin and chest discomfort is rare, but highly management can be instituted. (Abel
skeletal features), familial thoracic suggestive of aortic dissection. If aor- Guerra, MD, Christine Nefcy, MD,
aortic aneurysms, familial ectopia tic dissection is suspected, cardiac Mark LaShell, MD, 374th Medical
lentis, isolated skeletal features, and MRI is the best imaging modality. Group, Yokota Air Base, Japan)
mitral valve prolapse syndrome. Progression of skeletal abnormal- The views expressed in this case
Other syndromes that have similar ities can be dramatic in periods of are those of the authors and do not
clinical features include homocystin- rapid growth. Evaluation and reflect the official policy of the De-
uria, Ehlers-Danlos syndrome, Stick- follow-up by an orthopedist is indi- partment of Defense or other depart-
ler syndrome, Klinefelter syndrome, cated in these cases. ments of the United States govern-
and congenital contractural arachno- Many of the medical problems ment.
dactyly. seen in conditions such as emerging
The tall, thin teenager who has MS, MASS phenotype, and familial
long fingers presents a challenge to aortic dilatation are the same as those Case 3 Discussion
the clinician, who might suspect MS seen in patients who have MS. Thus, An extensive infectious evaluation re-
but is not sure of how extensive an regardless of the diagnosis, it is im- vealed no evidence of bacterial infec-
evaluation should be undertaken. If portant to adhere to the treatment tion, Mycoplasma or Legionella infec-
the history is suggestive of any ge- regimen prescribed for the particular tion, or viral infection, including
netic disorders or the physical exam- characteristics that do exist and be Epstein-Barr virus, cytomegalovirus,
ination reveals abnormalities, addi- conscientious about follow-up to en- and human immunodeficiency virus.
Pediatrics in Review Vol.27 No.11 November 2006 429
index of suspicion
An endocrinologic evaluation failed eyes, kidneys, lymphatics, and heart. pathogenesis of the granuloma in-
to identify a cause for his hypercalce- In one series, 75% of patients had cludes accumulation of mononuclear
mia. No evidence of malignancy was multisystem involvement. In infants, inflammatory cells in the target or-
found. sarcoidosis typically presents with gan, following which macrophages
The boy’s pulmonary function skin involvement (including ery- aggregate and differentiate into epi-
tests (PFTs) showed a restrictive pat- thema nodosum) and joint and eye thelioid and multinucleated cells. Ac-
tern, including a forced expiratory disease. In older children, sarcoidosis tivated lymphocytes and macro-
volume in 1 second (FEV1) and tends to affect the pulmonary system, phages within the granuloma release
forced vital capacity (FVC) at 58% of lymphatics, and eyes (uveitis) more mediators, including interleukin-1
predicted value. The FEV1/FVC ra- frequently. (IL-1), IL-2, interferon, and other
tio was 100%, correlating with his Clinical features of sarcoidosis cytokines that promote and maintain
restrictive pattern. His angiotensin- vary and depend on the specific or- the granulomatous lesion. During
converting enzyme (ACE) level was gan systems involved. This patient active disease, lymphocytes in the
elevated at 196 IU/L (normal, 18 to displayed the classic findings of a re- granulomas are predominantly
90 IU/L), and a bronchial biopsy strictive pattern on PFTs, although helper T (CD4) lymphocytes.
obtained during bronchoscopy he had no eye findings typical of uve- Three processes have been identi-
showed multiple noncaseating coa- itis or rash characteristic of cutaneous fied in the initiation of sarcoidosis:
lescing granulomas suggestive of sar- sarcoidosis. exposure to antigen, cellular immu-
coidosis. He was started on oral Sarcoidosis can be staged by the nity directed against the antigen me-
prednisone (1 mg/kg per day). He following criteria: Stage I is defined diated through antigen-presenting
required a short stay in the intensive as the presence of hilar lymphade- cells and antigen-specific T lympho-
care unit to control his hypercalcemia nopathy on radiographs without pa- cytes, and the appearance of immune
(ionized calcium level rose to renchymal infiltrates, stage II in- cells that produce a nonspecific im-
7.9 mg/dL [2 mmol/L]) and oxy- cludes pulmonary infiltrates, and mune response. This extensive in-
gen requirement. stage III is defined as infiltrates with- flammation often results in fibrosis,
Repeat PFTs showed significant out lymphadenopathy. as with pulmonary sarcoidosis.
improvement less than 1 week after The pathogenesis of sarcoidosis
the initiation of corticosteroids. The remains obscure, primarily because Differential Diagnosis
FVC and FEV1 improved to 72% and of the variety of manifestations it can Sarcoidosis is a diagnosis of exclu-
68% of predicted values, respectively, produce. Both environmental and sion. Because no specific test con-
and the FEV1/FVC ratio was 94% of genetic factors have been linked to firms the diagnosis, other causes of
its predicted value. He was dis- the condition. Infectious agents, granulomatous disease must be ruled
charged from the hospital on hospital chemicals, drugs, autoimmune fac- out. Tuberculosis, chronic beryllium
day 11 and instructed to follow up tors, and genetic factors all have been disease, hypersensitivity pneumoni-
with pediatric pulmonology and pe- explored as potential causes of the tis, pulmonary alveolar proteinosis,
diatric rheumatology. He will con- disease. The current belief is that sar- Wegener granulomatosis, and other
tinue daily steroids while having his coidosis represents the exposure of a conditions must be considered when
PFTs monitored serially. The goal is genetically susceptible individual to a evaluating a patient who has granu-
to taper his maintenance steroid dos- specific environmental agent that lomatous disease with diffuse pulmo-
ing to an every-other-day regimen. triggers an exaggerated cellular im- nary involvement. Clues to the diag-
Pulse high-dose steroids along with mune response. Sarcoidosis most nosis of sarcoidosis include an
methotrexate was considered, but it commonly affects young adults and elevated ACE level, hypercalcemia
was decided to pursue the more clas- in the United States occurs more fre- (33% of patients), uveitis, elevated
sic treatment of corticosteroids quently in African-Americans. ESR, hyperproteinemia, eosino-
dosed conventionally. philia, and a diffuse pulmonary pro-
Pathologic Findings cess.
The Condition Sarcoidosis is characterized by a fo-
Sarcoidosis is a generalized inflam- cused, overwhelming inflammatory Treatment
matory process that most often af- response to an unknown antigen. The mainstay of treatment is oral cor-
fects the lungs but can involve almost The noncaseating granuloma is the ticosteroids, with the dose and dura-
any body system, including the skin, classic pathologic finding. The tion of treatment tailored to the in-
430 Pediatrics in Review Vol.27 No.11 November 2006
index of suspicion
dividual because absolute guidelines roids for prevention of permanent skin involvement carry a guarded
regarding steroid use are not avail- damage in suspected cases of uveitis; prognosis; most experience a chronic
able. Initial dosing is 1 mg/kg per hydroxychloroquine for cutaneous course and multiple irreversible se-
day and may be tapered according to sarcoidosis unresponsive to steroids quelae. Determining the prognosis
clinical response. Duration of ther- and for hypercalcemia; and implant- for a patient who has sarcoidosis
apy is based on an individual patient’s able defibrillators for cardiac se- must involve screening for multior-
response to therapy. Corticosteroid quelae. In general, therapy for a pa- gan disease, using scales such as the
therapy has been associated with im- tient who has sarcoidosis requires a ACCESS Organ Assessment Instru-
provements in dyspnea, PFTs, and multidisciplinary approach, which ment, (1) as well as determining the
the appearance of the chest radio- can involve primary care clinicians, effect of pulmonary, systemic, and
graph as well as suppression of gran- pulmonologists, rheumatologists, der- cutaneous symptoms on the patient’s
uloma formation. However, evi- matologists, ophthalmologists, cardi- perceived quality of life.
dence that corticosteroids can ologists, and neurologists.
prevent long-term pulmonary fibro-
Lessons For The Clinician
sis does not exist, and adverse effects Prognosis
Sarcoidosis remains an unusual dis-
often limit their usefulness. More than 60% of patients afflicted
ease in children but must be consid-
Second-line therapy is with im- with sarcoidosis have a good progno-
ered when evaluating a patient who
munosuppressants and cytotoxic sis; they do not require therapy and
has a diffuse pulmonary process that
agents, including methotrexate, hy- their disease remits spontaneously.
cannot be explained by other causes.
droxycholorquine, azothioprine, and Poor prognostic indicators include
Sarcoidosis can present with involve-
antitumor necrosis factor drugs (en- advanced staging by chest radio-
ment of almost any organ system but
tanercept and infliximab). Of these graphs, cardiac or neurologic disease,
most commonly involves the lungs,
agents, methotrexate is the best stud- and pulmonary hypertension. Of
lymphatics, eyes, and skin in chil-
ied and has been found to reduce the these, the initial stage is the most
dren. Consultation with a pediatric
need for corticosteroid therapy as important prognostic factor: 95% of
pulmonologist, rheumatologist, and
well as to delay the decline in PFT patients who have stage I disease are
ophthalmologist should be consid-
parameters, such as the FEV1 and asymptomatic at 5 years compared
ered when the diagnosis is a possibil-
diffusing capacity of carbon monox- with 25% of patients who have stage
ity. (Michael Wolf, MD, Sibel Algon,
ide. One limitation of methotrexate III disease. In general, asymptomatic
MD, Bristol Myers Squibb Children’s
is hepatotoxicity, which is minimized patients undergo spontaneous reso-
Hospital/UMDNJ - Robert Wood
when folic acid supplementation is lution of their disease, while symp-
Johnson University Hospital, New
provided. tomatic patients tend toward multi-
Brunswick, NJ)
Other therapies are useful in treat- system involvement and chronic
ing specific symptoms of sarcoidosis: disease, with irreversible sequelae in
nonsteroidal anti-inflammatory drugs up to 20% of cases.
for erythema nodosum, joint in- Sarcoidosis in children usually car-
Reference
1. ACCESS Research Group. Design of a
volvement, and fevers; topical corti- ries a better prognosis than in adults. case control etiologic study of sarcoidosis
costeroids for mild cases of erythema However, children who have early- (ACCESS). J Clin Epidemiol. 1999;52:
nodosum; ophthalmic corticoste- onset sarcoidosis with eye, joint, or 1173–1186
Pediatrics in Review Vol.27 No.11 November 2006 431
technical tip
Technical Tip
Corneal Abrasions
Ann U. Stout, MD* sues of the body, so discomfort may external. The upper lid can be everted
range from mild to severe, depending over a cotton-tip applicator or a finger-
on the size of the defect. Symptoms tip to examine the tarsus. Abrasions
include photophobia, tearing, and in- that involve the entire cornea, such as
termittent sharp pain due to ciliary after chemical exposure, may be over-
Author Disclosure
body spasm. Physical findings include looked because no normal epithelium
Dr Stout did not disclose any irritability, blurry vision, conjunctival remains for comparison.
financial relationships relevant to injection, blepharospasm, irregular red Corneal abrasions heal rapidly, often
this tip. reflex, dulled corneal light reflex, and within 24 hours, although larger de-
fluorescein staining of the epithelial fects may take longer. Antibiotic oint-
defect. ment may help lubricate the surface
The father of a healthy 16-month-old Examination is facilitated by the use until healing occurs, but aminoglyco-
boy brings him in to “check his eye.” The of topical anesthetics (proparacaine or sides should be avoided because they
evening before, which had been rather tetracaine), which provide temporary may delay epithelial regrowth. The
windy, he had taken the child for a walk pain relief. Fluorescein helps define the chance of secondary infection is low,
in the stroller. During the walk, the boy size of the defect, although large de- unless foreign matter is retained.
began fussing and rubbing one eye. The fects may be seen without any dye. Therefore, a course of topical antibiot-
father noticed that the eye was watery Fluorescein strips can be moistened and ics is not requisite. Tight patching with
and red but could not see anything in touched to the lower fornix to apply two eye pads may help with comfort by
the eye. He gave the boy some acet- the stain or combination anesthetic/ blocking light and preventing the irri-
aminophen, and he slept well. Today, fluorescein drops can be used. The dye tation of repetitive blinking. The patch
however, the eye is still teary and stains the exposed corneal stroma, but must be tight enough to prevent inad-
irritated, and the boy is fussy. You washes off of intact epithelium. The vertent lid opening under the patch,
inspect the eye and find no foreign yellow dye is visible with regular white which could result in subsequent addi-
body. light, although blue or ultraviolet light tional abrasions from the patch mate-
Fluorescein staining viewed with a (Wood lamp) may make it more visible rial. Patching is not believed to speed
Wood lamp shows a 2-mm corneal and be better tolerated by a child who healing unless the defect encompasses
abrasion and fine linear vertical streak has photophobia. more than 75% of the corneal surface
defects. You suspect a hidden foreign The conjunctival cul de sac and area. Most younger children dislike the
body because the abrasion probably upper tarsus should be examined to rule patch, so it can be applied in the office
occurred yesterday and should have out retained foreign bodies, which may
healed overnight. Upon eversion of the cause persistent abrasions, unless the
upper lid, you see a small black particle cause of the abrasion is known to be
stuck to the tarsus that is removed
easily with a cotton swab (Fig. 1). You
prescribe analgesics as needed, topical
antibiotic ointment, and reassurance.
The next day, the father reports that his
son’s eye is back to normal.
Corneal abrasions (Fig. 2) occur of-
ten in children of all ages. The cornea is
one of the most richly innervated tis-
*Casey Eye Institute, Oregon Health & Science
University, Portland, Ore. Figure 1. Foreign body in the eye. Figure 2. Corneal abrasion.
Pediatrics in Review Vol.27 No.11 November 2006 433
in brief
and removed by the family if it is poorly Topical nonsteroidal drops (ketorolac) tial healing. During the night, the lid
tolerated. The family should not reapply may provide additional relief, but may sticks to the new epithelial cells and
it because it might be too tight or not delay healing. Topical anesthetics pulls them loose upon awakening.
tight enough. NEVER should be dispensed because These small abrasions are symptomatic
Over-the-counter analgesics or co- they not only retard healing but can upon awakening and often improve
deine may be used for pain manage- lead to corneal melting and perforation. throughout the day. Nightly lubrication
ment if needed. The pain of an abrasion Most small abrasions heal overnight. with ointment sometimes can break
should not be underestimated, and The patient can be seen the next day as this cycle. Patients who have nonheal-
treatment should be tailored to the needed or feasible. If symptoms and ing abrasions should be referred
child’s comfort level. Pupillary dilation signs have resolved, it can be assumed promptly for additional evaluation be-
with a cycloplegic agent (tropicamide that the abrasion has healed. A small cause such abrasions can be due to
1% or cyclopentolate 1%) may help to group of patients are at risk of devel- secondary infections, occult foreign
block ciliary spasm and relieve pain. oping recurrent erosions from poor ini- bodies, or lacerations.
In Brief
Ampicillin and Amoxicillin
Zainab A. Malik, MD cians. Pediatrics. 2004;113: do not produce beta-lactamase. These
Nathan Litman, MD 1451–1465 agents are not active against Pseudo-
Children’s Hospital at Montefiore Management of Sinusitis. Subcommit- monas sp and are hydrolyzed by beta-
tee on Management of Sinusitis and
Bronx, NY lactamases, making them ineffective
Committee on Quality Improvement.
American Academy of Pediatrics. against beta-lactamase-producing strains
Pediatrics. 2001;108:798 – 808 of bacteria.
Author Disclosure
Ampicillin is effective in treating
Drs Malik, Litman, and Adam did not upper and lower respiratory tract infec-
disclose any financial relationships Ampicillin and amoxicillin are amino-
tions caused by Streptococcus pneu-
penicillins derived from the penicillin
relevant to this In Brief. moniae, beta-hemolytic streptococci, and
nucleus. Their basic structure consists
nonbeta-lactamase-producing strains of
of the beta-lactam ring and a side
Haemophilus influenzae. It also is ef-
The Use of Antibiotics. Kucers A. In: chain. The ring structure confers anti-
fective in the treatment of meningitis
Crowe KS, Grayson ML, Hoy J, eds. microbial activity, and the side chain
determines the antibacterial spectrum caused by group B streptococci, Listeria
The Use of Antibiotics: A Clinical
and pharmacologic properties. The an- monocytogenes, N meningitidis, and all
Review of Antibacterial, Antifungal
and Antiviral Drugs. 5th ed. Oxford, tibacterial activity of aminopenicillins except highly resistant strains of S
United Kingdom: Butterworth-Heine- is similar to that of other penicillins via pneumoniae. Ampicillin previously was
mann Publishing; 1997:108 –143, inhibition of bacterial cell wall synthe- a first-line agent for treating urinary
192–208 sis. Penicillin-sensitive reactions in tract infections (UTIs) caused by Esch-
Penicillins. Chambers HF. In: Mandell bacterial cell wall synthesis are cata- erichia coli and gastroenteritis caused
GL, Bennett JE, Dolin R, eds. Princi- lyzed by a class of proteins called by Salmonella enterica or Shigella sp.
ples and Practice of Infectious Dis- penicillin-binding proteins (PBPs), However, due to the rising prevalence
eases. Vol 1. 6th ed. Philadelphia, Pa: of beta-lactamase-producing strains of
which are inhibited by beta-lactam
Elsevier Churchill Livingstone; 2005:
antibiotics. these organisms, ampicillin no longer is
281–293
The antibacterial spectrum of amino- the agent of choice for UTIs unless
Diagnosis and Management of Acute
Otitis Media. Subcommittee on penicillins includes nonbeta-lactamase- susceptibility has been documented.
Management of Acute Otitis Media. producing gram-positive cocci, anaer- The in vitro activity of amoxicillin is
American Academy of Pediatrics and obes, and gram-negative cocci, including similar to that of ampicillin. Ampicillin
American Academy of Family Physi- Neisseria and Enterobacteriacae that usually is given intravenously (IV) or
434 Pediatrics in Review Vol.27 No.11 November 2006
in brief
intramuscularly (IM), whereas amoxicil- joint effusions, ascitic fluid, and para- and food does not alter its absorption.
lin is the preferred oral agent because it pneumonic effusions. Very low concen- Almost 60% of an oral dose of amoxi-
is less likely to cause diarrhea and can trations of ampicillin can be detected in cillin is excreted unchanged in urine
be administered less frequently than normal cerebrospinal fluid, but higher within the first 6 hours. It has a tissue
oral ampicillin. Amoxicillin is indicated levels are achieved in patients who distribution similar to that of ampicil-
in the treatment of otitis media, sinus- have bacterial meningitis due to ongo- lin, and tissue levels are 40% of serum
itis, pneumonia, and susceptible UTIs. ing meningeal inflammation. levels. Because amoxicillin achieves
Among the oral penicillins and ceph- The serum half-life of ampicillin de- high levels in the gastric mucosa, it is a
alosporins, amoxicillin can achieve clines with increasing postnatal age. In good antibiotic for treating Helicobac-
therapeutic minimum inhibitory con- neonates 2 to 7 days old, the serum ter pylori infections in combination
centrations in body tissues for nonmen- half-life is 4 hours; in 8- to 14-day-old with other agents. Oral amoxicillin is
ingeal infections caused by penicillin- neonates, it is 2.8 hours; and in 15- to not indicated for treating central ner-
resistant pneumococci, except highly 30-day-old neonates, it is 1.7 hours. In vous system infections.
resistant strains. Amoxicillin is not use- older children and adults, ampicillin has Amoxicillin is relatively nontoxic
ful in the treatment of shigellosis be- a serum half-life of 1 hour. After par- and may be given in the usual recom-
cause it is well absorbed in the small enteral administration, 75% of the dose mended dose to patients who have mild
intestine. Oral ampicillin is indicated for is excreted in the urine and 0.1% of the renal failure. The dose should be re-
this purpose; its poor intestinal absorp- dose is excreted unchanged in bile. duced for patients whose renal failure
tion allows significant levels of the Because high concentrations of ampi- is moderate to severe. Amoxicillin is the
antibiotic to reach the site of infection cillin are excreted in the urine, it was an drug of choice for treating acute bac-
in the large intestine. agent of choice for UTIs prior to the terial sinusitis and acute otitis media.
Ampicillin can be given IV or IM in emergence of microbial resistance. Factors that justify its use as a first-line
the form of its sodium salt. For neo- The major adverse effects associated agent include its narrow antimicrobial
nates weighing more than 2,000 g and with ampicillin use are rashes, which spectrum, pleasant taste, low cost, ac-
younger than 7 days old, a dose of tend to occur more commonly than tivity against susceptible and interme-
25 mg/kg every 8 hours is recom- with other penicillins (7.7% versus diately resistant pneumococci, and ac-
mended for mild-to-moderate infec- 2.75%). Ampicillin rashes may be urti- ceptable safety profile in children.
tions. With serious infections such as carial or macular, resembling measles There is a high prevalence of beta-
meningitis, the dose should be in- or rubella. The macular rashes usually lactamase-producing strains of H influ-
creased to 50 mg/kg every 8 hours. appear 4 to 5 days after therapy has enzae and Moraxella catarrhalis in up-
Neonates older than 7 days and weigh- begun, without any other associated per respiratory tract isolates in the
ing more than 2,000 g who have mild signs of allergy, and often subside with United States, making them resistant to
infections can receive a dose of ongoing treatment. The nonurticarial amoxicillin. Of the S pneumoniae iso-
25 mg/kg every 6 hours; for meningitis, rashes do not indicate true ampicillin lates from the upper respiratory tract,
the dose should be increased to hypersensitivity. Parenteral ampicillin an average of 30% are resistant to
200 mg/kg per day divided every therapy also can cause nausea and penicillin. Some 50% of these organ-
6 hours. For older infants and children, diarrhea, which are more common in isms are highly resistant, reflected in
doses of 100 to 400 mg/kg per day, younger children. Ampicillin and their lack of response to standard-dose
divided every 4 to 6 hours, are recom- amoxicillin can both be responsible for amoxicillin therapy. Penicillin resis-
mended. Because ampicillin is relatively Clostridia difficile-associated pseudo- tance among S pneumoniae results not
nontoxic, dose adjustment is not imper- membranous colitis. Very large doses from the production of an enzyme, but
ative in mild-to-moderate renal failure, that achieve serum levels of 800 mcg/mL from an alteration in PBPs on the bac-
although it may be required for patients may cause central nervous system toxic- terial cell wall, which confers resistance
who have severe renal dysfunction. ity, resulting in convulsions. to penicillins and cephalosporins.
Ampicillin is well distributed Amoxicillin is available in the trihy- Conventional doses of amoxicillin
throughout the body. Although the drate preparation for oral use. The stan- (45 mg/kg per day) are effective against
peak interstitial tissue concentrations dard dose is 45 mg/kg per day in two all susceptible strains of S pneumoniae
are lower than those achieved in serum, divided doses or 80 to 90 mg/kg per day and most strains that are intermediate
the drug persists in the interstitium for in two divided doses for indications in resistance to penicillin. Highly resis-
a longer period of time. It achieves that require high-dose amoxicillin. It is tant strains are not susceptible to con-
therapeutic concentrations in septic well absorbed after oral administration, ventional doses of amoxicillin. High-
Pediatrics in Review Vol.27 No.11 November 2006 435
in brief
dose amoxicillin (80 to 90 mg/kg per otics in the preceding 3 months, partic- cause nausea and diarrhea, although
day) achieves high middle ear and sinus ularly among children younger than 2 less commonly than ampicillin.
fluid levels, making it effective against years of age.
all intermediately resistant strains and Amoxicillin and ampicillin are cross-
some, but not all, highly resistant allergenic with other penicillins and are Comment: Despite newer and newer
strains. In practice, the response rate to contraindicated in penicillin-allergic (and more expensive) antimicrobial
high-dose amoxicillin among children patients. Amoxicillin generally is well agents, amoxicillin remains the drug of
who have acute otitis media is approx- tolerated, although it has a propensity choice for both otitis media and sinus-
imately 80%. to cause rashes and results in a morbil- itis in most children. It’s nice when
Risk factors for the presence of in- liform rash if given to a patient acutely oldies are still goodies.
termediate or highly resistant S pneu- infected with Epstein-Barr virus. The
moniae necessitating the use of high- maculopapular eruptions produced by
dose amoxicillin include child care amoxicillin are similar to those seen Henry M. Adam, MD
attendance and having received antibi- with ampicillin. Amoxicillin also may Editor, In Brief
In Brief
Cocaine
Christine Rizkalla, MD TOX-ACLS: Toxicologic-oriented ease hunger and thirst, and to improve
Young-Jin Sue, MD Advanced Cardiac Life Support. the stamina required for daily labors
Children’s Hospital at Montefiore Albertson T, Dawson A, de Latorre F, and life at great altitudes. Spanish col-
et al. Ann Emerg Med. 2001;
Bronx, NY onists of the region introduced the leaf
37(4 suppl):S78 –S90
Cocaine, Amphetamines and Other to Europe, and the pure and far more
Sympathomimetics. Rao R, Hoffman potent chemical, cocaine, ultimately
Author Disclosure
R. In: Marx JA, Hockberger RS, Walls was extracted. The mid-1800s saw the
Drs Rizkalla, Sue, and Adam did not RM, eds. Rosen’s Emergency Medi- production of coca-infused wines and
disclose any financial relationships cine: Concepts and Clinical Practice. tonics. Early surgeons discovered its
relevant to this In Brief. 5th ed. St. Louis, Mo: Mosby; 2002: utility for local anesthesia. Sigmund
2386 –2392
Freud praised the drug for its multiple
Body Packing: The Internal Conceal-
ment of Drugs. Traub S, Hoffman R, medicinal uses. In 1886, Dr John Pem-
History of Cocaine. Petersen RC. NIDA berton produced a new beverage
Res Monogr. 1977;13:17–34 Nelson L. N Engl J Med. 2003;349:
2519 –2526 named Coca Cola, combining coca and
Cocaine: History, Use, Abuse. Karch S.
caffeine from the African kola nut
J R Soc Med. 1999;92:393–398
Cocaine Use: 2002–2003. The NSDUH According to one legend, before it was plant, touting it as tonic for multiple
Report. 2005. Available at: http:// a plant, coca was a beautiful woman, ailments and nervous disorders, partic-
www.oas.samhsa.gov/2k5/cocaine/ executed for adultery. Evidence of hu- ularly for the elderly. Gradually, more
cocaine.htm mans consuming Erythroxylon coca, a products contained greater amounts,
Intersecting Epidemics—Crack Cocaine South American shrub from which co- and consumption increased. Sir Arthur
Use and HIV Infection among Inner- caine (benzoylmethylecgonine) is de- Conan Doyle described his celebrated
city Young Adults. Edlin BR, Irwin fictional detective Sherlock Holmes us-
rived, dates to more than 1,000 years
KL, Faruque S, et al. Multicenter
ago. Regarded as divine in the northern ing cocaine when occupied by boring
Crack Cocaine and HIV Infection
Andes of Peru and Bolivia, cocaine cases. By the advent of the 20th cen-
Study Team. N Engl J Med. 1994;
331:1422–1427 played a role in religious ceremonies tury, increasing prevalence and nonme-
Cocaine and the Critical Care Chal- and inspired colorful mythology regard- dicinal use of pure cocaine brought
lenge. Shanti C, Lucas C. Crit Care ing its origin. Chewing coca leaves was with it the awareness of its toxic and
Med. 2003;31:1851–1859 promoted for its healing powers, to addictive potential. Beginning with the
436 Pediatrics in Review Vol.27 No.11 November 2006
in brief
Harrison Act of 1914, the United States seizure, pulmonary hemorrhage, gastro- such complications. Potentially life-
government passed legislation to at- intestinal ischemia, rhabdomyolysis, threatening hyperthermia results from
tempt to control its availability, but and renal failure. Use in pregnancy may agitation, increased motor tone, and
public demand remained. lead to placental abruption or fetal vasoconstriction, interrupting the
Far from myth and legend, cocaine demise. Behavioral manifestations of body’s cooling mechanisms. Once iden-
now is popularly known as bazooka, this sympathetic overstimulation in- tified, hyperthermia must be addressed
white lady, Charlie, snow, tornado, clude euphoria, confidence, agitation, emergently with: benzodiazepines to
kryptonite, dust, bones, sugar, and aggression, and hallucinations (“coke decrease agitation; paralysis and airway
blow, among other names. Estimates in bugs”). stabilization if indicated; IV access for
both 2002 and 2003 were that more Cocaine blocks sodium transport aggressive fluid management; and rapid
than 5.9 million people in the United across cell membranes, slowing nerve cooling with ice.
States older than age 12 years (2.5% of impulses, which accounts both for its The clinician also must monitor lev-
the population) had used cocaine anesthetic properties and for its poten- els of creatine kinase, electrolytes, cre-
within the past 12 months, primarily tial to induce fatal ventricular arrhyth- atinine, coagulation parameters, and
within the 18- to 25-year-old group. mias and cardiac arrest. IV use carries urine myoglobin because rhabdomyoly-
Cocaine is abused by several routes. the additional risks of local infection, sis may be an associated complication.
Water-soluble cocaine hydrochloride is sepsis, and endocarditis. Human immu- A direct-acting alpha-adrenergic an-
snorted as a powder or injected as an nodeficiency virus transmission is an tagonist such as phentolamine and a
aqueous solution. Alkaloid preparations additional risk of IV drug use, both from vasodilator, usually nitroprusside, are
are smoked as “free-base” or as the needle-sharing and because high-risk used to treat critical hypertension. Beta
precipitated crystal form known as sexual encounters are associated with blockers should be avoided because re-
crack. As a base, cocaine is highly drug-seeking behavior. sultant unopposed alpha-adrenergic
purified, heat-stable, and lipid-soluble, Chronic use of cocaine is associated stimulation may exacerbate the hyper-
thereby readily crossing the blood-brain with cachexia, poor nutrition, and tension. Computed tomography (CT)
barrier and yielding an intense and “crack dancing” (choreoathetotic move- scanning of the brain and lumbar punc-
immediate “high.” Both smoking and ments from decreased dopamine ture should be strongly considered for
intravenous (IV) injection produce a stores). Upregulation of dopaminergic patients who have persistent headache
high within seconds to minutes that receptors exacerbates tolerance as well or altered mental status.
lasts 15 to 30 minutes unless repeated as the drug craving and dysphoria that Evaluation of chest pain in associa-
hits are delivered. The effects of insuf- follow each high. With greater intake tion with cocaine use requires radio-
flated cocaine peak at 20 to 30 minutes needed to achieve the same effects, graphs of the chest (for pneumothorax,
(due to local vasoconstriction, which cocaine users increase their potential widened mediastinum, and pneumonia),
slows its absorption) and last approxi- for morbidity and mortality. electrocardiography (ECG), measure-
mately 1 hour. Cocaine may be adulter- Cocaine users may not be forthcom- ment of cardiac enzymes and electro-
ated to augment its mass (eg, with ing about their drug taking. Urine lytes, a complete blood count, and
sugars or talc) or to enhance its effects screening is widely available, employing blood cultures. Acute coronary syndromes
(eg, with heroin— known as a a highly specific immunoassay for the due to cocaine should be managed ini-
“speedball”—phencyclidine, lidocaine, metabolite benzoylecgonine, which is tially with nitrates and benzodiazepines,
or strychnine). Use with alcohol pro- excreted for 24 to 48 hours. However, with use of alpha-adrenergic antagonists
duces the metabolite cocaethylene, depending on the chronicity of use, considered in refractory cases. Sodium
which may augment its toxicity. urine may remain positive for several bicarbonate is appropriate for treating
The physiologic effects of cocaine days. the sodium channel blockade that re-
result from the release of norepineph- As with all medical emergencies, sults in ventricular dysrhythmias, man-
rine from adrenergic nerve terminals individuals who present with symptoms ifested as a widened QRS interval on
and from inhibited reuptake of dopamine, of toxicity should be evaluated for air- ECG. Class 1A and 1C antidysrhythmic
epinephrine, serotonin and norepineph- way stability. The most rapidly fatal agents generally are contraindicated in
rine. Sympathetic overstimulation man- complications in cocaine use are re- such situations because exacerbation of
ifests as mydriasis, diaphoresis, tachy- lated to hyperthermia, hypertension, sodium channel blockade may ensue.
cardia, hypertension, and hyperthermia. and cardiac dysrhythmias. Benzodiaz- A unique set of problems arises with
This may be followed by the complica- epines and aggressive external cooling individuals who have ingested densely
tions of myocardial infarction, stroke, are the foundation of management of contained, well-sealed packets of the
Pediatrics in Review Vol.27 No.11 November 2006 437
in brief
drug for transport (body packers) or bodies surrounded by gas. Bowel perfo- exposures, cocaine continues to present
who have hastily swallowed poorly ration is an additional concern. Because a complex and sometimes fatal public
sealed aliquots to conceal them from of the potential for lethal overdosing, a health challenge that includes the pe-
law enforcement officers (body positive urine assay accompanied by diatric population. Familiarity with the
stuffers). Body packers may harbor up symptoms of cocaine toxicity in such manifestations and management of co-
to 100 packages, each containing a individuals should prompt rapid surgi- caine intoxication is imperative for
lethal quantity of the drug. Body cal decontamination, with treatment of practitioners who work with children
stuffers, while concealing a lesser associated toxicity as described previ- and adolescents.
amount of drug, may be at greater risk ously. Stable individuals should be
for toxicity from rupture of poorly se- managed with whole bowel irrigation, Comment: So, at least initially,
cured packets. Plain radiographs may using polyethylene glycol to facilitate there really was a difference between
reveal air trapped between the wrap- gut emptying, and observation until Coke and Pepsi!
pers (often condoms) used for packag- passage of all packages.
ing (“double-condom sign”), and con- With considerable numbers of ado- Henry M. Adam, MD
trast CT scans may demonstrate foreign lescent users and accidental toddler Editor, In Brief
Correction
For question #11 on page 345 in the September 2006 issue of Pediatrics in Review,
the answer should be D rather than E.
438 Pediatrics in Review Vol.27 No.11 November 2006
Pediatrics in Review Vol.27 No.11 November 2006 439
visual diagnosis
A Child Who Has Acute
Onset of Unusual Skin
Lesions and Edema
Ceyda Acun, MD,* Gonca Ustundag, MD,* Ayhan Sogut, MD,*
Rafet Koca, MD,† Gamze Numanoglu, MD‡
Presentation
A 13-month-old boy presents to the emergency depart-
ment with a 1-day history of rash on his face, medial
thighs, and upper trunk and swelling of his face, ears,
hands, and feet. He has a 3-day history of an upper
respiratory tract infection. There is no recent history of
immunization or drug intake.
The physical examination reveals an alert child who
has a widespread rash over his peroral area, chin, cheeks,
and ears, with sparing of the mucous membranes (Figs.
1, 2). His vital signs are appropriate for his age. The rash
appears in a rosette pattern of 1 to 2-cm diameter,
purplish-red, slightly raised macules. A milder rash ap-
pears on his medial thighs and upper trunk. Both his face
and ears are significantly swollen, and the flexor surfaces
Figure 1. Purplish-red, slightly raised macules on the face and of the hands and feet are mildly swollen. The patient is
trunk. admitted for observation and evaluation.
Over the next 3 days, the rash spreads to his arms and
legs (Figs. 3, 4). However, apart from a transient mild
fever, the child appears well, having no obvious systemic
symptoms.
The laboratory examination reveals a normal com-
plete blood count, serum immunoglobulins, C3 and C4
levels, circulating immune complexes, antistreptolysin
titers, coagulation studies, urinalysis, renal function tests,
and liver function tests. Stool samples are negative for
ova and parasites, and blood cultures show no growth.
A skin biopsy reveals the diagnosis.
Figure 2. Purplish-red, slightly raised macules on the face and
ear.
Author Disclosure
Drs Acun, Ustundag, Sogut, Koca, and Numanoglu did not
disclose any financial relationships relevant to this case.
*Department of Pediatrics.
†
Department of Dermatology.
‡
Department of Pathology, Karaelmas University, School of Medicine, Zonguldak,
Turkey.
Pediatrics in Review Vol.27 No.11 November 2006 e71
visual diagnosis
Figure 3. Rash over extremities.
Figure 4. Rash over legs and buttocks.
e72 Pediatrics in Review Vol.27 No.11 November 2006
visual diagnosis
Diagnosis: Acute Hemorrhagic Edema of Clinical Features
Infancy The clinical hallmark of AHEI is the sudden appearance
The patient has acute hemorrhagic edema of infancy and spread of a purpuric rash and edema over the face and
(AHEI), a diagnosis based on the clinical presentation extremities in an otherwise healthy infant. Fever may be
and the skin biopsy demonstration of leukocytoclastic present. The rash first appears as red macules or urticarial
vasculitis. lesions that dramatically evolve into large (1 to 5 cm diam-
AHEI is a rare, benign form of leukocytoclastic vas- eter) ecchymotic papules, characteristically arranged in a
culitis that occurs in children younger than 2 years of age. cluster of circular lesions (sometimes described as a rosette
Originally reported by Snow in 1913, case reports in the or cockade pattern). The face, ears, scrotum, and extremi-
European literature have labeled this disorder Finkelstein ties are affected commonly, with sparing of the trunk and
disease, Seidlmayer syndrome, medallion-like purpura, mucous membranes. Edema develops early in the course of
and infantile postinfectious iris-like purpura and edema. the disorder and appears over the face, scalp, the dorsa of
the hands and feet, and the proximal extremities. Approxi-
mately 50% of patients complain of arthralgias.
Epidemiology Complications are rare and include purpuric lesion
Although uncommon, AHEI appears throughout the necrosis (especially of the ears) and gastrointestinal vas-
world. The disease frequency is unknown, and no racial culitis followed by intussusception. Transitory renal
predilection is reported. AHEI may be slightly more problems (microscopic hematuria, mild proteinuria)
common among male infants than among female infants. have been described infrequently, with spontaneous re-
Affected children are usually 4 to 24 months of age. covery within days to 3 weeks.
Spontaneous and complete healing of AHEI occurs
within 1 to 3 weeks, but relapses may occur up to 15
Cause months after initial presentation. Only necrotic areas may
The cause of AHEI is unknown, although in approxi- leave a scar.
mately 75% cases, AHEI is preceded by viral infection Suggested diagnostic criteria for AHEI include:
(usually upper respiratory tract infection), bacterial infec- ● Patient age younger than 2 years
tion (streptococcal pharyngitis, pulmonary tuberculosis, ● Purpuric or ecchymotic targetlike lesions, with
bronchopneumonia, urinary tract infection), immuniza- edema of the face, ears, and extremities, with or
tion (measles, diphtheria-pertussis-tetanus), or drug ex- without mucosal involvement
posure (penicillin, cephalosporins, trimethoprim- ● Lack of systemic disease or visceral involvement
sulfamethoxazole, acetaminophen). AHEI may be ● Spontaneous recovery within a few days or weeks
immune-mediated, but only a few cases demonstrate
immune complexes in biopsy specimens.
Laboratory Features
Laboratory findings are nonspecific and include mild
leukocytosis, lymphocytosis, thrombocytosis, and in
some cases, eosinophilia. Immune complexes may be
Definitions present in some cases, but serum complement and im-
munglobulin (Ig) values generally are within normal limits.
Leukocytoclastic vasculitis—A histopathologic term for
Skin biopsy demonstrates fibrinoid necrosis, pupura, neu-
small-vessel vasculitis, also known as hypersensitivity
trophil and mononuclear cell infiltration, and leukocytocla-
vasculitis, allergic vasculitis, and allergic angiitis.
sis. Direct immunoflourescence may reveal vascular depos-
Deposition of immune complexes along the
its of C1q, C3, and fibrinogen. One series of case reports
postcapillary venules activates the complement
found that 80% of patients had vessel deposits of IgM, 30%
cascade, leading to neutrophil migration, vessel wall
had IgA, 30% had IgE, and 20% had IgG.
destruction, fluid leakage, and red blood cell
extravasation. Palpable purpura is the most sensitive
clinical sign for leukocytoclastic vasculitis. Differential Diagnosis
Purpura—A red-purple, nonblanchable discloration, AHEI is similar to Henoch-Schönlein purpura (HSP) in
greater than 0.5 cm in diameter, that represents presentation. Some clinicians postulate that AHEI is a
hemorrhage into the skin. variant of HSP. However, HSP generally affects children
ages 3 to 6 years and, unlike AHEI, presents with sys-
Pediatrics in Review Vol.27 No.11 November 2006 e73
visual diagnosis
temic symptoms such as abdominal pain and vomiting. Summary
Frequently, renal disease (proteinuria, hematuria, tran- AHEI is a benign variant of leukocytoclastic vasculitis
sient azotemia) also is present in HSP. Most cases of HSP that occurs in children younger than 2 years of age.
demonstrate vascular IgA deposition; only a minority of Respiratory tract infection, drug intake, or immunization
cases of AHEI do so. Furthermore, although AHEI may frequently precedes AHEI. Striking clinical features in-
demonstrate C1q perivascular deposition, HSP does not. clude acute appearance of the cutaneous lesions in oth-
Other important differential diagnoses include me- erwise healthy young infants and children, lack of visceral
ningococcemia, erythema multiforme, urticaria with involvement, and self-limited progression. Laboratory
hemorrhage, Kawasaki disease, purpura due to septice- tests, except for punch biopsy of the skin lesions, are non-
mia, and drug eruption. diagnostic. Differential diagnoses include HSP and other
potentially serious disorders such as meningococcemia, er-
Management
ythema multiforme, and Kawasaki disease. No effective
There is no specific treatment for AHEI. Spontaneous,
therapy exists for AHEI, and treatment is supportive.
complete resolution without complications usually oc-
curs within 5 to 14 days, but the disease may endure as
long as 35 days. Antibiotics should be administered if
there is concurrent bacterial infection.
Case reports suggest that systemic corticosteroids and Suggested Reading
Barkai G, Sinai L. Index of suspicion: acute hemorrhagic edema of
antihistamines do not alter the course of the disease,
infancy. Pediatr Rev. 2003;24:349 –353
although some authors recommend treating AHEI with Caksen H, Odabas D, Kosem M, et al. Report of eight infants with
corticosteroids if the ears or joints appear compromised. acute infantile hemorrhagic edema and review of the literature.
J Dermatol. 2002;29:290 –295
Patient Course da Silva Manzoni AP, Viecili JB, de Andrade CB, et al. Acute
The patient was treated with prednisolone (1 mg/kg per hemorrhagic edema of infancy: a case report. Int J Dermatol.
2004;43:48 –51
day) because of rapid disease progression. Within 48 hours,
Garty BZ, Ofer I, Finkelstein Y. Acute hemorrhagic edema of
his condition had improved, and by 7 days, the skin lesions infancy. IMAJ. 2002;4:228 –229
had resolved completely. Prednisolone was tapered gradu- Smitt JH, Vermeer MH, Faber WR. Acute hemorrhagic edema of
ally over the next 2 weeks. The disease has not recurred. infancy (AHEI). Clin Dermatol. 2002;20:2–3
e74 Pediatrics in Review Vol.27 No.11 November 2006
commentary
Commentary
The Value of the ECG in the Preparticipation Sports Physical
Examination: The Italian Experience
Editor’s note: This commentary by Dr young athletes by preparticipation cases of sudden death in young people
Vitiello addresses cardiovascular prepar- screenings because there is a high in- and observed a significant reduction of
ticipation sports screening by describ- cidence of catastrophic deaths caused HCM-caused sudden death from the
ing the extensive Italian protocol aimed by cardiomyopathy in young athletes. expected 24% to 2% (one case). Further-
at preventing cardiovascular deaths in (2)(3)(4)(5) more, recognition of the relatively more
athletes. Presented data indicate the The Italian preparticipation screen- rare disease, arrhythmogenic right ven-
value of the protocol, and extending ing program, by requiring ECG studies, tricular (RV) cardiomyopathy, as a cause
the practice across Europe has been might reduce mortality. The thinking is of death increased. Thus, it appears that
proposed. Readers not only will find this that the ECG is an excellent screening the ECG has been an extremely valuable
information to be educational but also test for hypertrophic cardiomyopathy addition to the Italian program.
will appreciate the value of viewpoints (HCM), (6) the leading cause of sports- Besides HCM, other causes of car-
and experiences from other countries. related cardiac death. (7)(8)(9)(10) diac arrest in athletes may manifest
We hope to present more of these Burke and associates (8) found that ECG abnormalities at the preparticipa-
contributions from outside of North 24% of sudden deaths during compet- tion cardiovascular screening. These
America in the near future.—LFN itive sporting events were caused by disorders include arrhythmogenic RV
HCM. After the institution of the Italian cardiomyopathy, long QT syndrome, di-
In 1982, the Italian Ministry of Health
law, Corrado and colleagues (11) pro- lated cardiomyopathy, and Brugada
mandated required screening for every-
spectively studied 269 consecutive syndrome. With this knowledge in
one who participates in competitive
sports. (1) The law states that every 1 to
2 years, all competitive athletes must
be certified for participation. The defi- Classifications of Sport According to Type
Table.
nition of a competitive athlete includes of Screening
students in secondary schools, members
of sports clubs, and professional ath- Screening: Clinical Visit,
letes. By law, the screenings are per- Screening: Clinical Visit, 12-lead ECG, Exercise Testing,
formed at designated “Centers for Sport 12-lead ECG, Urinalysis Spirometry, Urinalysis
Medicine” and are conducted by sports Sport Frequency (y) Sport Frequency (y)
medicine specialists. The evaluation in- Auto racing 1 Soccer 1
cludes a comprehensive family and per- Badminton 2 Baseball 1
sonal history, a physical examination, a Bobsled 1 Boxing 1
12-lead electrocardiogram (ECG), and a Golf 2 Canoeing/Kayaking 1
Motorcycling 1 Rowing 1
urinalysis. Furthermore, athletes partic-
Diving 1 Speed skating 1
ipating in certain high-intensity sports Riflery 1 Hockey 1
also must undergo exercise testing and Archery 2 Skiing 1
pulmonary function testing (Table). Table tennis 2 Rugby 1
Those in whom abnormalities are found Karting 2 Tennis 1
Cycling 1
on the initial screening studies are
Swimming 1
referred for additional tests, including Basketball 1
echocardiography, 24-hour Holter moni- Biathlon/Pentathlon 1
toring, and others as necessary. (1) Gymnastics 1
In Italy, there has been considerable Modified from Decree of Italian Ministry of Health (1).
interest in preventing sudden death in
Pediatrics in Review Vol.27 No.11 November 2006 e75
commentary
mind, it is critical to characterize the Renato Vitiello, MD ding SS, Kurosaki TT, Bild DE. Prevalence
ECG findings in these diseases fully and Unità Operativa Complessa di of hypertrophic cardiomyopathy in a gen-
eral population of young adults: echocar-
to disseminate this information con- Pediatria e Neonatologia
diographic analysis of 4,111 subjects in the
cisely to those administering the pre- Ospedal Civile Torre Annunziata
CARDIA study: Coronary Artery Risk De-
participation screenings. Torre Annunziata, Italy velopment In (young) Adults. Circulation.
We believe that the Italian screen- 1995;92:785–789
ing system, which by national law re- 8. Burke AP, Farb A, Virmani R, Goodin J,
References Smialek JE. Sports-related and non-sports-
quires examinations and also routinely
1. Decree of the Italian Ministry of Health, related sudden cardiac death in young
employs the ECG, results in a significant February 18, 1982. Norme per la tutela sani- adults. Am Heart J. 1991;121:568 –575
reduction in sport-related cardiac taria dell’attività sportiva agonistica (rules con- 9. Maron BJ. Sudden death in young ath-
deaths. Accordingly, there has been cerning the medical protection of athletic ac-
letes. N Engl J Med. 2003;349:1064 –1075
great interest in the Italian model from tivity). Gazzetta Ufficiale. March 5, 1982;63
10. Maron BJ, Shirani J, Poliac LC, Ma-
2. Corrado D, Fontaine G, Marcus F, et al.
the greater European medical commu- thenge R, Roberts WC, Mueller FO. Sud-
Arrhythmogenic right ventricular dysplasia/
nity. Recently, the Study Group of Sport den death in young competitive athletes:
cardiomyopathy: need for an international
clinical, demographic, and pathological pro-
Cardiology of the Working Group of registry. Circulation. 2000;101:e101– e106.
Available at: http://circ.ahajournals.org/ files. JAMA. 96;276:199 –204
Cardiac Rehabilitation and Exercise 11. Corrado D, Basso C, Schiavon M,
cgi/content/full/101/11/e101
Physiology and the Working Group of Thiene G. Screening for hypertrophic car-
3. Thiene G, Nava A, Corrado D, Rossi L,
Myocardial and Pericardial Diseases of Penneli N. Right ventricular cardiomyopa- diomyopathy in young athletes. N Engl
the European Society of Cardiology thy and sudden death in young people. J Med. 1998;339:364 –369
N Eng J Med. 1988;318:129 –133 12. Corrado D, Pelliccia A, Bjornstad HH,
presented a consensus document, in
4. Thiene G, Basso C, Corrado D. Is pre- et al. Cardiovascular pre-participation screen-
which the key role of the 12-lead ECG ing of young competitive athletes for pre-
vention of sudden death in young athletes
for identification of cardiac diseases feasible? Cardiologia. 1999;44:497–505 vention of sudden death: proposal for a
leading to sudden death was empha- 5. Corrado D, Basso C, Thiene G. Arrhyth- common European protocol. Consensus
sized. (12) This same study group is mogenic right ventricular cardiomyopathy: Statement of the Study Group of Sport Car-
working on updated European guide- diagnosis, prognosis, and treatment. Heart. diology of the Working Group of Cardiac
2000;83:588 –595 Rehabilitation and Exercise Physiology and
lines to be published soon, although
6. Maron BJ. Hypertrophic cardiomyopa- the Working Group of Myocardial and Peri-
there may be problems for the differ- thy: a systematic review. JAMA. 2002;287: cardial Diseases of the European Society
ent health organizations in the Euro- 1308 –1320 of Cardiology. Eur Heart J. 2005;26:
pean countries. 7. Maron BJ, Gardin JM, Flack JM, Gid- 516 –524
e76 Pediatrics in Review Vol.27 No.11 November 2006
View publication stats
You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Breast Milk: Benefits & BarriersDocument22 pagesBreast Milk: Benefits & BarriersNazia ArifNo ratings yet
- AVENT Breastfeeding Online Guidebook2018Document60 pagesAVENT Breastfeeding Online Guidebook2018indikapereraNo ratings yet
- Reading Part A Practice Test-1Document5 pagesReading Part A Practice Test-1Andrewfield Perino100% (2)
- Mediwood 3.0 by DR Naveen Koval (With Links)Document707 pagesMediwood 3.0 by DR Naveen Koval (With Links)Rahul B100% (1)
- A-MIDTERMS EXAM-NutriLEC - To PrintDocument9 pagesA-MIDTERMS EXAM-NutriLEC - To PrintNelia AlfonsoNo ratings yet
- 2AN Group 3 Script/Flow For RLE CHN Duty RotationDocument8 pages2AN Group 3 Script/Flow For RLE CHN Duty RotationLouwella RamosNo ratings yet
- CHNDocument9 pagesCHNann aquinoNo ratings yet
- Writing The EditorialDocument12 pagesWriting The EditorialJessa Mae Lopez DonayreNo ratings yet
- Mental Health and Indian Classical Music GeneralDocument7 pagesMental Health and Indian Classical Music GeneralArunkumar Suri Dch HinduNo ratings yet
- 798 3072 1 PBDocument12 pages798 3072 1 PBMariana RitaNo ratings yet
- Nur 195 Long Exam P2 Rle 1 - 1Document21 pagesNur 195 Long Exam P2 Rle 1 - 1Marga WreatheNo ratings yet
- Hubungan Antara Pemberian Asi Eksklusif Dengan Kejadian Ispa Pada Bayi Usia 6-12 Bulan Di Puskesmas Purwokerto BaratDocument9 pagesHubungan Antara Pemberian Asi Eksklusif Dengan Kejadian Ispa Pada Bayi Usia 6-12 Bulan Di Puskesmas Purwokerto BaratFindari RahmanNo ratings yet
- Full Download Ebook PDF Breastfeeding and Human Lactation 5th Edition PDFDocument41 pagesFull Download Ebook PDF Breastfeeding and Human Lactation 5th Edition PDFmatthew.breton622100% (30)
- Dole Department Order No. 143-15: CD Technologies Asia, Inc. © 2016Document12 pagesDole Department Order No. 143-15: CD Technologies Asia, Inc. © 2016John Michael CamposNo ratings yet
- An Investigation of The Safety and Nutritional Adequacy of Infant Formulas Found in NigeriaDocument6 pagesAn Investigation of The Safety and Nutritional Adequacy of Infant Formulas Found in NigeriaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Group 2 Case Study 5 QuestionsDocument6 pagesGroup 2 Case Study 5 QuestionsChadd Vyllmorr VillarinNo ratings yet
- Pengaruh Pijat Woolwich Terhadap ProduksDocument7 pagesPengaruh Pijat Woolwich Terhadap ProduksAyu Nur rahmaNo ratings yet
- Breastfeeding BenefitsDocument13 pagesBreastfeeding BenefitsAngelyn Adan VisitacionNo ratings yet
- Nutrients: Nutritional Feeding Strategies in Pediatric Intestinal FailureDocument14 pagesNutrients: Nutritional Feeding Strategies in Pediatric Intestinal FailureKatherin AmadoNo ratings yet
- VitamindDocument2 pagesVitamindBellarmine MillenaNo ratings yet
- Components of Breast MilkDocument2 pagesComponents of Breast MilkAlya Putri KhairaniNo ratings yet
- BXX - Pediatrics PDocument65 pagesBXX - Pediatrics PDr-Firas Nayf Al-ThawabiaNo ratings yet
- Ijraw 2 4 15.1Document7 pagesIjraw 2 4 15.1Jonah MerabNo ratings yet
- Presented By: DR.A.JAYASUDHA, Principal Mrs.K.Jeyanthi, Assoc - ProfessorDocument74 pagesPresented By: DR.A.JAYASUDHA, Principal Mrs.K.Jeyanthi, Assoc - ProfessorsanthiyasandyNo ratings yet
- MSC Food Service Management and DieteticsDocument36 pagesMSC Food Service Management and Dieteticsmukulazad1988No ratings yet
- PIF Exemplo Japan - Eng2Document2 pagesPIF Exemplo Japan - Eng2DANIELLA GalegoNo ratings yet
- World Breastfeeding Week UntouchedDocument4 pagesWorld Breastfeeding Week UntouchedSowbharnikaNo ratings yet
- Optimal Protein Intake GuideDocument35 pagesOptimal Protein Intake GuideNa OliveiraNo ratings yet
- Pregnancy and LactationDocument40 pagesPregnancy and LactationBabs tvNo ratings yet
- Breast To BibDocument85 pagesBreast To BibsandNo ratings yet