You might also like
- Biologic Therapies: What and When?: ReviewDocument10 pagesBiologic Therapies: What and When?: ReviewRameshKrishnanNo ratings yet
- QP Code: 101501 Reg. No.: D.M. (Cardiology) Degree Regular/Supplementary Examinations September 2020Document1 pageQP Code: 101501 Reg. No.: D.M. (Cardiology) Degree Regular/Supplementary Examinations September 2020RameshKrishnanNo ratings yet
- Arterial Blood Gas Analysis: Ram E. RajagopalanDocument26 pagesArterial Blood Gas Analysis: Ram E. RajagopalanRameshKrishnanNo ratings yet
- Pclinical Aspects of Overlap Syndrome Case Report and Literature Reviewp PDFDocument15 pagesPclinical Aspects of Overlap Syndrome Case Report and Literature Reviewp PDFRameshKrishnanNo ratings yet
- Https Natboard - Edu.in NewWeb Stage-Site Notices Final Notice 31-5-20 A PDFDocument3 pagesHttps Natboard - Edu.in NewWeb Stage-Site Notices Final Notice 31-5-20 A PDFRameshKrishnanNo ratings yet
- Ventilación en SDRA - Guia ClinicaDocument18 pagesVentilación en SDRA - Guia ClinicaPablo PradoNo ratings yet
- Hypoaldosteronism - Johns Hopkins Diabetes GuideDocument4 pagesHypoaldosteronism - Johns Hopkins Diabetes GuideRameshKrishnanNo ratings yet
- Https Natboard - Edu.in NewWeb Stage-Site Notices Final Notice 31-5-20 A PDFDocument3 pagesHttps Natboard - Edu.in NewWeb Stage-Site Notices Final Notice 31-5-20 A PDFRameshKrishnanNo ratings yet
- Kikucchi Disease Poster FinalDocument1 pageKikucchi Disease Poster FinalRameshKrishnanNo ratings yet
- Labile Hypertension: A New Disease or A Variability Phenomenon?Document9 pagesLabile Hypertension: A New Disease or A Variability Phenomenon?RameshKrishnanNo ratings yet
- 50 Apnea Test For Determination of Clinical Brain Death1Document1 page50 Apnea Test For Determination of Clinical Brain Death1Maximiliano Vielma RojasNo ratings yet
- PDFDocument349 pagesPDFRameshKrishnanNo ratings yet
- Hypoglycemic Encephalopathy A Neurologic Manifestation of HypoglycemiaDocument2 pagesHypoglycemic Encephalopathy A Neurologic Manifestation of HypoglycemiaRameshKrishnanNo ratings yet
- 100014Z09JM2016 Mathew PDFDocument7 pages100014Z09JM2016 Mathew PDFRameshKrishnanNo ratings yet
- Severe Acute Respiratory Syndrome (SARS) : Fifty-Sixth World Health Assembly WHA56.29 Agenda Item 14.16 28 May 2003Document4 pagesSevere Acute Respiratory Syndrome (SARS) : Fifty-Sixth World Health Assembly WHA56.29 Agenda Item 14.16 28 May 2003Addy HardianaNo ratings yet
- 45472Document21 pages45472RameshKrishnanNo ratings yet
- 3943 16392 1 PBDocument3 pages3943 16392 1 PBRameshKrishnanNo ratings yet
- Multiple MyelomaDocument23 pagesMultiple MyelomaRameshKrishnanNo ratings yet
- Psoriatic Arthritis EULAR-1Document11 pagesPsoriatic Arthritis EULAR-1RameshKrishnanNo ratings yet
- Assessment of The Left Ventricular Function in Normotensive Prediabetics: A Tissue Doppler Echocardiography StudyDocument7 pagesAssessment of The Left Ventricular Function in Normotensive Prediabetics: A Tissue Doppler Echocardiography StudyRameshKrishnanNo ratings yet
- Pi Is 0085253815344501Document15 pagesPi Is 0085253815344501RameshKrishnanNo ratings yet
- Artritis Reumatoide Fisiopatología PDFDocument15 pagesArtritis Reumatoide Fisiopatología PDFJaime BarraganNo ratings yet
- Poster Ramesh MMDocument5 pagesPoster Ramesh MMRameshKrishnanNo ratings yet
- CKDDocument46 pagesCKDRameshKrishnanNo ratings yet
- Pathophysiology of UTIDocument1 pagePathophysiology of UTIRameshKrishnanNo ratings yet
- Multiple Myeloma Presenting As Oral Cavity Lesion: Stand Life SciencesDocument2 pagesMultiple Myeloma Presenting As Oral Cavity Lesion: Stand Life SciencesRameshKrishnanNo ratings yet
- New Official Website of Aryabhatta Knowledge University - PDFDocument1 pageNew Official Website of Aryabhatta Knowledge University - PDFRameshKrishnanNo ratings yet
- Ketamine-Induced Affective Switch in A Patient With Treatment-Resistant DepressionDocument3 pagesKetamine-Induced Affective Switch in A Patient With Treatment-Resistant DepressionRameshKrishnanNo ratings yet
- Eular Congress News - EULAR 2018 Report - Page 13Document1 pageEular Congress News - EULAR 2018 Report - Page 13RameshKrishnanNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- TOG 2023 Volume 25 Issue 3Document86 pagesTOG 2023 Volume 25 Issue 3saeed hasan saeedNo ratings yet
- Wound Management With Excessive DrainageDocument6 pagesWound Management With Excessive DrainageMatthew RyanNo ratings yet
- 3.5 A Clinical Classification of Cephalo-Pelvic Disproportion. C.J.T. CraigDocument2 pages3.5 A Clinical Classification of Cephalo-Pelvic Disproportion. C.J.T. CraigM ArdarisNo ratings yet
- History of Medical TechnologyDocument20 pagesHistory of Medical TechnologyAndrea-Ann CaravanaNo ratings yet
- Diagnostic - Procedure DoyleDocument1 pageDiagnostic - Procedure Doylemp1757No ratings yet
- A Family Physician's Perspective On Vaccine Hesitancy: Margot Savoy, MD, MPH, FaafpDocument6 pagesA Family Physician's Perspective On Vaccine Hesitancy: Margot Savoy, MD, MPH, FaafpNational Press FoundationNo ratings yet
- The Hospital Formulary: Bilal Hassan M.Phil PharmaceuticsDocument11 pagesThe Hospital Formulary: Bilal Hassan M.Phil PharmaceuticsShafaqat Ghani Shafaqat GhaniNo ratings yet
- Syllabus ClinPhar143Document2 pagesSyllabus ClinPhar143Angel GoNo ratings yet
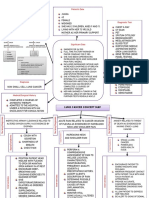
- Lung Cancer Concept Map-Group 2Document2 pagesLung Cancer Concept Map-Group 2Maria Cristina100% (2)
- National Oral Health Program GuidelinesDocument21 pagesNational Oral Health Program GuidelinesAniket PotnisNo ratings yet
- Star Out Patient Care Insurance PolicyV 1.0may2023Document37 pagesStar Out Patient Care Insurance PolicyV 1.0may2023ठाकुर सूरज राणाNo ratings yet
- Medicaliq Blogspot Com 2014-11-130 Top Epidemiology MultipleDocument25 pagesMedicaliq Blogspot Com 2014-11-130 Top Epidemiology MultipleRozen Tareque HasanNo ratings yet
- List of Master TemplatesDocument3 pagesList of Master TemplatesFlemingdonchcNo ratings yet
- Health Insurance Proposal Form SummaryDocument4 pagesHealth Insurance Proposal Form SummarySTARSRINo ratings yet
- PDGMDocument39 pagesPDGMLaluMohan KcNo ratings yet
- Journal Maria F Delong - Impact of Plaque Burden Vs Stenosis On Ischemic Events in Patient With Coronary AtherosclerosisDocument20 pagesJournal Maria F Delong - Impact of Plaque Burden Vs Stenosis On Ischemic Events in Patient With Coronary AtherosclerosisAris MarutoNo ratings yet
- Factors Affecting The Outcomes of Direct Pulp Capping Using BiodentineDocument9 pagesFactors Affecting The Outcomes of Direct Pulp Capping Using BiodentineyesikaichaaNo ratings yet
- Contingency PLAN COVID 19 FIN Sept 29 2022Document35 pagesContingency PLAN COVID 19 FIN Sept 29 2022Fabro F. MhiseyNo ratings yet
- Sexual Behavior - Challenges For Prevention and Control Among Medical Students in MexicoDocument9 pagesSexual Behavior - Challenges For Prevention and Control Among Medical Students in MexicoMiguel BoonaparteNo ratings yet
- Umbilical HerniapdfDocument16 pagesUmbilical HerniapdfAimie Farhanah Binti ZakariaNo ratings yet
- 001 RCA FlipchartDocument40 pages001 RCA FlipchartAbd ZouhierNo ratings yet
- Bureau of Fire Protection First AidDocument7 pagesBureau of Fire Protection First AidRexelle RamosNo ratings yet
- Guide to the history and physical exam for urologic patientsDocument39 pagesGuide to the history and physical exam for urologic patientsNendy OktariNo ratings yet
- Diabetes Mellitus NCPDocument6 pagesDiabetes Mellitus NCPJOHN CARLO APATANNo ratings yet
- Daleel EDocument44 pagesDaleel Ealiplus007No ratings yet
- Paediatric Question BankDocument27 pagesPaediatric Question BankBashiru SelemaniNo ratings yet
- Case Study ScriptDocument5 pagesCase Study ScriptTRECHIA DELA CRUZNo ratings yet
- Viva Content of PsychiatricDocument152 pagesViva Content of PsychiatricMonika Joseph0% (1)
- 2022-01 PresentationDocument31 pages2022-01 PresentationAnthony Babbitt, PhD, MSNo ratings yet
- Guideline of Record-KeepingDocument9 pagesGuideline of Record-KeepingGen LCNo ratings yet