You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- ADV BodySculptor THDDocument8 pagesADV BodySculptor THDali salahNo ratings yet
- Analgesics in Oral and Maxillofacial SurgeryDocument118 pagesAnalgesics in Oral and Maxillofacial SurgeryPavan Tenglikar100% (1)
- Powerpoint: Disorders of The EsophagusDocument65 pagesPowerpoint: Disorders of The Esophagusj.doe.hex_8782% (11)
- Caripirazine Review in SchizophreniaDocument13 pagesCaripirazine Review in SchizophreniaEsraa SaeedNo ratings yet
- Glaucoma & CataractDocument53 pagesGlaucoma & CataractBenita100% (1)
- New Consolidated List of EmpanelmentDocument16 pagesNew Consolidated List of EmpanelmentRajesh PatelNo ratings yet
- Acs (Acute Coronary Syndrome)Document54 pagesAcs (Acute Coronary Syndrome)xiaou123100% (1)
- Effectiveness of Myofunctional Therapy in Ankyloglossia: A Systematic ReviewDocument18 pagesEffectiveness of Myofunctional Therapy in Ankyloglossia: A Systematic Reviewmistic0No ratings yet
- AA Effectiveness - Faith Meets ScienceDocument68 pagesAA Effectiveness - Faith Meets SciencejgogekNo ratings yet
- Department of Rehabilitation Medicine: Philippine Orthopedic CenterDocument1 pageDepartment of Rehabilitation Medicine: Philippine Orthopedic Centerma celine villoNo ratings yet
- The Value of Meaningful Activity - Hospital Arts Programme January To March 2019Document48 pagesThe Value of Meaningful Activity - Hospital Arts Programme January To March 2019ArtlinkEdinburghNo ratings yet
- 2013-5-20 CE Mark Approval For BioMatrix NeoFlexDocument2 pages2013-5-20 CE Mark Approval For BioMatrix NeoFlexphuawlNo ratings yet
- Snake Bite ICU ManagementDocument52 pagesSnake Bite ICU Managementperfectdoc100% (3)
- Fiberoptic and Flexible Endoscopic-Aided TechniquesDocument51 pagesFiberoptic and Flexible Endoscopic-Aided TechniquesAgustin CuryNo ratings yet
- StudentreportviewerDocument15 pagesStudentreportviewerapi-341527743No ratings yet
- Sexually Transmitted Diseases Treatment Guidelines, 2010 PDFDocument110 pagesSexually Transmitted Diseases Treatment Guidelines, 2010 PDFAzam GundalNo ratings yet
- Question 1hDocument3 pagesQuestion 1hItharshan IndreswaranNo ratings yet
- PaqDocument9 pagesPaqAashique AliNo ratings yet
- Nursing Care in Plastic SurgeryDocument36 pagesNursing Care in Plastic Surgeryjengyee7186No ratings yet
- Jurnal InvaginasiDocument3 pagesJurnal InvaginasiAbdurrohman IzzuddinNo ratings yet
- Eating and Sexual DisorderDocument30 pagesEating and Sexual DisorderbiatchiiNo ratings yet
- The Mental Health Continuum Model: Healthy Reacting Injured ILLDocument1 pageThe Mental Health Continuum Model: Healthy Reacting Injured ILLViet Quang NguyenNo ratings yet
- Sand Brochure July 2016Document2 pagesSand Brochure July 2016Jack CianfaglioneNo ratings yet
- Puerperal Psychosis: A Carer's Survival GuideDocument64 pagesPuerperal Psychosis: A Carer's Survival GuideGrace LNo ratings yet
- 1 Compression Therapy..Document43 pages1 Compression Therapy..Nermeen7No ratings yet
- Project in Mapeh (Health)Document8 pagesProject in Mapeh (Health)guache warrinNo ratings yet
- DiarroheaDocument44 pagesDiarroheaRashmi SharmaNo ratings yet
- Appendix To Chapter Four: Applying Supply and Demand Analysis To Health CareDocument6 pagesAppendix To Chapter Four: Applying Supply and Demand Analysis To Health CaredeepikaNo ratings yet
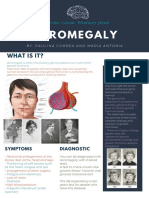
- Acromegaly: What Is It?Document1 pageAcromegaly: What Is It?Paulina CorreaaNo ratings yet
- Client Intake Form - NailsDocument2 pagesClient Intake Form - NailsGGenZ ConsultingNo ratings yet