You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Spe Math p2 Revision Yr7Document24 pagesSpe Math p2 Revision Yr7Hadizah JulaihiNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- R134a HXWC Series Water Cooled Screw Flooded Chillers Cooling Capacity 200 To 740 Tons 703 To 2603 KW Products That Perform PDFDocument16 pagesR134a HXWC Series Water Cooled Screw Flooded Chillers Cooling Capacity 200 To 740 Tons 703 To 2603 KW Products That Perform PDFmohamad chaudhariNo ratings yet
- 10 - Starting and ReversingDocument4 pages10 - Starting and ReversingAisha Zaheer100% (3)
- Geomechanics & ERDDocument18 pagesGeomechanics & ERDRene Torres HinojosaNo ratings yet
- 235practice Exam 2 AnswerDocument9 pages235practice Exam 2 Answernbobs7No ratings yet
- 2200SRM1266 (06 2006) Uk enDocument28 pages2200SRM1266 (06 2006) Uk enEbied Yousif Aly100% (9)
- Penilaian Babak Penyisihan Poster Publik EXIT 2021Document6 pagesPenilaian Babak Penyisihan Poster Publik EXIT 2021mutialailaniNo ratings yet
- Transport of Oxygen and Carbon Dioxide in Blood and Tissue FluidsDocument22 pagesTransport of Oxygen and Carbon Dioxide in Blood and Tissue FluidsmutialailaniNo ratings yet
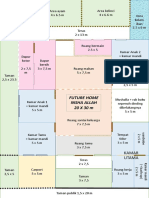
- Future Home Insha Allah (20 X 30 M)Document1 pageFuture Home Insha Allah (20 X 30 M)mutialailaniNo ratings yet
- Table 1Document4 pagesTable 1mutialailaniNo ratings yet
- AHF - ProQuestDocuments-2021-03-21Document18 pagesAHF - ProQuestDocuments-2021-03-21mutialailaniNo ratings yet
- CSV Acuteheart SetDocument1 pageCSV Acuteheart SetmutialailaniNo ratings yet
- Time Since Death From Rigor Mortis: Forensic Prospective: Review ArticleDocument10 pagesTime Since Death From Rigor Mortis: Forensic Prospective: Review Articleangga nugrahaNo ratings yet
- No Author Region Specimens Type Number of Sample Study Design BiomarkerDocument2 pagesNo Author Region Specimens Type Number of Sample Study Design BiomarkermutialailaniNo ratings yet
- Ucl Graduate Prospectus 2019 20 PDFDocument64 pagesUcl Graduate Prospectus 2019 20 PDFmutialailaniNo ratings yet
- 01 - Electro Chemistry (Level) Module-6-1Document16 pages01 - Electro Chemistry (Level) Module-6-1Raju SinghNo ratings yet
- File: OPL3.java Software Implementation of The Yamaha YMF262 Sound Generator. Version 1.0.6Document18 pagesFile: OPL3.java Software Implementation of The Yamaha YMF262 Sound Generator. Version 1.0.6mendofriulNo ratings yet
- Pitcher TemplateDocument1 pagePitcher Templatem.usmanNo ratings yet
- Reducing Signal NoiseDocument4 pagesReducing Signal NoiseXan OVNo ratings yet
- Industrial Organization (Theory and Practice) - 184-189Document6 pagesIndustrial Organization (Theory and Practice) - 184-189kurniaNo ratings yet
- 5000 KW Gearbox High Pinion Bearing Temperatures 1644227029Document7 pages5000 KW Gearbox High Pinion Bearing Temperatures 1644227029MC ANo ratings yet
- 3) Production SchedulingDocument26 pages3) Production SchedulingJhon Ace DuricoNo ratings yet
- Training - Manual - Diagnostic - and - Troublesh CPC 202GDocument186 pagesTraining - Manual - Diagnostic - and - Troublesh CPC 202GGA AnnerNo ratings yet
- CBCS Revised BCA 5 and 6 Sem-FinalDocument38 pagesCBCS Revised BCA 5 and 6 Sem-FinalIrfan AhmedNo ratings yet
- AI Lab Assignment: Q4. Implementation of 8 Queens ProblemDocument8 pagesAI Lab Assignment: Q4. Implementation of 8 Queens ProblemSajag ChauhanNo ratings yet
- MATLAB Modeling of SPT and Grain Size Data in Producing Soil-ProfileDocument5 pagesMATLAB Modeling of SPT and Grain Size Data in Producing Soil-Profileicv.xaviNo ratings yet
- Determinants of Profitability Performance: An Analysis of Class I Railroads in The United StatesDocument18 pagesDeterminants of Profitability Performance: An Analysis of Class I Railroads in The United StatesJayaniNo ratings yet
- InfiniBand WikipediaDocument2 pagesInfiniBand WikipediaYoussef BoukhdimiNo ratings yet
- V-Belt Sizing and Selection Guide: Standard V Belt Sizes FHP (Fractional Horsepower) V-Belts 3L, 4L, 5LDocument1 pageV-Belt Sizing and Selection Guide: Standard V Belt Sizes FHP (Fractional Horsepower) V-Belts 3L, 4L, 5LVijay ParmarNo ratings yet
- Mechanics of Solids by Crandall, Dahl, Lardner, 2nd ChapterDocument118 pagesMechanics of Solids by Crandall, Dahl, Lardner, 2nd Chapterpurijatin100% (2)
- Jimma Institute of Technology Faculty of Mechanical EngineeringDocument38 pagesJimma Institute of Technology Faculty of Mechanical EngineeringIsmail Ibn BehailuNo ratings yet
- Topcon GLS 2200Document2 pagesTopcon GLS 2200asepali005No ratings yet
- Сравнит. лингвистикаDocument22 pagesСравнит. лингвистикаАнастасия ДобровольскаяNo ratings yet
- Muhammad Ajmal Farooqi: Chemical EngineerDocument4 pagesMuhammad Ajmal Farooqi: Chemical EngineeromercomsatNo ratings yet
- Mini Project 2B 6th SemesterDocument28 pagesMini Project 2B 6th SemesterRohit Singh RajputNo ratings yet
- Lab 3Document8 pagesLab 3TOP 5 GHOSTNo ratings yet
- DDDD (Repaired)Document61 pagesDDDD (Repaired)Phung ba Quoc AnhNo ratings yet
- Cennamo - Intransitivity, Object Marking and Event StructureDocument16 pagesCennamo - Intransitivity, Object Marking and Event StructureAugusto PérezNo ratings yet