You might also like
- DFSGDFGDFDocument60 pagesDFSGDFGDFMada Dwi HariNo ratings yet
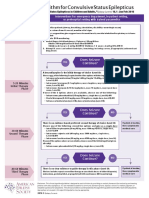
- CSE Treatment Chart-Final - RereleaseDocument1 pageCSE Treatment Chart-Final - RereleaseRizki Maulana TsaniNo ratings yet
- K33.2014 Trauma UG (Dr. TB)Document24 pagesK33.2014 Trauma UG (Dr. TB)Rizki Maulana TsaniNo ratings yet
- K27. Cardiovascular ToxicologyDocument16 pagesK27. Cardiovascular ToxicologyRizki Maulana TsaniNo ratings yet
- K19. Heart FailureDocument46 pagesK19. Heart FailureRizki Maulana TsaniNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Lou Ruvo Center For Brain HealthDocument8 pagesLou Ruvo Center For Brain HealthVladěn KubíčkováNo ratings yet
- 1 UsmleDocument6 pages1 UsmleKeaira KcNo ratings yet
- Palliative Care: Palliative Care (Derived From The Latin Root Palliare, or "To Cloak") Is An Interdisciplinary MedicalDocument2 pagesPalliative Care: Palliative Care (Derived From The Latin Root Palliare, or "To Cloak") Is An Interdisciplinary MedicalLNo ratings yet
- CHAPTER 7: Phar Macology, Medical Diagnostic Techno Logy, Treatment An D Life SupportDocument118 pagesCHAPTER 7: Phar Macology, Medical Diagnostic Techno Logy, Treatment An D Life SupportChristine LehmannNo ratings yet
- Histological Features of Candidiasis: By:Mamdouh Dagsh Alshrifi ID:321103259Document14 pagesHistological Features of Candidiasis: By:Mamdouh Dagsh Alshrifi ID:321103259Mamdouh D AlrwailiNo ratings yet
- Diagnostic Criteria For 298Document1 pageDiagnostic Criteria For 298Pradeep KumarNo ratings yet
- Case StudyDocument9 pagesCase StudyHenriettaNo ratings yet
- Symptoms & Causes of Diabetes NIDDKDocument1 pageSymptoms & Causes of Diabetes NIDDKAl-basri Bakil SampangNo ratings yet
- Malignant Disease of The JawsDocument26 pagesMalignant Disease of The JawsRawda NajjarNo ratings yet
- Kinesitherapie Et Covid 19 Tristan BonnevieDocument82 pagesKinesitherapie Et Covid 19 Tristan BonnevieSteveNo ratings yet
- Ophtha SGD 1Document4 pagesOphtha SGD 1Richelle IgnacioNo ratings yet
- Assignment1-UnaniMedicine Dosage LabellingDocument12 pagesAssignment1-UnaniMedicine Dosage LabellingFarhat JahanNo ratings yet
- Virtualreal Psychotherapeutic ToolDocument29 pagesVirtualreal Psychotherapeutic Toollic.evelincincottaNo ratings yet
- Effectiveness of TMS in Treatment Resistant Depression - EditedDocument13 pagesEffectiveness of TMS in Treatment Resistant Depression - EditedBandah Mwiti JosephNo ratings yet
- ChecklistDocument14 pagesChecklistYooleen SanchezNo ratings yet
- Precision 32 CT Product Recommendation, Campo ImagingDocument15 pagesPrecision 32 CT Product Recommendation, Campo ImagingNur HusenNo ratings yet
- Abnormal Psychology 6th Edition Nolen-Hoeksema Solutions Manual 1Document26 pagesAbnormal Psychology 6th Edition Nolen-Hoeksema Solutions Manual 1jamie100% (31)
- Merck Manual: Professional VersionDocument25 pagesMerck Manual: Professional VersionDwina Wiranti PutriNo ratings yet
- Referensi No 7Document5 pagesReferensi No 7Bagus Wanda HabibullahNo ratings yet
- Presentation Cervical SpineDocument48 pagesPresentation Cervical Spinekholoodrezeq8752No ratings yet
- Aha Guidelinedriven Management of Hypertension An Evidencebased UpdateDocument56 pagesAha Guidelinedriven Management of Hypertension An Evidencebased UpdateNanda Gopal Reddy AnamNo ratings yet
- Sleep 50 QuestionnaireDocument5 pagesSleep 50 QuestionnaireSónia Alves100% (1)
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument21 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For Scientistsnevin shawky Prof. Oral SurgeryNo ratings yet
- Samc Prospectus.Document6 pagesSamc Prospectus.Saurabh SinghNo ratings yet
- Intro To Rad MidtermDocument27 pagesIntro To Rad Midtermedenribalde3No ratings yet
- ENGLISH Tìm từ sai-TOEFL- Bài số 1Document5 pagesENGLISH Tìm từ sai-TOEFL- Bài số 1iey ranaNo ratings yet
- DMDocument24 pagesDMJudeLaxNo ratings yet
- NP 5Document12 pagesNP 5June DumdumayaNo ratings yet
- Qn-Rds-Corelab-2022-067: Quality NotificationDocument9 pagesQn-Rds-Corelab-2022-067: Quality NotificationAsesor científico 3 ComprolabNo ratings yet