You might also like
- Enabling Learning in Nursing and Midwifery Practice: A Guide for MentorsFrom EverandEnabling Learning in Nursing and Midwifery Practice: A Guide for MentorsSue WestNo ratings yet
- QI in Nursing 2012Document10 pagesQI in Nursing 2012rnrmmanphdNo ratings yet
- Hospitalist Program Toolkit: A Comprehensive Guide to Implementation of Successful Hospitalist ProgramsFrom EverandHospitalist Program Toolkit: A Comprehensive Guide to Implementation of Successful Hospitalist ProgramsNo ratings yet
- Nursing Student AttitudeDocument6 pagesNursing Student AttitudeI nengahvdarthayasaNo ratings yet
- Qi Nursing Communication Final - Nurs 484Document12 pagesQi Nursing Communication Final - Nurs 484api-558100249No ratings yet
- Brochure NursingDocument10 pagesBrochure Nursingsiska dwiNo ratings yet
- Nursing Information SystemDocument5 pagesNursing Information SystemFransiscaapNo ratings yet
- Developing A Framework: Nursing ResearchDocument10 pagesDeveloping A Framework: Nursing Researchbombillode13No ratings yet
- SN JDDocument2 pagesSN JDChoi ToNo ratings yet
- Nursing LeadershipDocument15 pagesNursing LeadershipRolando PinchettiNo ratings yet
- Negotiating Nursing LeadershipDocument8 pagesNegotiating Nursing LeadershipHani TuasikalNo ratings yet
- Nursing Sensitive Indicators Their RoleDocument3 pagesNursing Sensitive Indicators Their RolePuspita Eka Kurnia SariNo ratings yet
- Clinical Area Objective Headnursing Activities Students Activities EvaluationDocument2 pagesClinical Area Objective Headnursing Activities Students Activities EvaluationTrixie Anne GamotinNo ratings yet
- What Is Administration in Nursing Service?Document4 pagesWhat Is Administration in Nursing Service?Princess Melanie MelendezNo ratings yet
- A Learning Model For NursingDocument7 pagesA Learning Model For NursingLina Mahayaty SembiringNo ratings yet
- T5 Plan The Nursing InterventionDocument22 pagesT5 Plan The Nursing InterventionFildzah CyNo ratings yet
- Nurse Residency Program 1Document5 pagesNurse Residency Program 1api-315956703No ratings yet
- The Nursing Assessment and Clinical Nursing JudgementDocument6 pagesThe Nursing Assessment and Clinical Nursing Judgementapi-603940523No ratings yet
- IHI Patient Family Experience of Hospital Care White Paper 2011Document34 pagesIHI Patient Family Experience of Hospital Care White Paper 2011Sorina VoicuNo ratings yet
- Journal Nursing DocumentationDocument8 pagesJournal Nursing DocumentationikaNo ratings yet
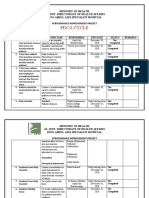
- Pdca CycleDocument4 pagesPdca CycleHamid BouleghabNo ratings yet
- Adaptability of Nursing HandoversDocument22 pagesAdaptability of Nursing HandoversegregiousNo ratings yet
- Nursing PhilosophyDocument6 pagesNursing Philosophyapi-429775578No ratings yet
- Critical Thinking in Nursing Education: A Literature Review: CorrespondenceDocument25 pagesCritical Thinking in Nursing Education: A Literature Review: CorrespondenceLheo AngelesNo ratings yet
- NursingDocument9 pagesNursingMichael_A8No ratings yet
- NUR3165 MS Nursing Research For Evidence-Based Practice 16 Week Fall 2022Document16 pagesNUR3165 MS Nursing Research For Evidence-Based Practice 16 Week Fall 2022Somie Jr. SanchezNo ratings yet
- Interdisciplinary Nursing DocumentationDocument6 pagesInterdisciplinary Nursing Documentationgrace_nakateNo ratings yet
- Scope of NursingDocument4 pagesScope of NursingIvy Jenica Mamuad100% (1)
- Sainath College of Nursing, KatniDocument4 pagesSainath College of Nursing, KatniFabin JoseNo ratings yet
- Evidencebased Healthcare and Quality ImprovementDocument8 pagesEvidencebased Healthcare and Quality ImprovementJemimah BureresNo ratings yet
- Nurs 403 Practice Summary PaperDocument17 pagesNurs 403 Practice Summary Paperapi-369824515No ratings yet
- Nursing InformaticsDocument1 pageNursing InformaticsStacey GarciaNo ratings yet
- The Concept of NursingDocument14 pagesThe Concept of NursingHarry PendiemNo ratings yet
- Interventions in Nursing HomesDocument18 pagesInterventions in Nursing Homesvictory818No ratings yet
- Standard of Nursing ServicesDocument30 pagesStandard of Nursing Servicesardian_primaNo ratings yet
- NRCP EBCS Accountability in NursingPracticeDocument4 pagesNRCP EBCS Accountability in NursingPracticeReshma RinuNo ratings yet
- Nursing Research Methodology 5 PDFDocument12 pagesNursing Research Methodology 5 PDFCarlos Samuel QuimbenzeNo ratings yet
- Capstone Clinical Nursing JudgementDocument7 pagesCapstone Clinical Nursing Judgementapi-544889322No ratings yet
- Emergency Nurses Association (ENA)Document5 pagesEmergency Nurses Association (ENA)Ngu W PhooNo ratings yet
- Nursing PhilosophyDocument5 pagesNursing Philosophyapi-522933227No ratings yet
- Futuristic Nursing: By:-Firoz Qureshi Dept. Psychiatric NursingDocument37 pagesFuturistic Nursing: By:-Firoz Qureshi Dept. Psychiatric NursingpadmaNo ratings yet
- Nursing WorkforceDocument6 pagesNursing WorkforceNashon Reiner KNo ratings yet
- The Nursing ProcessDocument6 pagesThe Nursing Processnazole1978No ratings yet
- The Diagnoses of Community NursingDocument8 pagesThe Diagnoses of Community NursingIOSRjournalNo ratings yet
- Nursing Leadership - Delegation PaperDocument5 pagesNursing Leadership - Delegation PaperKaylee BlankenshipNo ratings yet
- Herzing University Nursing InformationDocument4 pagesHerzing University Nursing InformationEmily DavisNo ratings yet
- Interaction Nursing Staff PDFDocument12 pagesInteraction Nursing Staff PDFLina SafitriNo ratings yet
- Lewis: Medical-Surgical Nursing, 10 Edition: Professional Nursing Practice Key Points Professional Nursing PracticeDocument3 pagesLewis: Medical-Surgical Nursing, 10 Edition: Professional Nursing Practice Key Points Professional Nursing PracticePrincess AgarwalNo ratings yet
- Nursing, Bachelor of Science: WWW - CNC.BC - Ca - 113Document5 pagesNursing, Bachelor of Science: WWW - CNC.BC - Ca - 113cnc_program_pagesNo ratings yet
- Nursing Competencies. The Artristy of NursingDocument6 pagesNursing Competencies. The Artristy of NursingneoclintNo ratings yet
- Nursing Skills ChecklistDocument6 pagesNursing Skills Checklistapi-379379776No ratings yet
- Lollipop UCLA NursingStudyDocument5 pagesLollipop UCLA NursingStudySam DyerNo ratings yet
- Arfan Nursing EducationDocument13 pagesArfan Nursing EducationwahyuningsihhusainNo ratings yet
- Model of Nursing ResearchDocument57 pagesModel of Nursing Researchhye shinNo ratings yet
- NursingDocument14 pagesNursingbipinsteeephenNo ratings yet
- A Philosophy of NursingDocument2 pagesA Philosophy of NursingIrna MegawatyNo ratings yet
- Nur Assess BSN Nursing Care PlanDocument12 pagesNur Assess BSN Nursing Care PlanWen SilverNo ratings yet
- Mod2 - Ch3 - Health IndicatorsDocument13 pagesMod2 - Ch3 - Health IndicatorsSara Sunabara100% (1)
- Nursing TheoryDocument15 pagesNursing TheoryTherese CanapiNo ratings yet
- Nursing Theories and Advanced Practice.Document4 pagesNursing Theories and Advanced Practice.Antony OmbogoNo ratings yet
- Kia - Budi Setyawan - 1-5 - Revisi - OkDocument79 pagesKia - Budi Setyawan - 1-5 - Revisi - OkFitra PringgayudaNo ratings yet
- Florence NightingaleDocument15 pagesFlorence Nightingaleazhar_hussain_15206No ratings yet
- Evaluation of The Use of Electronic Medical Record Systems in Brazilian Intensive Care UnitsDocument9 pagesEvaluation of The Use of Electronic Medical Record Systems in Brazilian Intensive Care UnitsFitra PringgayudaNo ratings yet
- Florence Nightingale: The Lady With The LampDocument15 pagesFlorence Nightingale: The Lady With The LampFitra PringgayudaNo ratings yet
- Editable Classroom Officers TemplateDocument6 pagesEditable Classroom Officers TemplateRachelle AbalosNo ratings yet
- Plastic PackagingDocument47 pagesPlastic PackagingRajaSekarsajja100% (1)
- ISLAND SAILING CLUB COWES 2012 ROUND THE ISLAND RACE RESULTSDocument64 pagesISLAND SAILING CLUB COWES 2012 ROUND THE ISLAND RACE RESULTSmatthias_25No ratings yet
- EIE Resume FormatDocument1 pageEIE Resume FormatRakesh MandalNo ratings yet
- BLRBAC Emergency Shutdown Procedure (February 2012)Document18 pagesBLRBAC Emergency Shutdown Procedure (February 2012)SubburajMechNo ratings yet
- Manual Micro DNC 2dDocument31 pagesManual Micro DNC 2dDiego GarciaNo ratings yet
- Nov 2018 Pathfinder SkillsDocument162 pagesNov 2018 Pathfinder SkillsWaidi AdebayoNo ratings yet
- Kami Export - Exercise Lab - Mini-2Document3 pagesKami Export - Exercise Lab - Mini-2Ryan FungNo ratings yet
- OxygenDocument18 pagesOxygenbillllibNo ratings yet
- Entry Test Result MPhil 2014 PDFDocument11 pagesEntry Test Result MPhil 2014 PDFHafizAhmadNo ratings yet
- Tinas Resturant AnalysisDocument19 pagesTinas Resturant Analysisapi-388014325100% (2)
- Gartner Reprint 2022Document33 pagesGartner Reprint 2022Sajan Rajagopal100% (1)
- Ari Globe Valve SupraDocument26 pagesAri Globe Valve SupraAi-samaNo ratings yet
- 18th Century Political Formation. CL 7Document22 pages18th Century Political Formation. CL 7Gamer AditKills100% (1)
- Industry Standard: What Are The Benefits For You?Document4 pagesIndustry Standard: What Are The Benefits For You?Zarnimyomyint MyintNo ratings yet
- COVID-19 Impact on Philippine ExportsDocument5 pagesCOVID-19 Impact on Philippine ExportsHazel BorboNo ratings yet
- Autoencoder Asset Pricing ModelsDocument22 pagesAutoencoder Asset Pricing ModelsEdson KitaniNo ratings yet
- How efficient is a wind turbineDocument8 pagesHow efficient is a wind turbinejNo ratings yet
- Iwan Lab Guide v1.1 FinalDocument63 pagesIwan Lab Guide v1.1 FinalRicardo SicheranNo ratings yet
- Connect Debug LogDocument20 pagesConnect Debug LogrohanZorba100% (1)
- Lab Manual 2 PrintDocument17 pagesLab Manual 2 Printmonikandakumar ramachandranNo ratings yet
- Day 1 What Is Phased Array How Phased Array Works? Beam Forming Beam Focusing Beam Streeing Sectorial Scan and Linear ScanDocument64 pagesDay 1 What Is Phased Array How Phased Array Works? Beam Forming Beam Focusing Beam Streeing Sectorial Scan and Linear ScanvibinkumarsNo ratings yet
- Toshiba X-Ray Tube Product InfoDocument10 pagesToshiba X-Ray Tube Product InfoJairo ManzanedaNo ratings yet
- COURSE Strucure - M.tech (S.E) I & II Sem (Autonomous)Document40 pagesCOURSE Strucure - M.tech (S.E) I & II Sem (Autonomous)Fresherjobs IndiaNo ratings yet
- United States v. Bueno-Hernandez, 10th Cir. (2012)Document3 pagesUnited States v. Bueno-Hernandez, 10th Cir. (2012)Scribd Government DocsNo ratings yet
- Water Quality For Irrigation Free PPT - Google SearchDocument3 pagesWater Quality For Irrigation Free PPT - Google SearchJames NeoNo ratings yet
- CIVL 222 AXIAL MEMBERSDocument27 pagesCIVL 222 AXIAL MEMBERSskhan247100% (1)
- Simple Problem On ABC: RequiredDocument3 pagesSimple Problem On ABC: RequiredShreshtha VermaNo ratings yet
- ADUHAI @herman & Rhoca - Lyrics and Music by Rhoma Irama Arranged by - HERMAN - BOY - SmuleDocument4 pagesADUHAI @herman & Rhoca - Lyrics and Music by Rhoma Irama Arranged by - HERMAN - BOY - SmuleHERMAN BOYNo ratings yet
- RELATED STUDIES AND LITERATURE ON EGGSHELL POWDER USE IN CONCRETEDocument5 pagesRELATED STUDIES AND LITERATURE ON EGGSHELL POWDER USE IN CONCRETEReiBañez100% (2)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (14)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisFrom EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisRating: 5 out of 5 stars5/5 (8)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (327)
- The Tennis Partner: A Doctor's Story of Friendship and LossFrom EverandThe Tennis Partner: A Doctor's Story of Friendship and LossRating: 4.5 out of 5 stars4.5/5 (4)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)
- Daniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisFrom EverandDaniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisRating: 3.5 out of 5 stars3.5/5 (130)
- Troubled: A Memoir of Foster Care, Family, and Social ClassFrom EverandTroubled: A Memoir of Foster Care, Family, and Social ClassRating: 4.5 out of 5 stars4.5/5 (24)
- Nonviolent Communication by Marshall B. Rosenberg - Book Summary: A Language of LifeFrom EverandNonviolent Communication by Marshall B. Rosenberg - Book Summary: A Language of LifeRating: 4.5 out of 5 stars4.5/5 (49)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- The Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeFrom EverandThe Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeNo ratings yet
- Dark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingFrom EverandDark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingRating: 4 out of 5 stars4/5 (1138)