You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5813)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Radiation Treatment Machine Capacity Planning at Cancer CareDocument8 pagesRadiation Treatment Machine Capacity Planning at Cancer CareeviNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Materi 2 - Prof. Dr. Amin Soebandrio, PH.D., SP - MKDocument27 pagesMateri 2 - Prof. Dr. Amin Soebandrio, PH.D., SP - MKChristina100% (1)
- Senior Citizen Red Carpet BrochureDocument2 pagesSenior Citizen Red Carpet Brochureramki020983No ratings yet
- Vodic Za Stomatologe DHADocument9 pagesVodic Za Stomatologe DHAIvanaNo ratings yet
- Oral ScrerenDocument9 pagesOral Screrenfayasyabmin100% (2)
- DR René KABERA :this Situation Was AlarmingDocument2 pagesDR René KABERA :this Situation Was AlarmingKABERA RENENo ratings yet
- Hyperemesis GravidarumDocument32 pagesHyperemesis GravidarumBharat ThapaNo ratings yet
- ANTENATAL CARE Translate GooglingDocument26 pagesANTENATAL CARE Translate GooglingLutfi ari206100% (2)
- Jurnal Hukum Kesehatan 2020Document14 pagesJurnal Hukum Kesehatan 2020mona marhamahNo ratings yet
- DUPIXENT MyWay English Enrollment FormDocument5 pagesDUPIXENT MyWay English Enrollment FormJhoanna Marie MonterolaNo ratings yet
- CovidDocument5 pagesCovidNirav BhandariNo ratings yet
- MAF WP Heart Rate v1.5Document9 pagesMAF WP Heart Rate v1.5Adi DbgadNo ratings yet
- InfluDocument7 pagesInfluAnh NguyenNo ratings yet
- 4000 PG Medical Admission-2016 Application Form and RulesDocument28 pages4000 PG Medical Admission-2016 Application Form and RulesDr. Karan ShahNo ratings yet
- Biocon:: Launching A New Cancer Drug in IndiaDocument10 pagesBiocon:: Launching A New Cancer Drug in IndiaDeepak Jangid0% (1)
- Modul Skill Drug Prescribing - StudentDocument8 pagesModul Skill Drug Prescribing - StudentCak JamelNo ratings yet
- HRT Formulary and Treatment Guidance: (Apc Clindoc 010)Document8 pagesHRT Formulary and Treatment Guidance: (Apc Clindoc 010)psdsportsdocNo ratings yet
- OM008: Health Information Technology Short Answer Submission FormDocument13 pagesOM008: Health Information Technology Short Answer Submission FormSiddharth DungarwalNo ratings yet
- Health Psychology - Week 1 - Class 2Document14 pagesHealth Psychology - Week 1 - Class 2Behroze khalilNo ratings yet
- Deficient Fluid Volume Nursing Diagnosis & Care Plan - RNlessonsDocument11 pagesDeficient Fluid Volume Nursing Diagnosis & Care Plan - RNlessonsA.No ratings yet
- Trigger Finger Faq 1) What Is Trigger Finger?Document1 pageTrigger Finger Faq 1) What Is Trigger Finger?Lasiaf AlaskaNo ratings yet
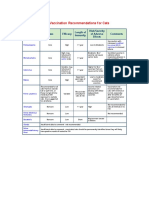
- AVMA Vaccination Recommendations F or CatsDocument2 pagesAVMA Vaccination Recommendations F or CatsHazim Azmi Al-QadryNo ratings yet
- 2 RPSDocument8 pages2 RPSnurfitriaNo ratings yet
- Neurosurgery Direct 6 Yrs PDFDocument31 pagesNeurosurgery Direct 6 Yrs PDFSoumitraNo ratings yet
- Cure Veda-The Modern Science of Healthy Life: September 2021Document8 pagesCure Veda-The Modern Science of Healthy Life: September 2021ReconnectingNo ratings yet
- Introduction To Health Promotion and Health Education - Dr. ElizabethDocument33 pagesIntroduction To Health Promotion and Health Education - Dr. ElizabethArnold Dickens JosephNo ratings yet
- V ' Exgv 'Vex DG©: Health Insurance Claim FormDocument2 pagesV ' Exgv 'Vex DG©: Health Insurance Claim Formjakaria emtiajNo ratings yet
- DSL On Health Care Delivery SystemDocument4 pagesDSL On Health Care Delivery SystemNoreen FæţįmæNo ratings yet
- Pulp Therapy For Primary and Immature Permanent Teeth: Latest RevisionDocument9 pagesPulp Therapy For Primary and Immature Permanent Teeth: Latest RevisionGhufran KhalilNo ratings yet
- Case Report: Systemic Lupus ErythematosusDocument32 pagesCase Report: Systemic Lupus ErythematosusdesmyyNo ratings yet