You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Pub - Parenting A Defiant Child A Sanity Saving Guide To PDFDocument237 pagesPub - Parenting A Defiant Child A Sanity Saving Guide To PDFAlex IordanNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Seven Stages of Crisis Intervention Model PDFDocument27 pagesSeven Stages of Crisis Intervention Model PDFAngeila TolosaNo ratings yet
- Prescriptions And: Medication OrdersDocument67 pagesPrescriptions And: Medication OrdersGraizel Joy Andres100% (1)
- Crane Safety Analysis ReportDocument12 pagesCrane Safety Analysis Report88san100% (1)
- Pasteur Vs Bechamp - An Alternative View of Infectious DiseaseDocument3 pagesPasteur Vs Bechamp - An Alternative View of Infectious DiseaseRadhe GovindaNo ratings yet
- 2nd Edn ID MHFA Manual Sept 2012 SmallDocument125 pages2nd Edn ID MHFA Manual Sept 2012 SmallAnonymous Nvv1TaS7100% (1)
- Anemia NCPDocument5 pagesAnemia NCPMel Christian Baldoz100% (2)
- DepEd Class Schedules and Timetables On The Limited Face-to-Face Learning ModalityDocument21 pagesDepEd Class Schedules and Timetables On The Limited Face-to-Face Learning ModalityCHANIELOU MARTINEZNo ratings yet
- 2003 Gray Literature in Meta Analysis PDFDocument6 pages2003 Gray Literature in Meta Analysis PDFadiNo ratings yet
- Therapeutic CommunicationDocument12 pagesTherapeutic CommunicationadiNo ratings yet
- Responsive DimensionDocument9 pagesResponsive DimensionadiNo ratings yet
- Introduction of Psychiatric NursingDocument26 pagesIntroduction of Psychiatric NursingadiNo ratings yet
- Concepts of Health - IllnessDocument45 pagesConcepts of Health - IllnessadiNo ratings yet
- Diabetes Family Behavior Checklist 2Document2 pagesDiabetes Family Behavior Checklist 2adi100% (1)
- Certificate of Analysis PDFDocument2 pagesCertificate of Analysis PDFadiNo ratings yet
- Complementary Therapies in Clinical Practice: Sai Qi, Shuang Lou, Tao TanDocument4 pagesComplementary Therapies in Clinical Practice: Sai Qi, Shuang Lou, Tao TanMuhammad KamilNo ratings yet
- DapDocument12 pagesDapgopala_krishna_2No ratings yet
- Saint-Go Bain: Safety Data SheetDocument7 pagesSaint-Go Bain: Safety Data SheeteadriesNo ratings yet
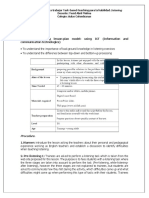
- Task Based Lesson Plan Model 1Document2 pagesTask Based Lesson Plan Model 1yesopunkNo ratings yet
- IRE Tipsheet - Toxic City - Philly InquirerDocument3 pagesIRE Tipsheet - Toxic City - Philly InquirerCoreyJohnsonNo ratings yet
- Disciplines and Ideas in The Applied SocDocument57 pagesDisciplines and Ideas in The Applied SocJenalin MakipigNo ratings yet
- MalpresentationDocument16 pagesMalpresentationAnghel CruzNo ratings yet
- Canadian Diabetes Clinical Guidelines 2008Document215 pagesCanadian Diabetes Clinical Guidelines 2008FelipeOrtiz100% (4)
- Soal Utbk 12Document5 pagesSoal Utbk 12Isro Datul KhasanahNo ratings yet
- Registering As A Nurse or Midwife From Outside EU or EEADocument28 pagesRegistering As A Nurse or Midwife From Outside EU or EEACorinaBotorogaNo ratings yet
- Disorders of The Adrenal Glands: Adrenal Cortical Adenoma and CarcinomaDocument9 pagesDisorders of The Adrenal Glands: Adrenal Cortical Adenoma and Carcinomahussain AltaherNo ratings yet
- HANDOUT ON Care of Eye and Care of Nails and FeetDocument4 pagesHANDOUT ON Care of Eye and Care of Nails and Feetchaitali shankarNo ratings yet
- PHS811 Principles of Health Planning & ManagementDocument171 pagesPHS811 Principles of Health Planning & ManagementRICKSON KAWINANo ratings yet
- Afbc 404 F 2 Baf 1 D 1Document29 pagesAfbc 404 F 2 Baf 1 D 1api-584621926No ratings yet
- Eng 7 WK 1Document12 pagesEng 7 WK 1Jade BaliolaNo ratings yet
- Claim Form - IPDDocument2 pagesClaim Form - IPDEswar Kiran ReddyNo ratings yet
- Theoretical Models DeJoy PDFDocument12 pagesTheoretical Models DeJoy PDFrazamenesesNo ratings yet
- Care Giver Stress IndexDocument2 pagesCare Giver Stress IndexcpradheepNo ratings yet
- File1 146 1714383Document366 pagesFile1 146 1714383Mutiara SazkiaNo ratings yet
- AziziDocument6 pagesAziziAlvi MirzaNo ratings yet
- Polietileno - CAS #9002-88-4 (Formosa Plastics)Document6 pagesPolietileno - CAS #9002-88-4 (Formosa Plastics)Elver GalargaNo ratings yet
- Oral and Maxillofacial Trauma - Fonseca - Primary ManagementDocument7 pagesOral and Maxillofacial Trauma - Fonseca - Primary ManagementyogeshNo ratings yet