You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Test Bank For Williams Essentials of Nutrition and Diet Therapy 12th Edition Eleanor Schlenker Joyce Ann GilbertDocument11 pagesTest Bank For Williams Essentials of Nutrition and Diet Therapy 12th Edition Eleanor Schlenker Joyce Ann Gilbertdennisgallegosmkrgyabsod100% (15)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- ESOR 2017 Annual Report Final PDFDocument108 pagesESOR 2017 Annual Report Final PDFSonia GalliNo ratings yet
- Nut in Clin Prac - 2023 - Mohamed Elfadil - Peptide Based Formula Clinical Applications and BenefitsDocument11 pagesNut in Clin Prac - 2023 - Mohamed Elfadil - Peptide Based Formula Clinical Applications and BenefitshizburNo ratings yet
- Thyroid Testing: What Is A Normal TSH Level?: Implications For PatientsDocument1 pageThyroid Testing: What Is A Normal TSH Level?: Implications For PatientskaterinaNo ratings yet
- Dpue Biology Notes: Chapter - 3 Human ReproductionDocument15 pagesDpue Biology Notes: Chapter - 3 Human ReproductionvdfeNo ratings yet
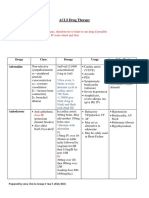
- ACLS Drug Therapy RevisedDocument4 pagesACLS Drug Therapy RevisedpaveethrahNo ratings yet
- Human and Social Biology Pratice QuestionsDocument3 pagesHuman and Social Biology Pratice QuestionsDerron WilliamsNo ratings yet
- Lithium ToxicityDocument28 pagesLithium ToxicityReejan PaudelNo ratings yet
- Adverse Effects of Hormonal ContraceptivesDocument153 pagesAdverse Effects of Hormonal ContraceptivesTWGAScNo ratings yet
- Department of Chemical Pathology: Lipid ProfileDocument2 pagesDepartment of Chemical Pathology: Lipid ProfileShahab KhanNo ratings yet
- Roles of HormonesDocument13 pagesRoles of Hormoneshafizah_90100% (6)
- Smart VisionDocument139 pagesSmart VisionpankajNo ratings yet
- Physical Examination in Psychiatric Practice: Gill GardenDocument8 pagesPhysical Examination in Psychiatric Practice: Gill Gardenyeremias setyawanNo ratings yet
- Beauty From The Inside OutDocument600 pagesBeauty From The Inside Outjaustin4100% (2)
- Differential Diagnosis of Head and SwellingDocument41 pagesDifferential Diagnosis of Head and Swellingmachine318No ratings yet
- CAGANHAO - Masterlist of Pregnant 2021Document161 pagesCAGANHAO - Masterlist of Pregnant 2021Boac Nutrition LadiesNo ratings yet
- B. Sc. 2 YearDocument84 pagesB. Sc. 2 YearSreelekha Ramtenki100% (1)
- Acute Pancreatitis - Godlewska IzabellaDocument2 pagesAcute Pancreatitis - Godlewska IzabellaIzaNo ratings yet
- Benefits of Black Garlic - Black GarlicDocument3 pagesBenefits of Black Garlic - Black GarlicRicardo CampuzanoNo ratings yet
- OET 2.0 AdhdDocument14 pagesOET 2.0 AdhdnishantNo ratings yet
- Fluid Volume Deficit QuestionsDocument6 pagesFluid Volume Deficit QuestionsCorinneNo ratings yet
- Enzyme ReviewDocument7 pagesEnzyme Reviewsmbdy tbhhhNo ratings yet
- OPD Schedule (October 2021)Document33 pagesOPD Schedule (October 2021)Ajay DherwaniNo ratings yet
- Test Bank For Before We Are Born Essentials of Embryology and Birth Defects 8th EditionDocument13 pagesTest Bank For Before We Are Born Essentials of Embryology and Birth Defects 8th EditionTofik MohammedNo ratings yet
- Anti-TPO 30461Document8 pagesAnti-TPO 30461Haider Almothafer0% (1)
- AV Y TẾ 2Document27 pagesAV Y TẾ 2Đạt Bùi TiếnNo ratings yet
- Taurine 3 Cellular and Regulatory MechanismsDocument510 pagesTaurine 3 Cellular and Regulatory MechanismsYoBjjNo ratings yet
- How To Build Your Cellular EngineDocument14 pagesHow To Build Your Cellular EngineEva TuáNo ratings yet
- GPL Test OAT BookDocument40 pagesGPL Test OAT BookJalya JalyaNo ratings yet
- MRCP AcrDocument8 pagesMRCP AcrgurudrarunNo ratings yet