You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Day2 2 Jason Hawrelax Treatment Dysbiosis Small and Large BowelDocument76 pagesDay2 2 Jason Hawrelax Treatment Dysbiosis Small and Large BowelNicoleta ButucNo ratings yet
- Prisma Health Adult Antimicrobial Guidebook 2021Document52 pagesPrisma Health Adult Antimicrobial Guidebook 2021JhNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- A Chronicle: Dax's Case As It HappenedDocument6 pagesA Chronicle: Dax's Case As It Happenedkhanna_chetan45950% (1)
- Experiment ResultsDocument10 pagesExperiment ResultsArdita Rizky Putri ArcanggiNo ratings yet
- B Lactamase 1401 1431 DsDocument3 pagesB Lactamase 1401 1431 DsYenny Paulet Romero GalindoNo ratings yet
- Chapter 5Document2 pagesChapter 5Sid LoverholicNo ratings yet
- CoamoxiclavDocument1 pageCoamoxiclavBbhie AntiguaNo ratings yet
- Isolation, Identification and Characterization of Urinary Tract Infectious Bacteria and The Effect of Different AntibioticsDocument10 pagesIsolation, Identification and Characterization of Urinary Tract Infectious Bacteria and The Effect of Different AntibioticsAlexander DeckerNo ratings yet
- Carbapenamases Facts and DetecctionDocument68 pagesCarbapenamases Facts and Detecctiontummalapalli venkateswara raoNo ratings yet
- Ventilator Associated Pneumonia (Vap)Document11 pagesVentilator Associated Pneumonia (Vap)Suresh KumarNo ratings yet
- Peniciilins and Beta LactamsDocument134 pagesPeniciilins and Beta LactamsMelissa TisadoNo ratings yet
- Medicinal Chemistry 3rd Year Pharm D-2016Document9 pagesMedicinal Chemistry 3rd Year Pharm D-2016Ananda VijayasarathyNo ratings yet
- TICKLER-PRINT Pedia PDFDocument8 pagesTICKLER-PRINT Pedia PDFCarlos H. AcuñaNo ratings yet
- Journal of Research in Pharmacy Practice - 4-222 - DUE of Meropenem at Tertiary Care University HospitalDocument4 pagesJournal of Research in Pharmacy Practice - 4-222 - DUE of Meropenem at Tertiary Care University Hospital8229 ERIKA ARISTA PUTRINo ratings yet
- Thyfoid FeverDocument31 pagesThyfoid FeverTommy Prasetyo AliNo ratings yet
- MeropenemDocument3 pagesMeropenemJasmin T LarizaNo ratings yet
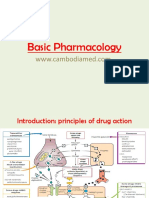
- Basic PharmacologyDocument48 pagesBasic PharmacologyEmily Mccarthy100% (2)
- Sentence ArrangementDocument40 pagesSentence ArrangementAditya Ramana Sastry UNo ratings yet
- Antibiotics 1Document41 pagesAntibiotics 1AlaaNo ratings yet
- BD Phoenix AST User ManualDocument280 pagesBD Phoenix AST User ManualDewi Paramita YuniarahmiNo ratings yet
- Drugs For Bacterial InfectionsDocument7 pagesDrugs For Bacterial InfectionsArienne Janine MalabananNo ratings yet
- OPAT Anti-Infective Administration MethodsDocument6 pagesOPAT Anti-Infective Administration MethodsNikki TranNo ratings yet
- WHY NOT BHARAT RATNA TO GREAT MEDICAL SCIENTIST AND MAN OF MIRACLE DRUGS DR - YELLAPRAGADA SUBBA RAO ?Document13 pagesWHY NOT BHARAT RATNA TO GREAT MEDICAL SCIENTIST AND MAN OF MIRACLE DRUGS DR - YELLAPRAGADA SUBBA RAO ?Anumakonda JagadeeshNo ratings yet
- Antibiotics MCQsDocument4 pagesAntibiotics MCQsPh Israa Kadhim100% (1)
- Fact Sheet Denagard Mycoplasma SPP MIC ValuesDocument4 pagesFact Sheet Denagard Mycoplasma SPP MIC Valuesnick224No ratings yet
- 03 The Evaluation of Antibacterial Activity of Fabrics Impregnated With Dimethyltetradecyl (3 - (Trimethoxysilyl) Propyl) Ammonium ChlorideDocument8 pages03 The Evaluation of Antibacterial Activity of Fabrics Impregnated With Dimethyltetradecyl (3 - (Trimethoxysilyl) Propyl) Ammonium Chloridedharmayanti976No ratings yet
- Antimicrobial Drugs: Powerpoint Presentations Prepared by Bradley W. Christian, Mclennan Community CollegeDocument35 pagesAntimicrobial Drugs: Powerpoint Presentations Prepared by Bradley W. Christian, Mclennan Community CollegeTiffany Jane Huertas100% (1)
- Antibiotic Resistance: Audience-Senior Medical Officers Venue-Pune Date - 9 May 2011Document42 pagesAntibiotic Resistance: Audience-Senior Medical Officers Venue-Pune Date - 9 May 2011J Nuchin100% (1)
- Secundum Artem: Compounding For Otic DisordersDocument0 pagesSecundum Artem: Compounding For Otic Disordersdebieyolanda_7180456No ratings yet
- Megha Kulkarni: Dept of PharmacologyDocument51 pagesMegha Kulkarni: Dept of PharmacologyMegha Kulkarni FPS PES UniversityNo ratings yet